Comprehensive Introduction and Patho-Epidemiology
While flexible pes planus is a common, often asymptomatic condition that rarely necessitates surgical intervention, rigid pes planus frequently produces significant biomechanical dysfunction and pain, justifying operative management. The etiology of a rigid flatfoot deformity is highly diverse, encompassing a spectrum of congenital, developmental, and acquired pathologies. Congenital vertical talus represents the most severe manifestation of rigid pes planus; however, because it is typically diagnosed and treated in infancy via serial casting and minimally invasive pinning, the focus of this definitive masterclass is on the pathologies encountered in older children, adolescents, and adults. Specifically, we will exhaustively analyze the symptomatic accessory navicular, idiopathic rigid pes planus, and tarsal coalition. Understanding the nuanced differences in the patho-epidemiology of these conditions is the critical first step in formulating an effective, patient-specific surgical algorithm.
Idiopathic rigid pes planus is a distinct clinical entity characterized by a stiff, painful flatfoot in the absolute absence of radiographic evidence of tarsal coalition or other structural anomalies. Luhmann, Rich, and Schoenecker described a highly specific cohort of patients presenting with this condition. Demographically, the overwhelming majority of these patients were in the 95th percentile for weight relative to their age, suggesting a mechanical overload phenomenon on the developing midfoot architecture. Clinically, they exhibited a profoundly externally rotated gait with an elevated foot-progression angle. In a parallel investigation, El Rassi, Riddle, and Kumar evaluated patients presenting with anterolateral hindfoot pain, reduced subtalar mobility, and negative plain radiographs, computed tomography (CT), and magnetic resonance imaging (MRI). The defining diagnostic feature in their cohort of 19 patients (23 feet) was a positive technetium-99m bone scan, which consistently demonstrated increased radiotracer uptake localized precisely at the middle facet of the subtalar joint. Surgical exploration revealed a hypervascular, thickened capsule and synovium in this region, indicating a localized, intense inflammatory capsulitis rather than a structural synostosis.
Tarsal coalition is frequently, though somewhat inaccurately, grouped strictly under congenital rigid pes planus. While the anatomical defect is undeniably present at birth, symptoms rarely manifest until the cartilaginous bar begins to ossify in late childhood or early adolescence, decreasing the compliance of the peritalar complex. Because the coalition is initially cartilaginous, the malleability of the peritalar complex prevents significant symptoms in early childhood. As the cartilage ossifies, profound hindfoot stiffness ensues, and the patient's ability to withstand the microtrauma of vigorous activity precipitously declines. Calcaneonavicular coalitions typically ossify and become symptomatic between 8 to 12 years of age, whereas talocalcaneal coalitions ossify later, typically between 12 to 16 years of age. The coalition interface may be bony (synostosis), cartilaginous (synchondrosis), or fibrous (syndesmosis). Paradoxically, incomplete coalitions (cartilaginous or fibrous) are often significantly more symptomatic due to painful micro-motion at the rigid, unyielding interface.
Genetically and embryologically, the etiology of tarsal coalition is almost irrefutably a failure of primitive mesenchyme to segment by cleavage in the 27- to 72-mm fetus, preventing the formation of the normal peritalar joint complex. This hypothesis was definitively demonstrated by Harris in 1955 through the meticulous dissection of fetal hindfeet. Genetically, tarsal coalition behaves as an autosomal dominant trait with reduced penetrance. Wray and Herndon documented a calcaneonavicular bar across three successive generations of men. Leonard's extensive radiographic survey of 31 index patients and 98 first-degree relatives revealed that an astonishing 39% of the relatives had tarsal coalitions. Strikingly, not a single one of the affected relatives had any history of foot complaints or peroneal spasticity, strongly suggesting that the true incidence of tarsal coalition in the general population is significantly higher than the traditionally quoted 1%, likely approaching 4-6%.
Detailed Surgical Anatomy and Biomechanics
Understanding the pathoanatomy and kinematics of the hindfoot is paramount for any reconstructive foot and ankle surgeon. The peritalar complex, comprising the subtalar, talonavicular, and calcaneocuboid joints, functions as a highly synchronized "mitered hinge" (as described by Inman), translating transverse plane rotation of the tibia into coronal and sagittal plane motion of the foot. A rigid deformity alters the normal force distribution across the midfoot and forefoot, leading to adaptive shortening of musculotendinous units, capsular contractures, and eventual degenerative joint disease if left untreated. When the subtalar joint is locked in valgus—whether by a coalition, an accessory navicular disrupting the posterior tibial tendon, or idiopathic capsulitis—the transverse tarsal joint unlocks, resulting in a profound loss of the medial longitudinal arch and a failure of the foot to become a rigid lever arm during the terminal stance phase of gait.
Historically, tarsal coalition, rigid pes planus, and peroneal muscle spasm were collectively termed "peroneal spastic pes planus." However, true spasticity—which is an upper motor neuron sign characterized by a velocity-dependent increase in muscle tone—is entirely absent in these patients. The "spasm" is actually an acquired, adaptive shortening of the musculotendinous units of the peroneal muscles. When an examiner applies an aggressive inversion stress to the foot, it elicits an unsustained three- or four-beat clonus; this is simply the physiological stretch reflex of a chronically shortened muscle belly. According to Lapidus, the relaxed position of the subtalar joint is valgus, which places the least mechanical strain on the talocalcaneal interosseous ligament. Through an ill-defined reflex mechanism, the peroneal muscles are stimulated to evert the hindfoot, effectively "decompressing" the subtalar joint. Over time, this everted position becomes fixed, leading to the classic rigid, valgus presentation.

