INTRODUCTION TO REVISION TOTAL HIP ARTHROPLASTY
The volume of primary total hip arthroplasties (THA) has grown exponentially over the past three decades. Concurrently, the expansion of indications to include younger, highly active patients has led to a dramatic increase in the incidence of revision procedures. Historically, revision THA accounted for approximately 17.5% of all hip arthroplasties performed in the United States, a figure that continues to evolve with the aging population and the survivorship curves of primary implants.
Failure of a primary THA can frequently be traced to technical errors during the index procedure, underscoring the critical importance of precision in primary arthroplasty. A meticulously executed index procedure remains the patient's best defense against future failure. Revision THA is inherently more complex than primary surgery, characterized by increased operative time, greater blood loss, and significantly higher rates of complications, including periprosthetic joint infection (PJI), thromboembolism, instability, nerve palsy, and intraoperative periprosthetic fractures.
The paradigm of revision THA has shifted significantly. The historically discouraging long-term results of cemented revisions, combined with the excellent survivorship of cementless implants, have led the vast majority of arthroplasty surgeons to abandon cement in the revision setting. Today, bone deficiency is managed biologically and mechanically with bone grafting and highly porous-coated cementless implants, rather than bulk filling with polymethylmethacrylate (PMMA).
Clinical Pearl: The potential for osteointegration in areas of severe bone deficiency is limited, particularly when structural allografts are interposed between host bone and the implant's porous surface. To achieve durable biologic fixation, contemporary revision stems must utilize extensive porous coatings or fluted tapered designs that bypass proximal defects and achieve diaphyseal scratch fit.
INDICATIONS AND CONTRAINDICATIONS
Diagnostic Evaluation of the Painful THA
The primary indication for revision THA is disabling pain. However, before considering surgical intervention, the surgeon must systematically rule out extrinsic sources of hip and thigh pain. Differential diagnoses include lumbar radiculopathy, spinal stenosis, metastatic or primary osseous tumors, vascular claudication, stress fractures, and complex regional pain syndrome.
Once the pain is localized to the arthroplasty, the surgeon must determine if the functional limitation warrants a major reconstructive operation. In elderly, low-demand patients with multiple comorbidities, conservative management—including activity modification, weight loss, assistive devices, and targeted analgesia—may be more appropriate. In severely debilitated patients where reconstruction is technically unfeasible, a modified Girdlestone resection arthroplasty remains a viable salvage option.
Establishing the Mechanism of Failure
Revisions are broadly indicated for:
1. Painful aseptic loosening of one or both components.
2. Progressive particle-induced osteolysis and bone loss.
3. Implant fracture or mechanical failure (e.g., dissociation of modular components).
4. Recurrent or irreducible instability/dislocation.
5. Periprosthetic joint infection (PJI) managed via one- or two-stage exchange.
6. Periprosthetic fractures.

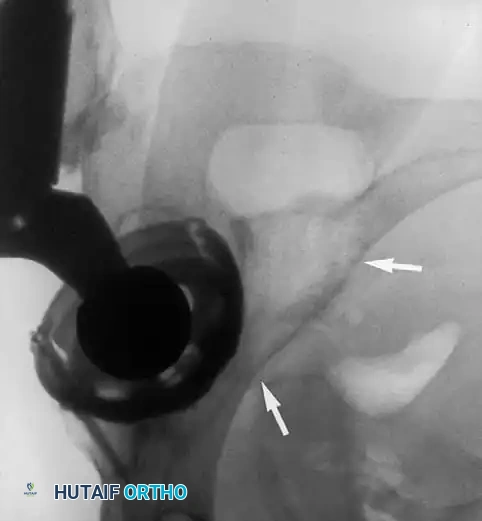
Aseptic vs. Septic Loosening: Differentiating mechanical loosening from PJI is the most critical step in preoperative planning. Septic loosening must be suspected in the presence of rapid endosteal scalloping, periosteal reactions, or early failure (<2 years post-op). Initial screening requires serum Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP).
Surgical Warning: Routine aspiration of all painful hips prior to revision is no longer recommended due to unacceptable false-positive rates (up to 13%). Aspiration should be performed selectively based on clinical suspicion, abnormal serology, or radiographic evidence of rapid osteolysis.
Clinical Presentation of Loosening:
* Start-up Pain: Pain that occurs with the first few steps and improves with ambulation is the hallmark of mechanical loosening.
* Acetabular Loosening: Typically presents as deep groin pain.
* Femoral Loosening: Often radiates to the anterior thigh or distal knee.
Revision is rarely indicated for painless functional deficits, such as isolated loss of motion or painless limb-length discrepancy. Operating on the contralateral hip to correct a discrepancy is ill-advised unless that hip is independently symptomatic.
PREOPERATIVE PLANNING AND TEMPLATING
Planning a complex revision THA requires exhaustive preparation. Intraoperative surprises are common, and the surgeon must formulate multiple contingency plans.
Radiographic Evaluation
High-quality, orthogonal radiographs of the pelvis and the entire femur are mandatory. Poor-quality imaging obscures the distinction between thinned cortical bone, osteolysis, and cement mantles.
