Sacral Plexus & Sciatic Nerve: Anatomy & Surgical Approach
Key Takeaway
The sciatic nerve, the largest peripheral nerve in the human body, arises from the sacral plexus (L4-S3). It is highly susceptible to injury from trauma, hip dislocations, and iatrogenic causes. Surgical management requires a meticulous approach through the posterior thigh and gluteal region. This guide details the anatomical landmarks, step-by-step surgical exposure, and postoperative protocols necessary for optimal sciatic nerve repair and neurolysis.
INTRODUCTION TO THE SACRAL PLEXUS AND SCIATIC NERVE
The sacral plexus and its terminal branch, the sciatic nerve, represent the most critical neurological structures governing the motor and sensory function of the lower extremity. Analogous in its clinical importance to the brachial plexus in the upper extremity, the sacral plexus is a complex arborization of nerve roots that demands profound anatomical respect during pelvic, hip, and femoral surgeries.
Injuries to these structures—whether through high-energy trauma, penetrating wounds, or iatrogenic mechanisms—result in devastating functional deficits, including foot drop, loss of plantar flexion, and profound sensory neuropathy that can lead to chronic ulceration. This comprehensive masterclass delineates the intricate surgical anatomy, biomechanical implications, clinical evaluation, and step-by-step operative management of sacral plexus and sciatic nerve lesions.
SURGICAL ANATOMY OF THE SACRAL PLEXUS
The sacral plexus is formed by the anterior primary rami of L5, S1, S2, and S3. Furthermore, the anterior primary ramus of L4 contributes a substantial branch that joins with L5 to form the lumbosacral trunk, which descends into the pelvis over the sacral ala to join the sacral roots.
A segment of S4 joins a segment of S3 to form the pudendal nerve. Anatomists variably classify the pudendal nerve as part of the sacral plexus, a distinct pudendal plexus, or the superior aspect of the coccygeal plexus.
As the anterior primary rami converge, they systematically split into anterior and posterior divisions:
- Posterior Divisions: The trunk formed by the posterior divisions gives rise to the superior and inferior gluteal nerves and proceeds toward the greater sciatic notch to become the common peroneal part of the sciatic nerve.
- Anterior Divisions: The trunk formed by the anterior divisions becomes the tibial part of the sciatic nerve, proceeding toward the sciatic notch.
Intrapelvic and Gluteal Branches
Before exiting the pelvis, the sacral plexus gives off several smaller motor branches that are rarely of primary surgical concern but are anatomically significant. These supply the quadratus femoris, obturator internus, superior gemellus, and piriformis muscles.
More critical are the major branches that dictate gluteal function and posterior thigh sensation:
- Posterior Femoral Cutaneous Nerve (S1, S2, S3): Often referred to as the "small sciatic nerve," this relatively large sensory nerve leaves the sciatic notch medial to the sciatic trunk. It lies just deep to the deep fascia (fascia lata) as it courses distally down the midline of the posterior thigh, roughly overlying the sciatic trunk. It provides critical sensory innervation to the skin of the entire posterior thigh and the popliteal fossa.
- Superior Gluteal Nerve (L4, L5, S1): Exits the sciatic notch proximal to the piriformis muscle. It supplies the gluteus medius, gluteus minimus, and tensor fasciae latae. These muscles are the primary abductors and internal rotators of the hip, essential for maintaining a level pelvis during the stance phase of gait (preventing Trendelenburg gait).
- Inferior Gluteal Nerve (L5, S1, S2): Exits the sciatic notch distal to the piriformis, accompanying the sciatic nerve. It exclusively supplies the gluteus maximus, the primary extensor of the hip.
Clinical Pearl: Paralysis of the gluteus maximus secondary to inferior gluteal nerve injury results in profound difficulty rising from a squatting or sitting position, and severe impairment when ascending stairs or walking up a slope.