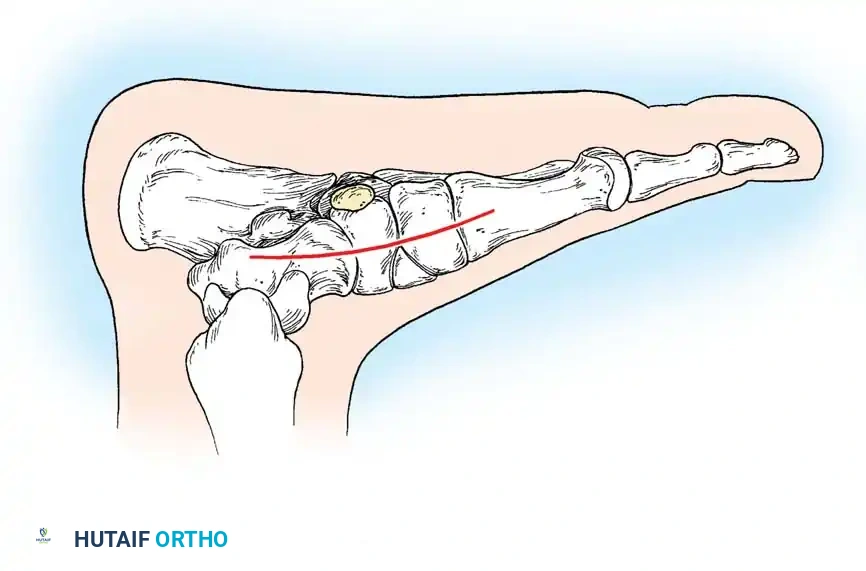
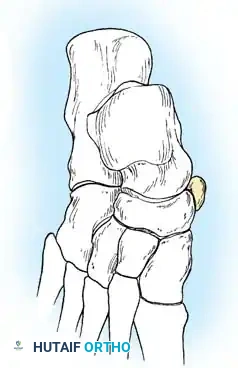
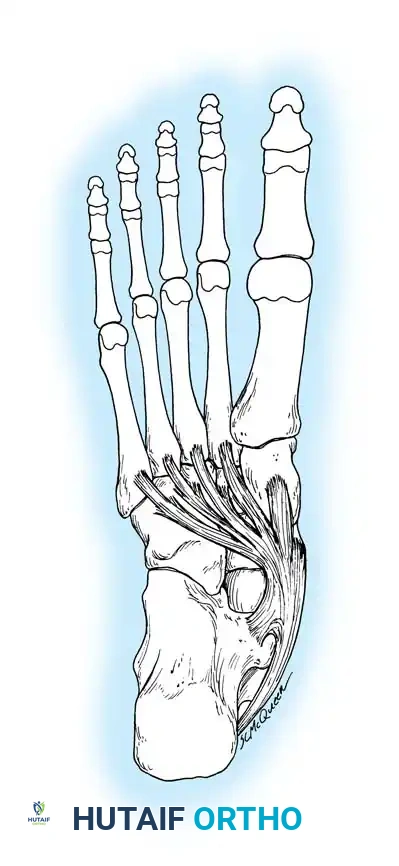
The accessory navicular (os naviculare) is a common accessory ossicle located adjacent to the medial tuberosity of the navicular, present in approximately 10-14% of the population. Lawson classified these into three distinct types: Type I is a small, round sesamoid bone within the posterior tibial tendon (PTT) substance; Type II is a larger, triangular ossicle connected to the navicular tuberosity by a 1-2 mm layer of fibrocartilage or hyaline cartilage (synchondrosis); and Type III is a solid bony fusion, resulting in a prominent cornuate navicular. Type II is the most frequently symptomatic variant. When symptomatic, it disrupts the normal insertion and mechanical advantage of the PTT. Instead of inserting firmly into the plantar aspect of the navicular, cuneiforms, and metatarsal bases to actively invert and plantarflex the midfoot, the PTT inserts proximally into the accessory ossicle. This proximal insertion effectively weakens the tendon's ability to act as a dynamic elevator of the medial longitudinal arch, contributing directly to medial arch collapse, spring ligament attenuation, and rigid pes planus.
In the context of tarsal coalitions, the specific anatomical location dictates the surgical approach and biomechanical consequence. The calcaneonavicular coalition bridges the anterior process of the calcaneus to the lateral and dorsolateral extra-articular surface of the navicular. It typically measures 1 to 2 cm in length and 1 to 1.2 cm in width, directly blocking the motion of the Chopart joint complex. The talocalcaneal coalition most commonly involves the middle facet, located directly superior to the sustentaculum tali. The flexor hallucis longus (FHL) tendon runs intimately beneath the sustentaculum tali, serving as a critical surgical landmark but also placing it at high risk for iatrogenic injury during middle facet coalition resections. The posterior facet is rarely involved, but its integrity is crucial; if a middle facet coalition is resected, the posterior facet must be capable of assuming the biomechanical load to prevent rapid subtalar arthrosis.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in rigid pes planus and tarsal coalition requires a meticulous synthesis of clinical symptomatology, failure of conservative measures, and precise radiographic staging. In patients with suspected idiopathic rigid pes planus, an Examination Under Anesthesia (EUA) is a critical diagnostic and prognostic tool. Luhmann et al. demonstrated that out of 13 patients, 9 experienced significant improvement in hindfoot motion under anesthesia, while 4 showed only partial improvement. This differentiates structural rigidity from severe musculotendinous guarding. A mobile hindfoot under EUA indicates that the rigidity is primarily driven by pain and muscle spasm; these patients often respond well to serial casting combined with subtalar corticosteroid injections. Conversely, persistent rigidity under EUA indicates fixed capsular or tendinous contractures, necessitating surgical release, osteotomy, or arthrodesis.