* Magnification Markers: Essential for precise digital templating to anticipate the need for extra-small or jumbo components.
* Lateral Femoral Views: Must be assessed to evaluate the anterior bow of the femur. Mismatch between a long, straight revision stem and a bowed femur increases the risk of anterior cortical perforation.
* Advanced Imaging: Computed Tomography (CT) with metal artifact reduction sequences (MARS) is invaluable for assessing acetabular column integrity and pelvic discontinuity.

Equipment and Inventory
Revision THA demands a specialized armamentarium. The surgeon must identify the existing prosthesis to ensure the availability of proprietary extraction tools. If a well-fixed component is to be retained, compatible modular heads and liners must be sourced.
Essential Revision Equipment:
* Fluoroscopic image intensifier (C-arm) and radiolucent table.
* Universal and proprietary stem extraction devices.
* Motorized cement removal tools and flexible intramedullary reamers.
* Flexible, thin osteotomes (e.g., Explant system) for cementless cup removal.
* High-speed metal-cutting burrs (for stripped screws or trunnion failure).
* Pelvic reconstruction plates, multi-hole jumbo cups, and trabecular metal augments.
* Structural and particulate allograft bone.
* Intraoperative cell salvage systems.
SURGICAL APPROACHES
The choice of surgical approach depends on the components requiring revision, the location of bone defects, and the need for extensile exposure. While previous incisions should be utilized when possible to prevent skin necrosis, the deep fascial approach can be tailored.
Posterolateral Approach
The posterolateral approach is the workhorse for most uncomplicated revisions. It provides excellent visualization of the posterior column and the femoral shaft. However, it carries a higher inherent risk of postoperative dislocation compared to anterior-based approaches. If a fixed-head femoral component is retained during an isolated acetabular revision, the femur must be carefully translated anteriorly, often requiring extensive capsular and gluteus maximus releases.
Direct Lateral and Anterolateral Approaches
These approaches are excellent for isolated acetabular revisions, offering a lower dislocation rate. However, they provide limited access to the posterior column and make extensile femoral exposure challenging. Extending the dissection proximally places the superior gluteal nerve at significant risk.
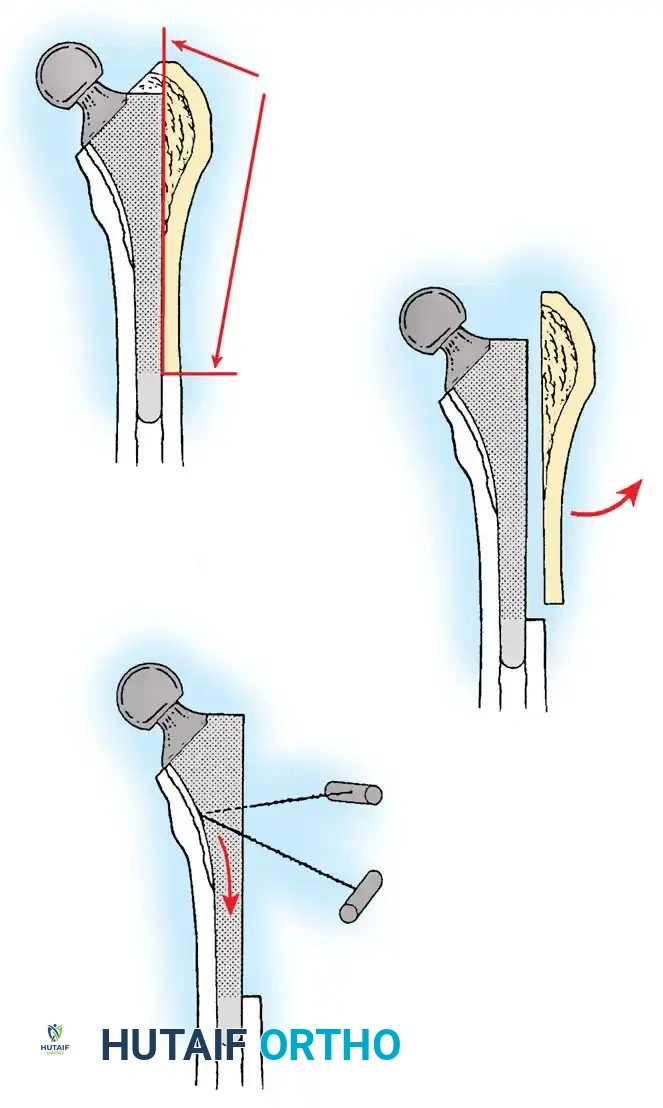
The Extended Trochanteric Osteotomy (ETO)
For complex femoral revisions, particularly those involving well-fixed cementless stems, varus remodeling, or extensive distal cement mantles, the Extended Trochanteric Osteotomy (ETO) is the gold standard.