SURGICAL ANATOMY OF THE SCIATIC NERVE
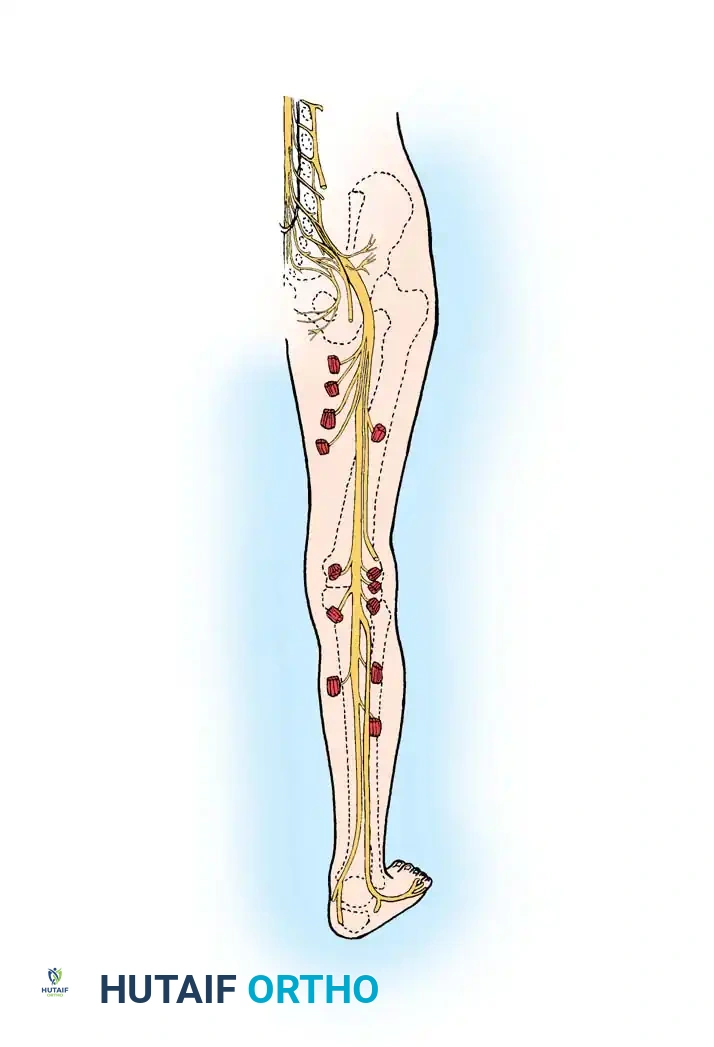
The sciatic nerve is the largest peripheral nerve in the human body, boasting a transverse diameter of 2 to 2.5 cm at its origin. It is composed of fibers from L4, L5, S1, S2, and S3.
It exits the pelvis through the greater sciatic notch, typically emerging inferior to the piriformis muscle. At this proximal level, the large trunk is already anatomically distinct, easily separable into its common peroneal part laterally and its tibial part medially.
Frequently, along the medial aspect of the main trunk, a smaller distinct segment—the nerve to the hamstrings—is visible and can be easily dissected. This branch sends motor fibers medially to supply the adductor magnus (ischial head), semimembranosus, semitendinosus, and the long head of the biceps femoris. Conversely, a branch leaves the common peroneal part of the trunk laterally to supply the short head of the biceps femoris.
Course and Distribution
The sciatic nerve descends deep to the gluteus maximus to the level of the inferior gluteal fold. Here, it lies in the anatomical depression between the ischial tuberosity medially and the greater trochanter laterally.
Distal to this level, it follows a more superficial course beneath the long head of the biceps femoris to the distal third of the thigh. While coursing through the posterior thigh, its upper part supplies vital articular branches to the posterior capsule of the hip joint. Just proximal to the popliteal fossa, the sciatic nerve formally divides into its two large terminal branches:
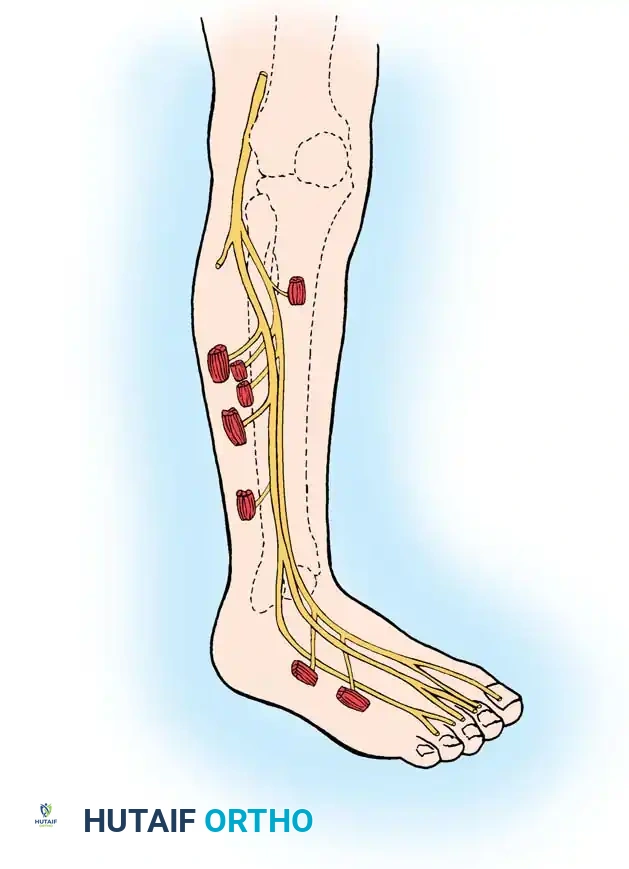
1. Common Peroneal Nerve: Deviates laterally, following the medial border of the biceps femoris toward the fibular head.
2. Tibial Nerve: Continues distally in the midline of the limb, bisecting the popliteal fossa.
MECHANISMS OF INJURY
The sacral plexus and sciatic nerve are vulnerable to a variety of traumatic and iatrogenic insults. The sacral plexus may be compressed by pelvic neoplasms, during labor and delivery (especially with forceps utilization), or injured during sacral fractures and severe sacroiliac joint dislocations.
The sciatic nerve is most frequently injured by:
* High-Energy Trauma: Gunshot wounds to the thigh or buttock, and penetrating lacerations.
* Orthopaedic Trauma: Posterior dislocations and fracture-dislocations of the hip. The peroneal division is tethered at the sciatic notch and the fibular head, making it significantly more susceptible to stretch injuries during posterior hip dislocations than the tibial division.
* Iatrogenic Causes: Intramuscular injections into the buttock (if placed outside the safe upper-outer quadrant) and surgical retractors during total hip arthroplasty (THA).
* Chronic Compression: Compression caused by anatomical variations (e.g., piriformis syndrome) or by wear debris/granulomas from long-standing total hip replacements, as described by Crawford et al.
Surgical Warning: In the setting of a complete division of the proximal one-third of the sciatic nerve (e.g., from a gunshot wound), the semimembranosus and semitendinosus are rarely paralyzed because their motor branches often arise very proximally, sometimes directly from the plexus.
CLINICAL EXAMINATION AND DIAGNOSTICS
Accurate clinical evaluation requires a systematic assessment of the motor and sensory domains innervated by the tibial and peroneal components.
Motor Examination
- Tibial Component: Innervates the hamstrings, gastrocsoleus complex, tibialis posterior, and the long flexors of the toes. Profound weakness here results in an inability to plantarflex the foot, invert the foot, or flex the toes.
- Peroneal Component: Innervates the tibialis anterior, long extensors of the toes (deep peroneal nerve), and the peroneus longus and brevis (superficial peroneal nerve). Injury results in a classic "foot drop" (equinus deformity) and an inability to evert the foot.
An extremity with a completely divided sciatic nerve will rapidly develop an equinus deformity, clawing of the toes, and severe muscle atrophy.
Sensory Examination and Autonomous Zones
Sensory loss mapping is critical for localizing the lesion.
* Peroneal Nerve Involvement: Sensory loss is primarily over the lateral aspect of the leg and the dorsum of the foot.
* Tibial Nerve Involvement: Sensory deficit is primarily over the plantar aspect of the foot.
Pitfall: Anesthesia on the plantar surface of the foot is devastating. Without protective sensation, patients are at an exceptionally high risk of developing chronic, limb-threatening neuropathic ulcerations.

The autonomous zone of the sciatic nerve includes the area over the metatarsal heads, the heel, the lateral and posterior aspects of the sole, the dorsum of the foot as far medially as the second metatarsal, and a narrow strip up the lateral aspect of the leg.
Diagnostic Adjuncts
- Electromyography (EMG): Highly valuable for evaluating the extent of denervation and monitoring reinnervation. The sciatic nerve is too deeply located to stimulate easily in situ via surface electrodes.
- Skin Resistance / Iodine Starch Test: Helpful for evaluating sudomotor (sympathetic) function, which is lost in complete nerve transections.
- Tinel's Sign (Percussion): In multiple penetrating wounds, percussing along the anatomical course of the nerve to the point where distal tingling is most pronounced is a highly accurate method of locating the exact zone of injury.
SURGICAL INDICATIONS AND TIMING
The decision to explore the sciatic nerve depends heavily on the mechanism of injury:
1. External Compression: If injury is caused by a poorly fitted cast or unusual posture, the cause must be removed immediately. If compression has been of long duration, exploration and neurolysis may be warranted, though the prognosis remains guarded.