Surgical intervention for an accessory navicular (the Kidner procedure or its modifications) is strictly indicated for patients with refractory medial midfoot pain, localized tenderness over the ossicle, and a progressive collapse of the medial longitudinal arch that has failed at least 3 to 6 months of conservative management (including CAM boot immobilization, custom orthotics, and targeted physical therapy). For tarsal coalitions, resection is indicated in younger patients (typically under 16 years of age) who present with localized pain, recurrent ankle sprains, and rigid pes planus, provided there is no evidence of advanced degenerative joint disease in the adjacent hindfoot joints. For talocalcaneal coalitions specifically, resection is generally indicated if the coalition involves less than 50% of the posterior subtalar joint surface area and the heel is in neutral or only mild valgus alignment.
Contraindications must be rigorously respected to prevent catastrophic surgical failures. Absolute contraindications include active localized or systemic infection, severe peripheral vascular disease, and profound medical comorbidities precluding safe anesthesia. Relative contraindications for joint-sparing procedures (such as coalition resection or the Kidner procedure) include advanced patient age, severe fixed hindfoot valgus (which will not correct with simple resection), and established degenerative changes in the subtalar or talonavicular joints. In the presence of significant arthrosis or a talocalcaneal coalition encompassing greater than 50% of the joint surface, simple resection is contraindicated; these patients require primary subtalar or triple arthrodesis to achieve a stable, plantigrade, and pain-free foot.
| Clinical Pathology | Primary Surgical Indication | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Symptomatic Accessory Navicular | Refractory pain > 6 months, arch collapse, failed orthotics. | Active infection, non-ambulatory status. | Asymptomatic incidental finding, generalized hyperlaxity without localized pain. |