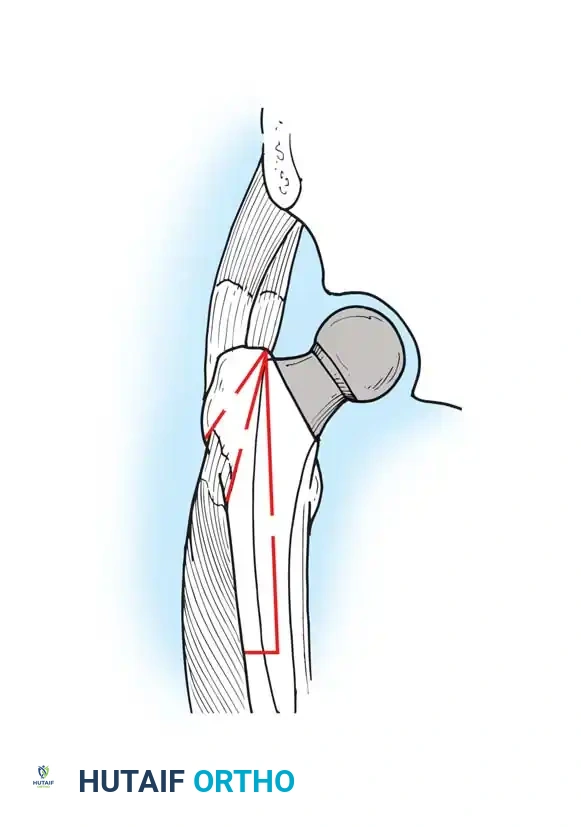
Biomechanics of the ETO:
Unlike a standard trochanteric osteotomy, the ETO preserves the insertion of the gluteus medius and minimus proximally, and the origin of the vastus lateralis distally. This maintains a continuous myofascial sleeve, providing dynamic stability to the osteotomy fragment and dramatically improving union rates (typically >95%).
ETO Technique:
1. Measure the required length of the osteotomy preoperatively (usually 12-15 cm, ensuring it bypasses the well-fixed portion of the stem).
2. Elevate the vastus lateralis anteriorly to expose the lateral femur.
3. Use an oscillating saw or high-speed burr to make the posterior and anterior longitudinal cuts.
4. Complete the distal transverse cut, ensuring rounded corners to prevent stress risers.