2. Fractures and Dislocations: If complete division complicates a hip dislocation or pelvic fracture, early exploration assists in determining the extent of injury. If it complicates a femoral shaft fracture with no signs of clinical or EMG recovery after 3 to 4 months, exploration is justified.
3. Penetrating Trauma: Sharp lacerations or proximal buttock penetrating injuries warrant early exploration and primary repair. Delaying repair in proximal lesions means the distal musculature remains denervated for an extended period, leading to irreversible motor endplate fibrosis.
Critical Limit of Delay: Zachary established that useful motor and sensory recovery is not to be anticipated if a sciatic nerve injured high in the thigh or buttock is not sutured before 12 to 15 months post-injury.
SURGICAL APPROACH TO THE SCIATIC NERVE (TECHNIQUE 59-15)
The sciatic nerve can be expansively exposed from its emergence at the greater sciatic notch down to its bifurcation in the popliteal fossa.
Positioning and Incision
The patient is placed in the prone position. The entire hemipelvis, thigh, and leg are prepped and draped free to allow for intraoperative manipulation of the hip and knee joints.
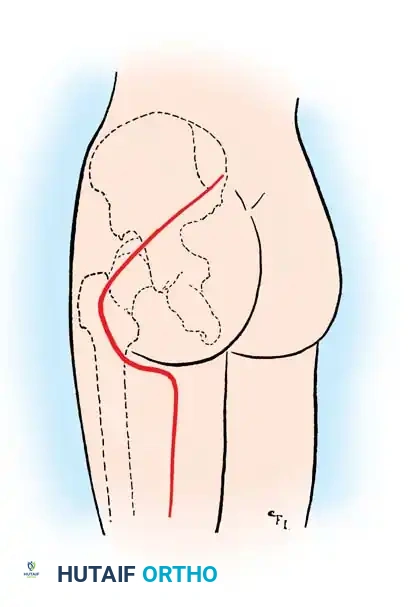
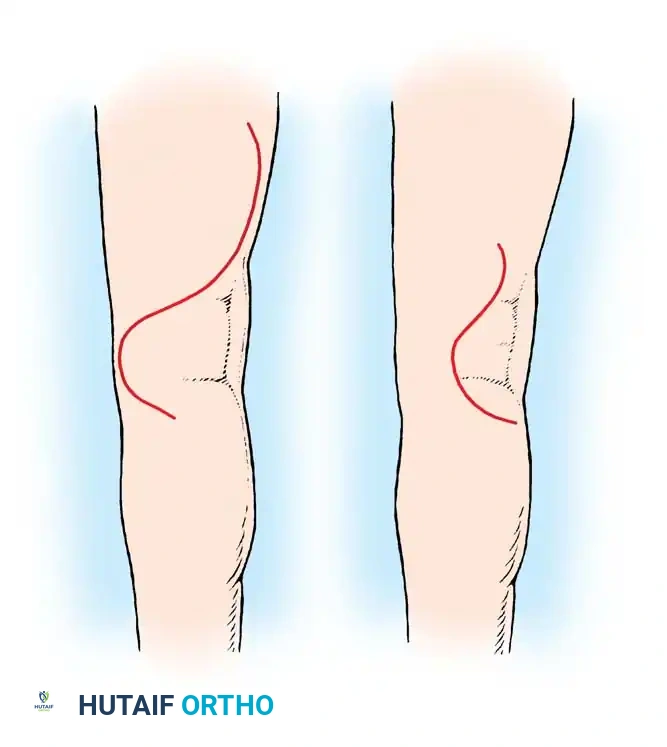
For injuries near the sciatic notch, begin the incision at the posterior superior iliac spine (PSIS). Carry it diagonally, distally, and laterally in the direction of the fibers of the gluteus maximus to a point approximately 2.5 cm medial to the greater trochanter.
Curve the incision medially, distal to the gluteal fold, reaching the midpoint of the fold. Finally, extend the incision distally along the posterior aspect of the thigh to a point 10 cm proximal to the skin creases of the popliteal fossa.
Proximal Exposure (Gluteal Region)
- Deepen the proximal part of the incision through the thick gluteal fascia.
- Bluntly separate the coarse muscle fibers of the gluteus maximus as far laterally as the greater trochanter.
- Incise the fascia of the thigh longitudinally down to the gluteal fold.