| Calcaneonavicular Coalition | Rigid flatfoot, lateral pain, failed casting, no adjacent DJD. | Advanced talonavicular or calcaneocuboid arthrosis. | Severe fixed structural valgus requiring concurrent osteotomy. |
| Talocalcaneal Coalition | Middle facet involvement < 50%, failed conservative care, age < 16. | Posterior facet arthrosis, coalition > 50% of joint area. | Severe hindfoot valgus > 15 degrees, older patient age. |
| Idiopathic Rigid Pes Planus | Fixed contracture confirmed via EUA, failed serial casting. | Mobile hindfoot under EUA (treat conservatively first). | BMI > 40 (high risk of osteotomy/arthrodesis failure). |
Patient-specific factors also play a massive role in surgical decision-making. High Body Mass Index (BMI), as noted in the Luhmann cohort, places immense stress on soft-tissue reconstructions and osteotomies, increasing the risk of loss of correction or nonunion. Furthermore, postoperative compliance is paramount; procedures like the Kidner or complex osteotomies require prolonged periods of non-weight-bearing immobilization. If a patient or their family demonstrates an inability to adhere to strict postoperative protocols, joint-sparing or soft-tissue procedures may be contraindicated in favor of more robust, inherently stable arthrodesis constructs.
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive pre-operative planning begins with an exhaustive clinical and radiographic evaluation. Clinically, the surgeon must perform a heel rise test to evaluate posterior tibial tendon function and hindfoot inversion. The Hubscher maneuver (passive dorsiflexion of the hallux) should be utilized to assess the flexibility of the medial longitudinal arch; in rigid pes planus, the arch will fail to reconstitute. The Coleman block test is essential to differentiate between a forefoot-driven and a hindfoot-driven deformity, guiding whether a medial column procedure (e.g., Cotton osteotomy) is required in conjunction with hindfoot correction. A thorough neurovascular examination is mandatory, particularly documenting the status of the sural and saphenous nerves, which are at high risk during lateral and medial surgical approaches, respectively.