5. Lever the fragment open anteriorly, hinging on the intact anterior periosteum and vastus lateralis.
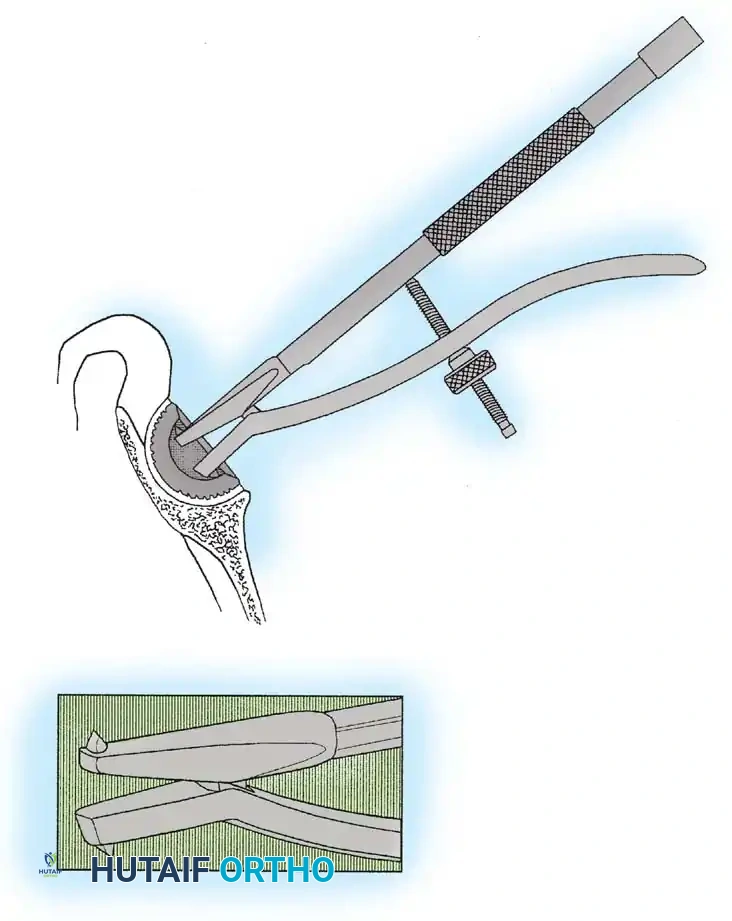
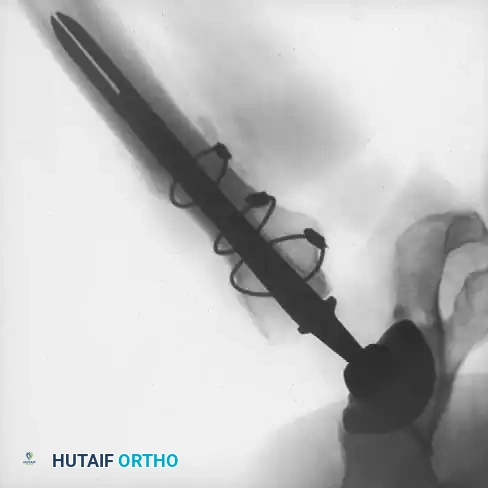
COMPONENT EXTRACTION TECHNIQUES
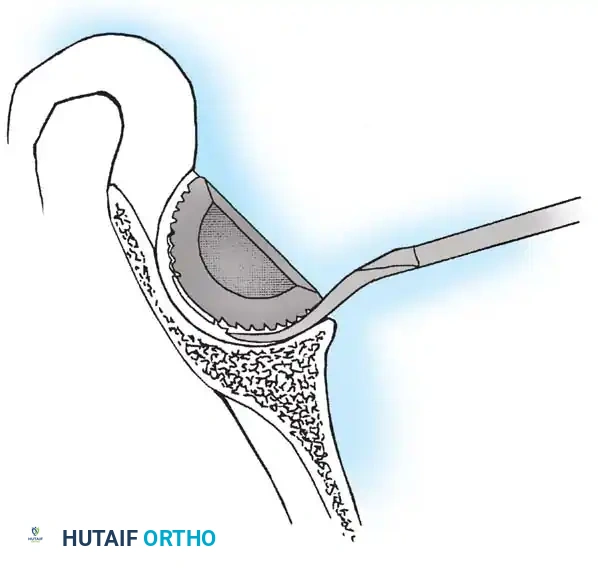
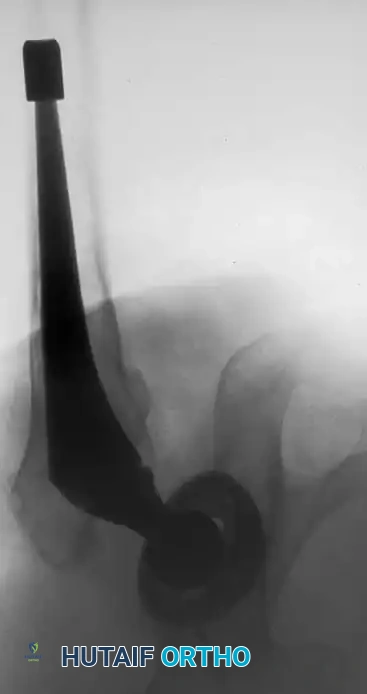
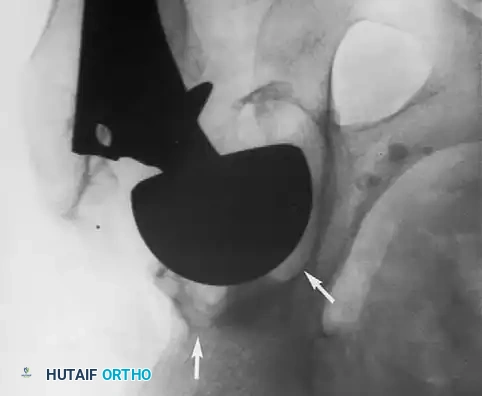
Acetabular Extraction
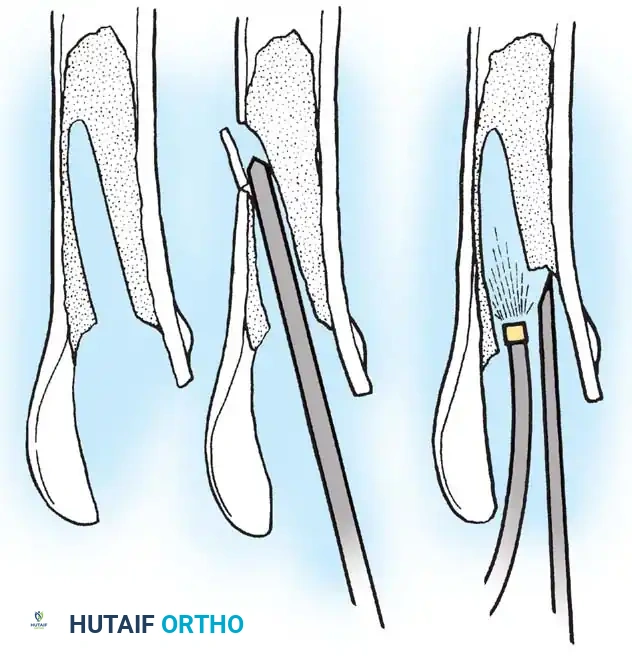
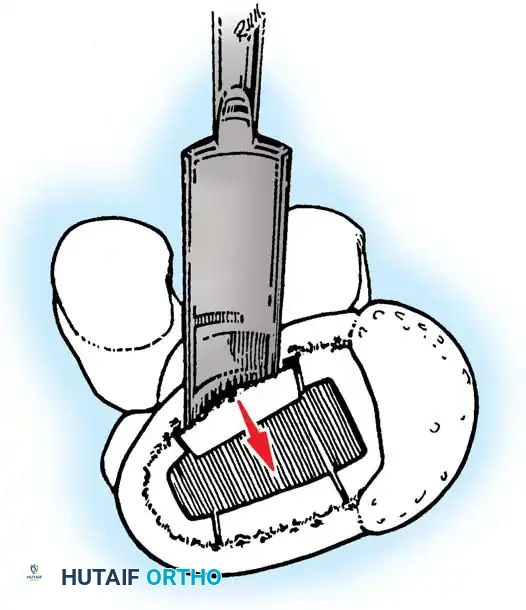
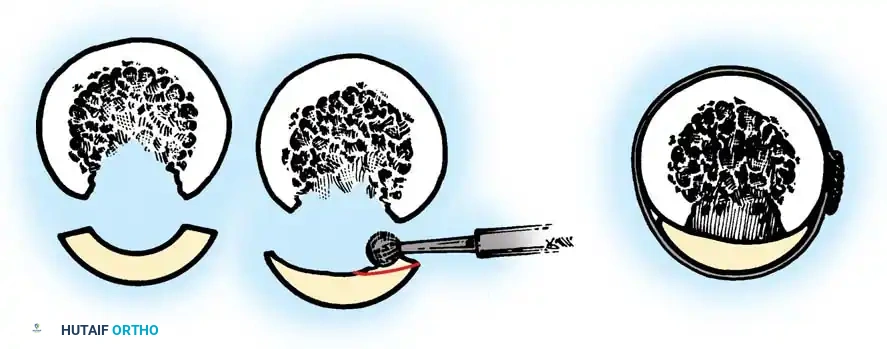
Removal of a well-fixed cementless acetabular component can result in catastrophic bone loss if not performed meticulously. The use of curved, flexible osteotomes (e.g., the Explant system) allows the surgeon to cut the bone-implant interface precisely along the hemisphere of the cup, preserving the critical subchondral bone of the acetabular dome and columns.