- Detach the insertion of the distal fibers of the gluteus maximus from the iliotibial band and the gluteal tuberosity of the femur.
- Reflect the gluteus maximus medially. This muscle flap retains its neurovascular pedicle (inferior gluteal nerve and artery) and exposes the sciatic nerve as far proximally as the piriformis muscle.
- If the nerve is injured at the notch, the piriformis muscle may be sacrificed (tenotomized and reflected) to expose the nerve as it emerges from the pelvis.
- If intrapelvic exposure is required, a portion of the posterior sacrum and greater sciatic notch can be removed with a rongeur.
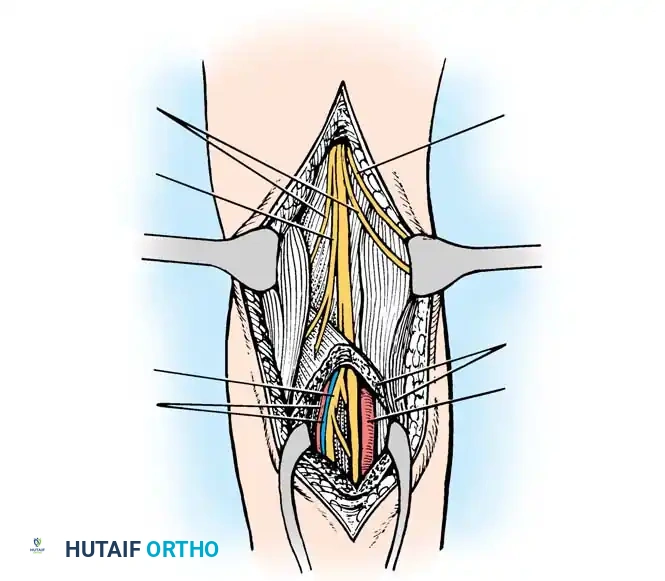
Distal Exposure (Posterior Thigh)
When the injury is isolated to the thigh, the proximal gluteal incision is unnecessary. Begin at the gluteal fold and continue distally along the posterior thigh.
- Open the deep fascia (fascia lata) longitudinally in line with the skin incision.
- Protect the posterior femoral cutaneous nerve, which lies immediately deep to the deep fascia and superficial to the hamstrings.
- In the proximal thigh, identify the long head of the biceps femoris. Retract it medially to identify the sciatic nerve lying on the adductor magnus.
METHODS OF CLOSING NERVE GAPS
Primary tension-free neurorrhaphy is the gold standard but is often impossible in high-energy trauma with zone of injury resection.
Mobilization and Positioning:
Extensive proximal and distal mobilization of the nerve, including separating its two divisions, combined with flexing the knee and hyperextending the hip, can allow closure of a gap of up to 15 cm.
Bone Shortening:
When the femur is concomitantly fractured and the sciatic nerve divided, it is imperative to operate on the nerve before the femur unites. If the knee stiffens, it becomes impossible to flex it enough to close large defects. Resecting a part of the femur to shorten the limb may be justified to close the nerve gap in the presence of a fracture. However, in the absence of a femoral fracture, the intact femur should never be shortened solely for nerve repair.
Nerve Grafting:
If a tension-free primary repair cannot be achieved through mobilization and positioning, autogenous interfascicular nerve grafting (typically utilizing the sural nerve) is the standard of care, particularly in young patients.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Following primary neurorrhaphy under tension (utilizing joint positioning), the limb must be strictly immobilized to prevent catastrophic rupture of the repair.
- Immobilization: Apply a double spica cast extending from the nipple line to the toes on the affected side, and to above the knee on the contralateral side. The affected hip is extended, and the knee is flexed to relieve all tension on the sciatic nerve.
- Wound Care: The cast is windowed to allow removal of sutures at approximately 10 to 14 days.
- Bracing: At 6 weeks, the spica cast is removed. A long leg brace with an adjustable drop-lock knee hinge is applied. The knee is extended gradually (e.g., 10 degrees per week) over the subsequent 6 weeks to slowly stretch the nerve without disrupting the intraneural microvasculature.
- Rehabilitation: Aggressive physical therapy is initiated to restore joint mobility and prevent contractures. Once knee extension is complete, an ankle-foot orthosis (AFO) is applied to compensate for foot drop and prevent equinus contracture while awaiting reinnervation.