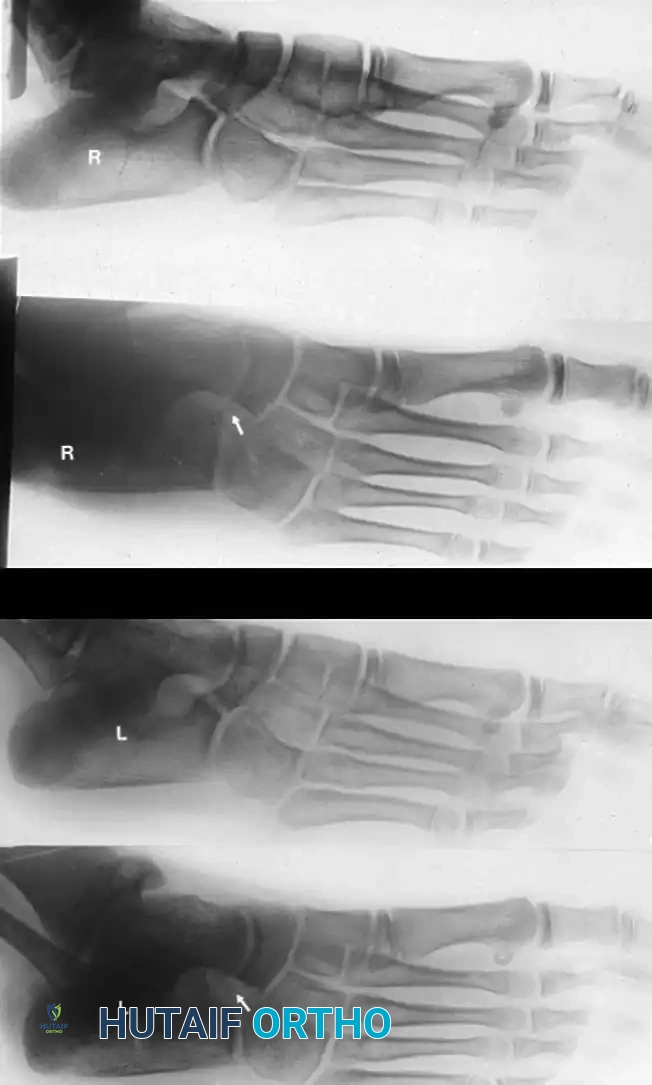
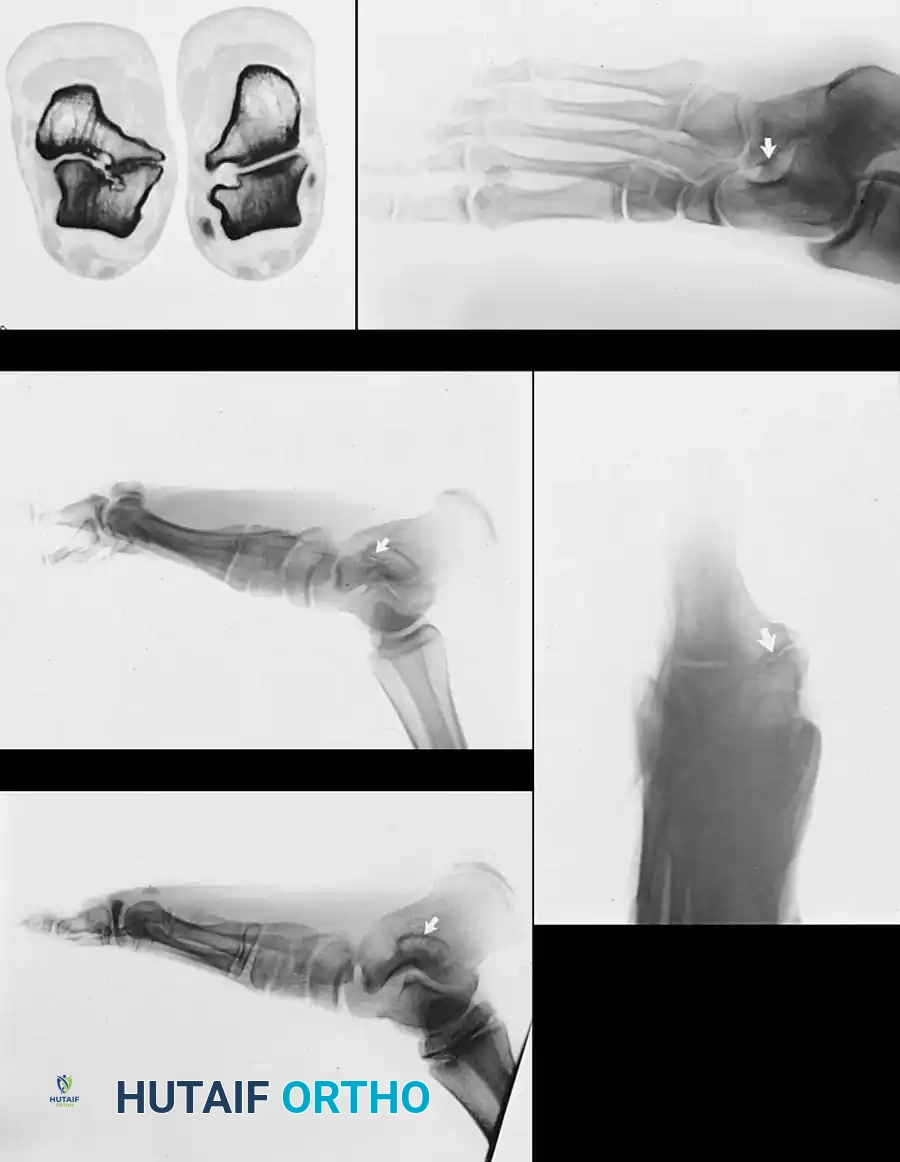
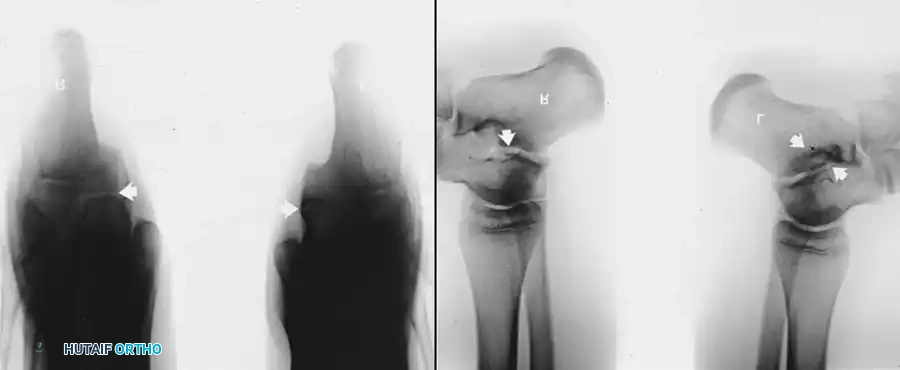
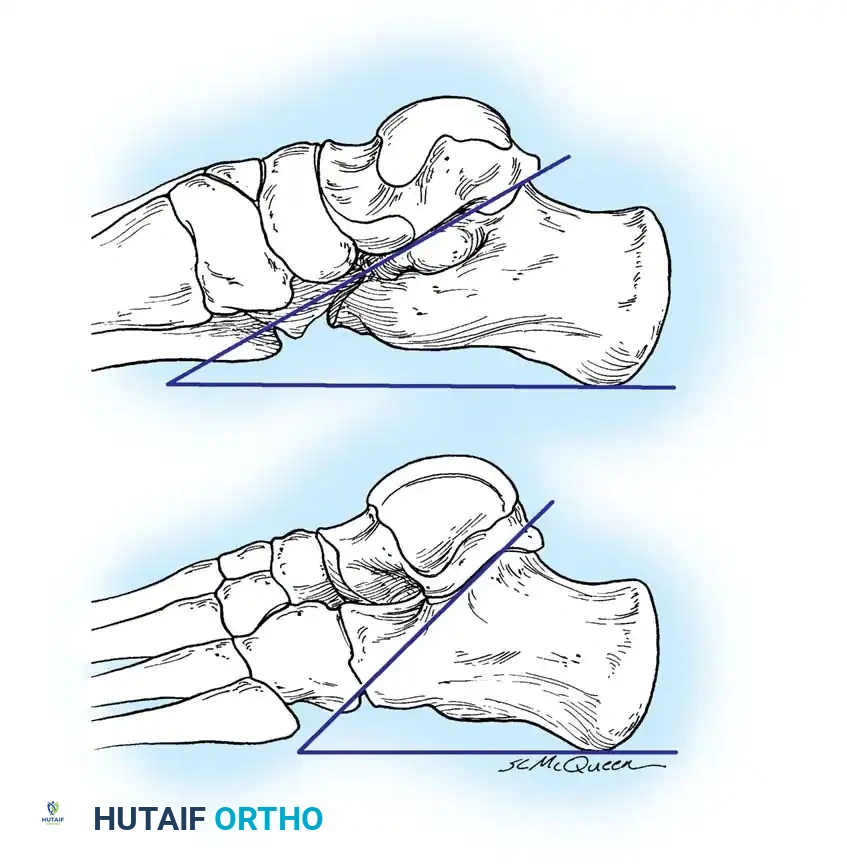
Radiographic imaging remains the cornerstone of preoperative templating. Standard weight-bearing anteroposterior (AP), lateral, and mortise views of the foot and ankle are required. On the lateral view, the surgeon must look for the "C-sign" (a continuous C-shaped outline formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali), which is highly indicative of a talocalcaneal coalition. Talar beaking, a traction osteophyte at the dorsal talonavicular joint resulting from altered kinematics, is another secondary sign. For calcaneonavicular coalitions, the 45-degree lateral oblique radiograph is the absolute gold standard. The abnormal bar extends from the anterior process of the calcaneus dorsally and medially to the navicular. The surgeon must be cautious of the "Pseudocoalition" pitfall: in older adolescents and adults, a prominent anterior tuberosity of the calcaneus may overlap the navicular on standard views, creating the illusion of a coalition.
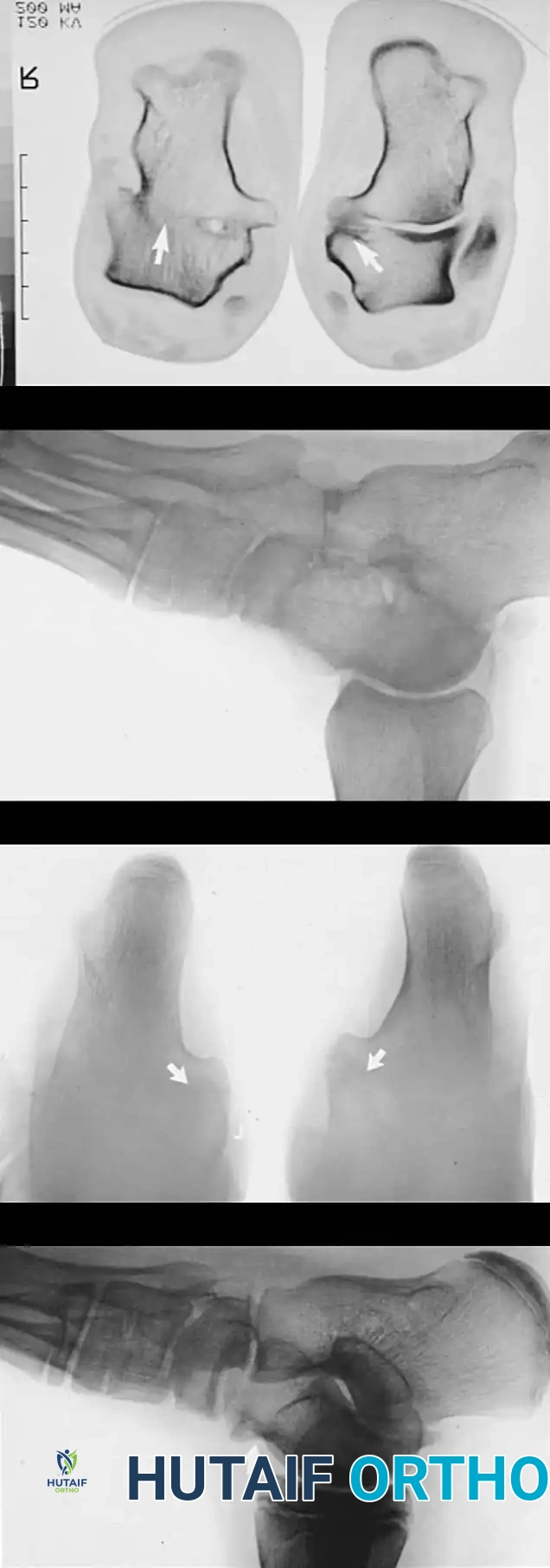

In modern orthopedic practice, advanced cross-sectional imaging is universally utilized for surgical planning, particularly for talocalcaneal coalitions and complex idiopathic deformities. A fine-cut CT scan (1-2 mm slices) with multiplanar reconstruction is invaluable. Coronal CT images are critical for calculating the exact surface area of a talocalcaneal coalition relative to the normal posterior facet, directly dictating whether a resection or an arthrodesis is indicated. MRI is highly sensitive for detecting fibrous or cartilaginous coalitions (synchondroses/syndesmoses) that may appear normal on plain radiographs. Furthermore, MRI can identify bone marrow edema adjacent to the coalition interface, confirming that the coalition is the acute source of the patient's pain.