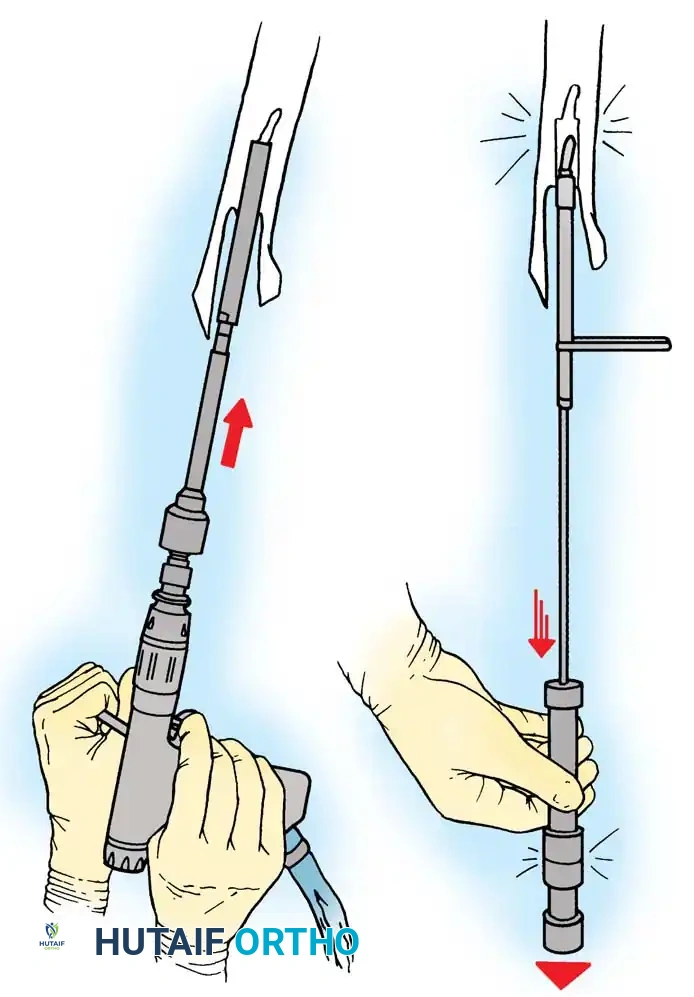
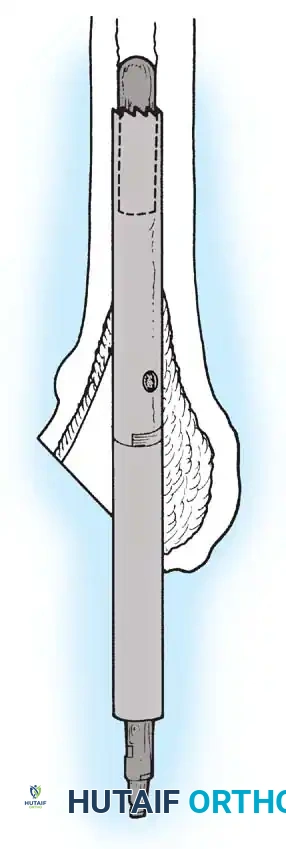
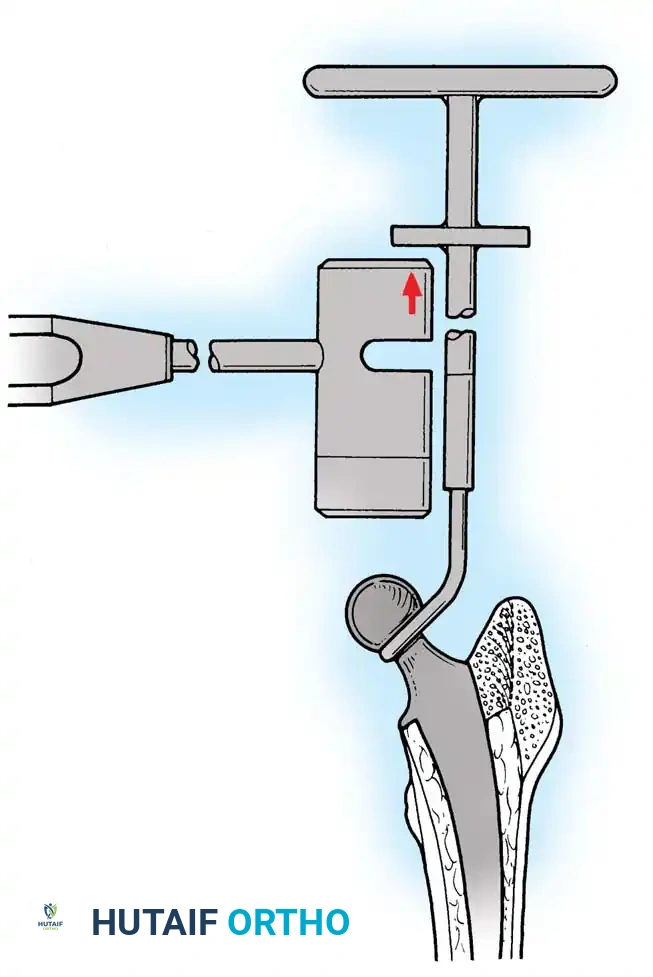
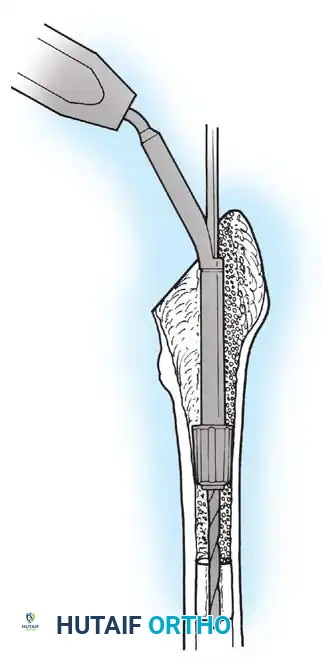
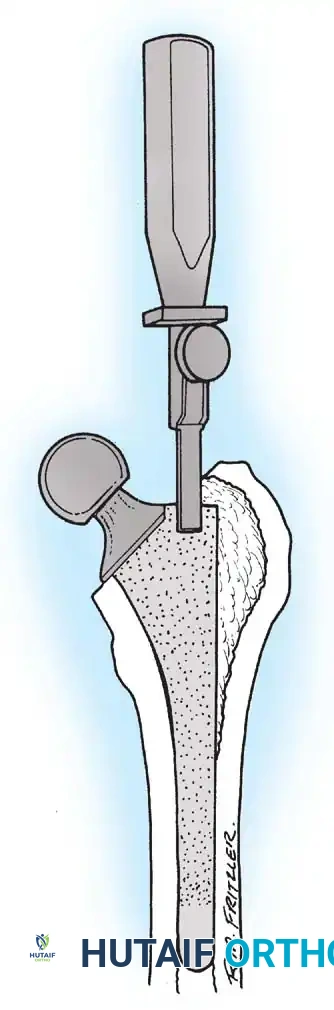
Femoral Extraction
Extracting a femoral stem requires patience and the right instrumentation.