Note: If autogenous nerve grafting was utilized, extreme joint positioning is unnecessary as the repair is inherently tension-free. A standard spica cast is used for soft tissue rest, but early motion can be initiated once the surgical wounds have healed.
OUTCOMES AND PROGNOSIS
The prognosis following sciatic nerve repair is heavily dependent on the level of injury and the age of the patient.
According to Sunderland's extensive data, the results of sciatic nerve suture are generally poor for distally innervated muscles (e.g., intrinsic foot muscles, peroneals). This is due to:
* Extensive retrograde neuronal degeneration.
* Intraneural intermixing of regenerating fibers, leading to a loss of somatotopic fiber localization.
* Irreversible degenerative fibrotic changes in the distal muscles, which must remain denervated for the prolonged time it takes for axonal regeneration (growing at approximately 1 mm per day) to reach them from the proximal thigh.
Significant motor recovery is typically only expected in the proximally innervated muscles, specifically the hamstrings and the gastrocsoleus complex. If sensory recovery occurs in the plantar aspect of the foot, it is usually only of a protective nature (S3 level), which is nonetheless critical for preventing neuropathic ulceration.
In a landmark series by Delaria et al. evaluating 22 surgically treated sciatic lesions:
* Neurolysis (13 patients): 5 achieved excellent results (complete muscle recovery), 7 were good, and 1 was poor.
* Nerve Grafting (9 patients): 4 achieved excellent results, 4 were good, and 1 was poor.
These results underscore that while distal fine motor function is rarely restored, protective sensation and proximal stability can be reliably achieved with meticulous microsurgical technique and rigorous postoperative rehabilitation.
📚 Medical References
- sciatic nerve palsy in total hip arthroplasty, Clin Orthop Relat Res 218:136, 1987.
- Eggli S, Hankemayer S, Müller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip, J Bone Joint Surg 81B:843, 1999.
- Lazarides MK, Arvanitis DP, Dayantas JN: Iatrogenic arterial trauma associated with hip joint surgery: an overview, Eur J Vasc Surg 5:549, 1991.
- Navarro RA, Schmalzried TP, Amstutz HC, et al: Surgical approach and nerve palsy in hip arthroplasty, J Arthroplasty 10:1, 1995.
- Nercessian OA, Gonzalez EG, Stinchfi eld FE: The use of somatosensory evoked potential during revision or reoperation for total hip arthroplasty, Clin Orthop Relat Res 243:138, 1989.
- Nercessian OA, Piccoluga F, Eftekhar NS: Postoperative sciatic and femoral nerve palsy with reference to leg lengthening and medialization/lateralization of the hip joint following total hip arthroplasty, Clin Orthop Relat Res 304:165, 1994.
- Schmalzried TP, Amstutz HC, Dorey FJ: Nerve palsy associated with total hip replacement: risk factors and prognosis, J Bone Joint Surg 73A:1074, 1991.
- Shoenfeld NA, Stuchin SA, Pearl R, et al: The management of vascular injuries associated with total hip arthroplasty, J Vasc Surg 11:549, 1990.
- Siebenrock KA, Rösler KM, Gonzalez E, et al: Intraoperative electromyography of the superior gluteal nerve during lateral approach to the hip for arthroplasty: a prospective study of 12 patients, J Arthroplasty 15:867, 2000.
- Silbey MB, Callaghan JJ: Sciatic nerve palsy after total hip arthroplasty: treatment by modular neck shortening, Orthopedics 14:351, 1991.
- Simmons C, Izant TH, Rothman RH, et al: Femoral neuropathy following total hip arthroplasty: anatomic study, case reports, and literature review, J Arthroplasty 6(suppl):59, 1991.
- Leg-Length Discrepancy Bose WJ: Accurate limb-length equalization during total hip arthroplasty, Orthopedics 23:433, 2000.
- Edeen J, Sharkey PF, Alexander AH: Clinical signifi cance of leg-length inequality after total hip arthroplasty, Am J Orthop 4:347, 1995.
- Goodman SB, Huene DS, Imrie S: Preoperative templating for the equalization of leg lengths in total hip arthroplasty, Contemp Orthop 24:703, 1992.
- Knight JL, Atwater RD: Preoperative planning for total hip arthroplasty, J Arthroplasty 7:403, 1992.
- Love BRT, Wright K: Leg length discrepancy after total hip joint replacement, J Bone Joint Surg 65B:103, 1983.
- Parvizi J, Sharkey PF, Bissett GA, et al: Surgical treatment of
You Might Also Like