Patient positioning is dictated by the specific pathology and planned surgical approach. For the Kidner procedure, resection of a middle facet talocalcaneal coalition, or medializing calcaneal osteotomies, the patient is positioned supine with a bump placed under the ipsilateral hip. This internally rotates the leg, bringing the medial aspect of the foot and ankle into direct view. For the resection of a calcaneonavicular coalition or lateral column lengthening procedures, the patient is positioned in the lateral decubitus or "sloppy lateral" position, allowing unhindered access to the sinus tarsi and lateral calcaneal wall. A well-padded thigh tourniquet is applied in all cases to ensure a bloodless surgical field, which is absolutely critical for identifying delicate neurovascular structures like the medial calcaneal nerve branches and the flexor hallucis longus tendon.
Step-by-Step Surgical Approach and Fixation Technique
The Kidner Procedure for the Accessory Navicular
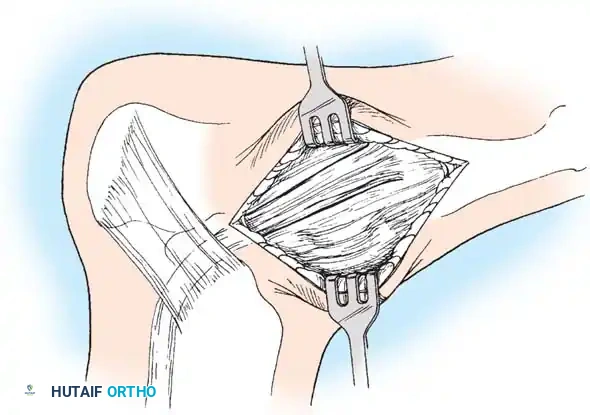
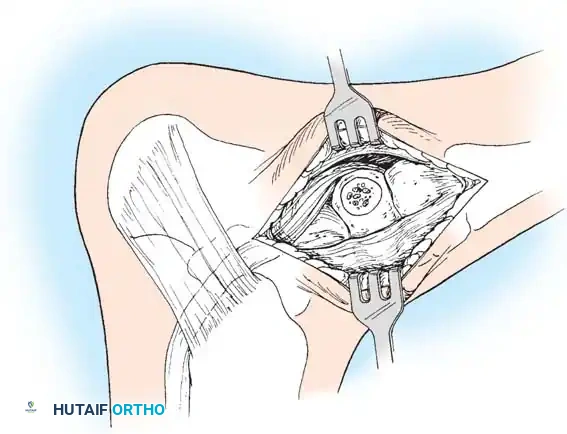
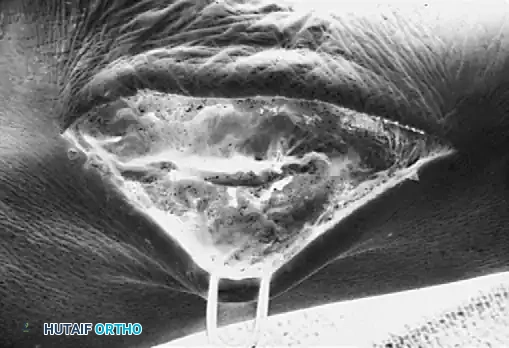
The Kidner Procedure involves the meticulous excision of the accessory navicular and the transposition/advancement of the PTT to restore its function as a dynamic elevator of the medial longitudinal arch. The skin incision begins 1 to 1.5 cm inferior and distal to the tip of the medial malleolus, arching slightly dorsalward over the medial prominence of the accessory navicular, and sloping distally to the base of the first metatarsal. Subcutaneous dissection must be performed with extreme care to identify and ligate the plantar communicating branches of the saphenous venous system while strictly protecting the terminal branches of the saphenous nerve.
The posterior tibial tendon is identified as it approaches the accessory navicular. The surgeon must identify the dorsal and plantar margins of the PTT approximately 2 cm proximal to the accessory navicular, exposing the tendon distally down to the bone. A critical surgical warning: it is imperative to expose the entire tendon without disturbing the portion extending plantarward toward its multiple insertions on the cuneiforms and metatarsal bases. Preserving these plantar slips maintains the structural integrity of the midfoot. Using sharp dissection, the accessory navicular is meticulously shelled out from the substance of the posterior tibial tendon. Attempt to leave a microscopic sliver of bone within the tendon to enhance subsequent bone-to-tendon healing.


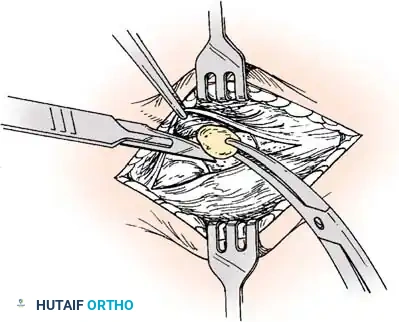

The medial prominence of the main navicular is then resected using a sharp osteotome so that it is flush with the medial border of the first cuneiform. A rongeur and rasp are utilized to smooth the cortical edges, preventing future bursa formation. The PTT is then advanced and sutured to the apex of the medial longitudinal arch. This is achieved by passing heavy non-absorbable sutures (e.g., #2 FiberWire) through drill holes placed in the center of the navicular and tying them dorsally, or by utilizing modern suture anchors. During knot tying, the midfoot and forefoot must be held in a cavovarus position to biomechanically reduce the talonavicular joint and reestablish the medial arch.