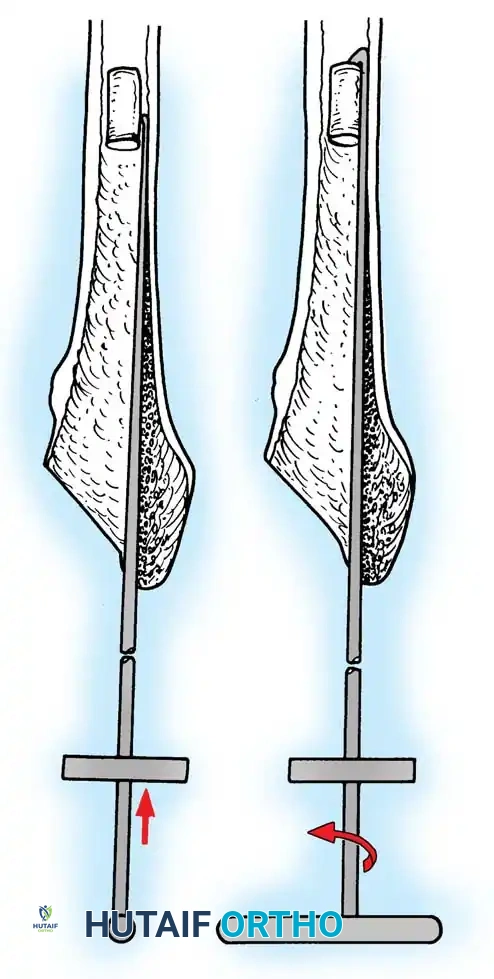
* Cemented Stems: Often easily extracted if loose. The challenge lies in removing the distal PMMA plug. This requires sequential drilling, specialized retrograde hooks, or ultrasonic cement removal tools.
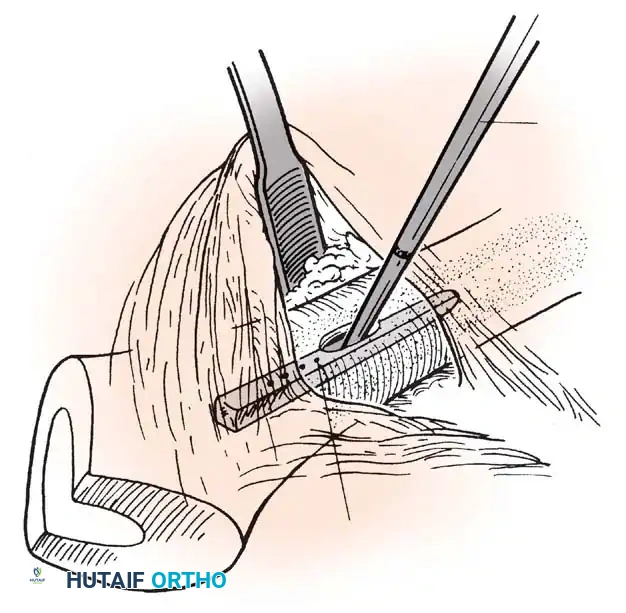
* Cementless Stems: Well-fixed porous-coated stems require disruption of the osteointegrated interface. Flexible osteotomes and high-speed pencil burrs are used to clear the proximal shoulder. If the stem cannot be extracted with a universal slap-hammer, an ETO must be performed to prevent iatrogenic proximal femur fracture.
RECONSTRUCTION AND REIMPLANTATION
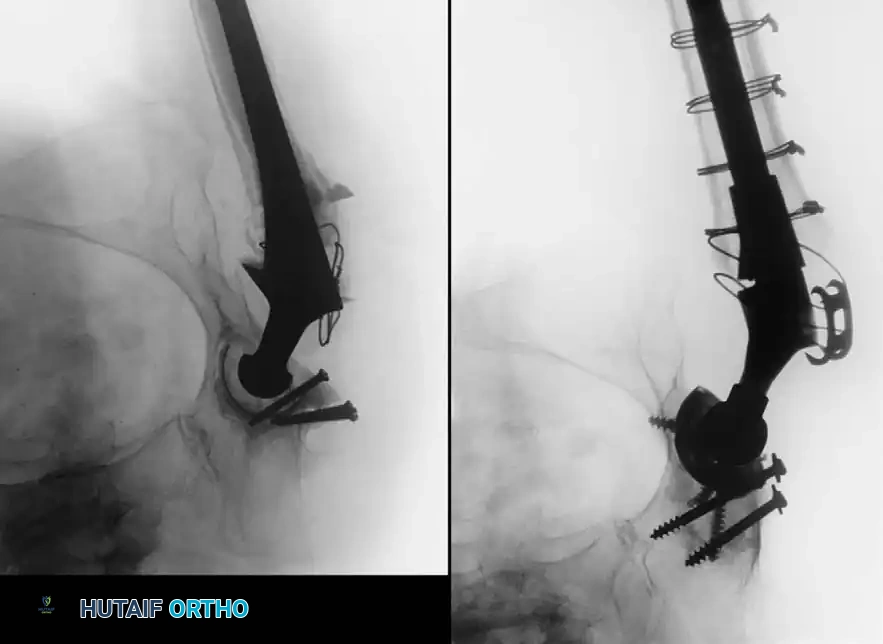
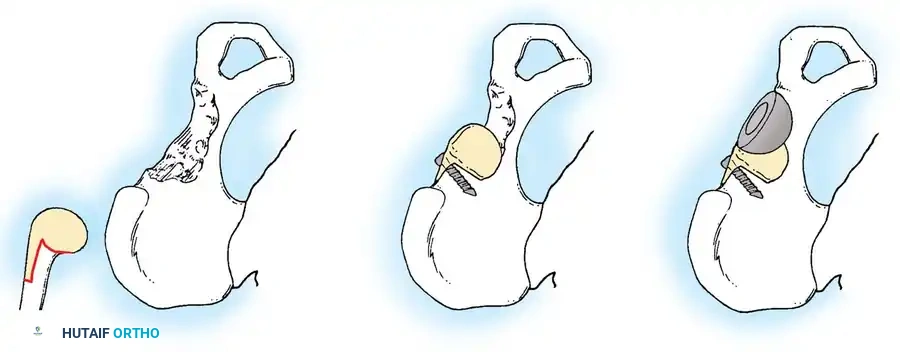
Acetabular Reconstruction
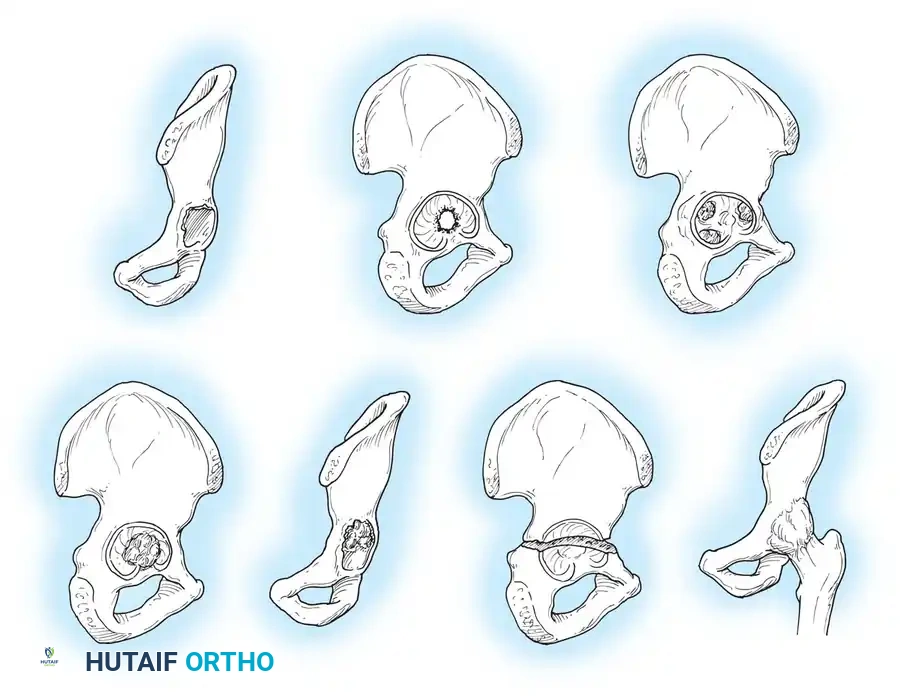
The goal of acetabular revision is to restore the anatomic center of rotation, achieve rigid initial fixation, and provide a biologic environment for long-term stability. Defects are classified using the Paprosky system.