Resection of Tarsal Coalitions and Idiopathic Deformity Management
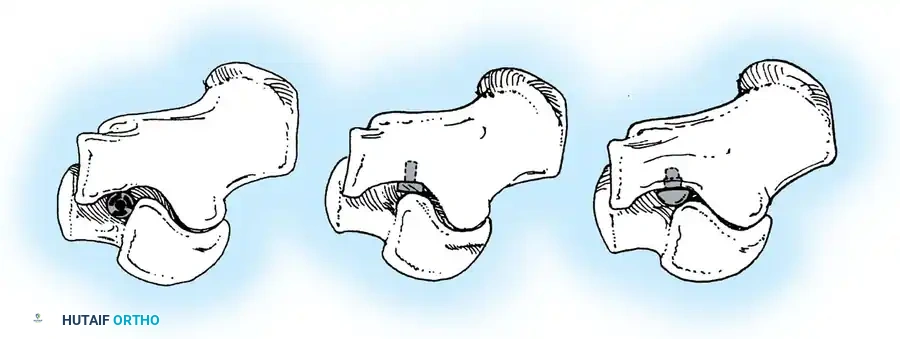
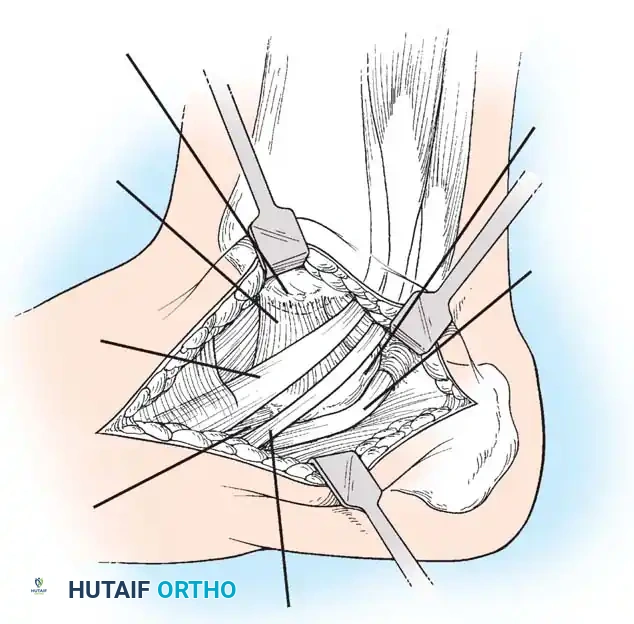
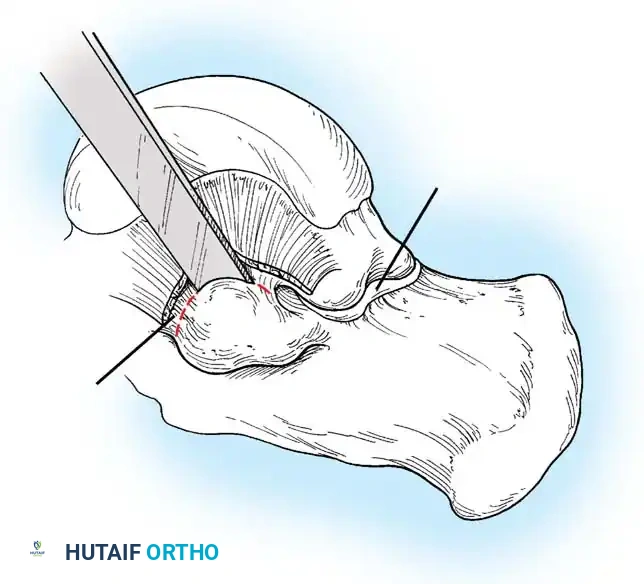
For a calcaneonavicular coalition, a lateral Ollier incision is utilized over the sinus tarsi. The extensor digitorum brevis (EDB) muscle belly is identified and reflected distally. The coalition is identified, and a rectangular block of bone (at least 1.5 cm wide) is aggressively resected using osteotomes and rongeurs until normal hyaline cartilage is visualized on the talar head and cuboid. To prevent recurrence, the EDB muscle belly or a free fat graft is interposed into the defect and secured with absorbable sutures.
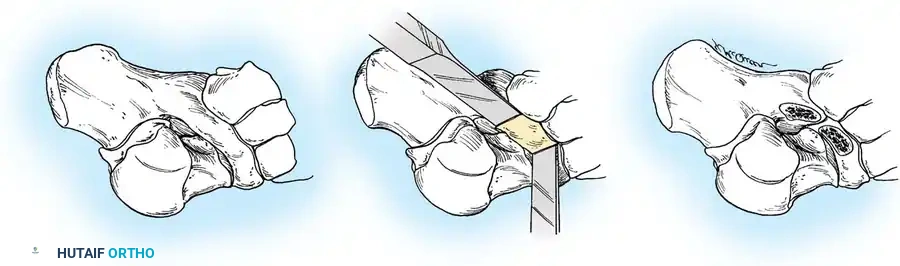
For a talocalcaneal coalition, a medial approach is utilized, centered over the sustentaculum tali. The flexor retinaculum is incised, and the FHL and flexor digitorum longus (FDL) tendons are identified and retracted. The coalition, typically located at the middle facet, is resected using a high-speed burr and osteotomes. The resection must extend laterally until the normal posterior facet and the interosseous ligament are visualized. A split portion of the FHL tendon, bone wax, or a massive fat graft is interposed to prevent synostosis recurrence.
In cases of idiopathic rigid pes planus that remain rigid under EUA, the surgeon must address the fixed contractures. This often requires a peroneal fractional lengthening to release the lateral tether. If structural realignment is necessary due to chronicity, a medializing calcaneal osteotomy is performed via a lateral approach, shifting the posterior tuberosity 10 mm medially to restore the mechanical axis, fixed with one or two large fragment cannulated screws. In severe, refractory cases with established arthrosis, a subtalar or triple arthrodesis remains the definitive salvage procedure.
Complications, Incidence Rates, and Salvage Management
The surgical management of rigid pes planus and tarsal coalitions is fraught with potential complications, demanding meticulous surgical technique and vigilant postoperative care. The inherent risks of midfoot and hindfoot surgery include delayed wound healing, superficial and deep infections, and deep vein thrombosis (DVT). Wound dehiscence is particularly common in medial approaches for the Kidner procedure or talocalcaneal coalition resection due to the thin soft-tissue envelope and the tension placed on the skin when the foot is immobilized in an inverted, cavovarus position. Meticulous, tension-free layered closure and strict elevation in the immediate postoperative period are mandatory to mitigate this risk.
Recurrence of a tarsal coalition is a devastating complication, most frequently resulting from inadequate primary resection rather than true biological recurrence. If a calcaneonavicular or talocalcaneal bar is not resected widely enough (failing to expose normal articular cartilage margins) or if an interpositional graft (EDB, fat, or bone wax) is not adequately secured, osteogenic factors will rapidly bridge the gap. The incidence of symptomatic recurrence ranges from 5% to 15% in the literature. Salvage management for a recurrent coalition depends on the joint status; if the adjacent joints remain pristine, a revision wide resection can be attempted. However, if secondary arthrosis has developed, a definitive subtalar or triple arthrodesis is required.
Failure of the posterior tibial tendon or persistent flatfoot deformity following a Kidner procedure occurs when the tendon is under-advanced, fails to biologically integrate into the navicular, or when the underlying deformity was primarily structural rather than soft-tissue driven. In these instances, the patient continues to experience medial arch collapse and pain. Salvage management typically involves a flexor digitorum longus (FDL) tendon transfer to the navicular, augmented with a medializing calcaneal osteotomy to protect the transfer by restoring the hindfoot mechanical axis.
Neurological complications are also a significant concern. The sural nerve is at high risk during lateral approaches for calcaneonavicular coalition resections or calcaneal osteotomies. The saphenous nerve and the medial calcaneal branches of the tibial nerve are vulnerable during medial approaches. Injury can lead to painful neuromas or Complex Regional Pain Syndrome (CRPS). Careful blunt dissection and retraction are essential.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Coalition Recurrence | 5% - 15% | Inadequate resection width, failure of interposition graft. | Revision wide resection vs. Subtalar/Triple Arthrodesis. |
| PTT Failure / Arch Collapse | 10% - 20% | Failure of tendon |
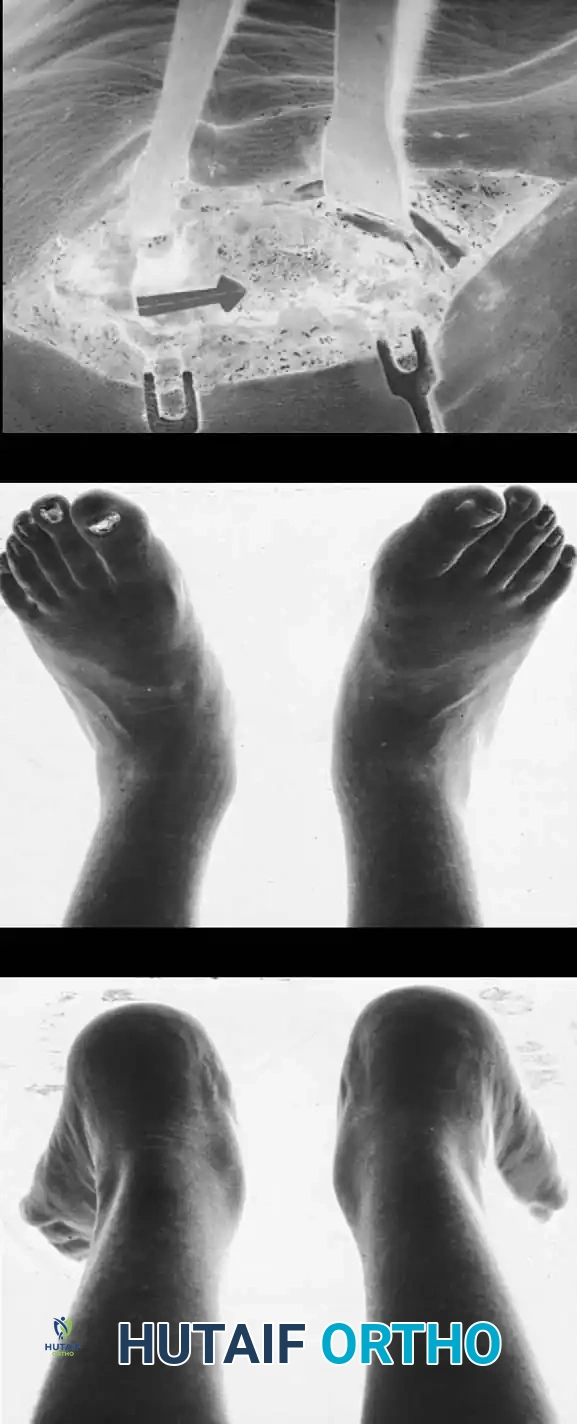
Clinical & Radiographic Imaging Archive