- Type I & II Defects (Cavitary): Managed with hemispherical, highly porous-coated "jumbo" cups (typically >62 mm) and particulate cancellous autograft/allograft. Multiple screws are utilized in the safe zone (posterosuperior quadrant) to achieve rigid primary fixation.
- Type III Defects (Segmental/Severe): Require advanced techniques. Trabecular metal augments are used to fill superior segmental defects and support the cup. In cases of pelvic discontinuity, a cup-cage construct or custom triflange acetabular component may be necessary.
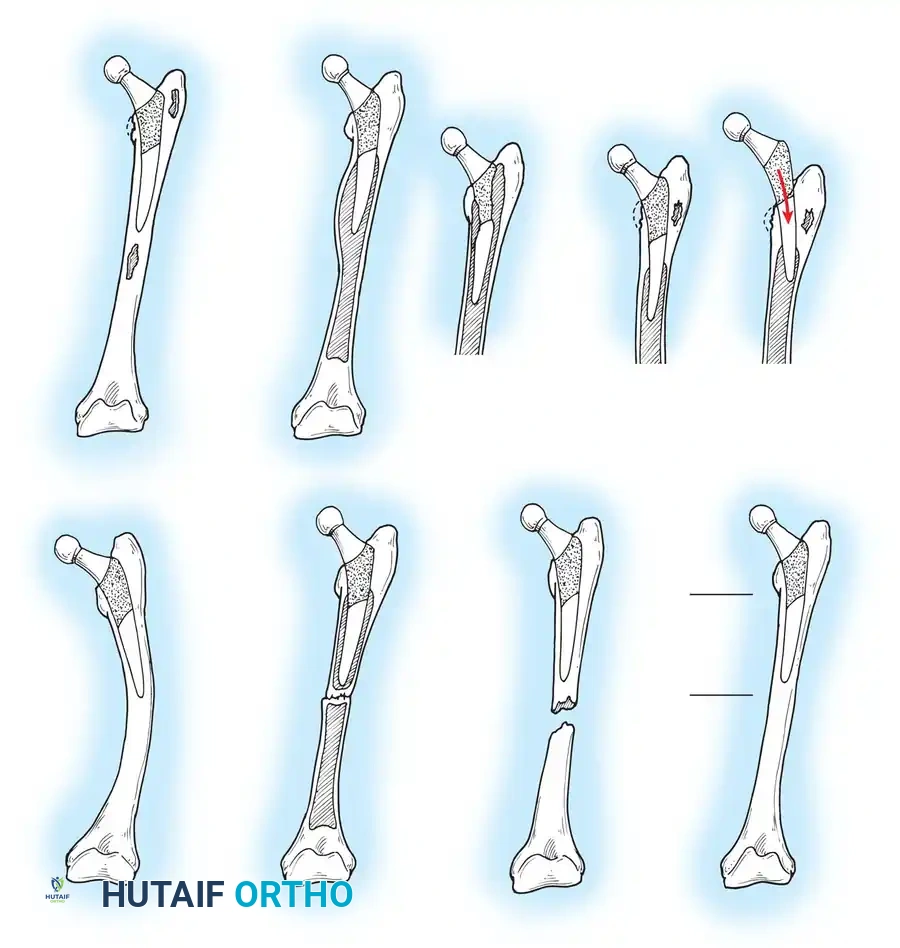
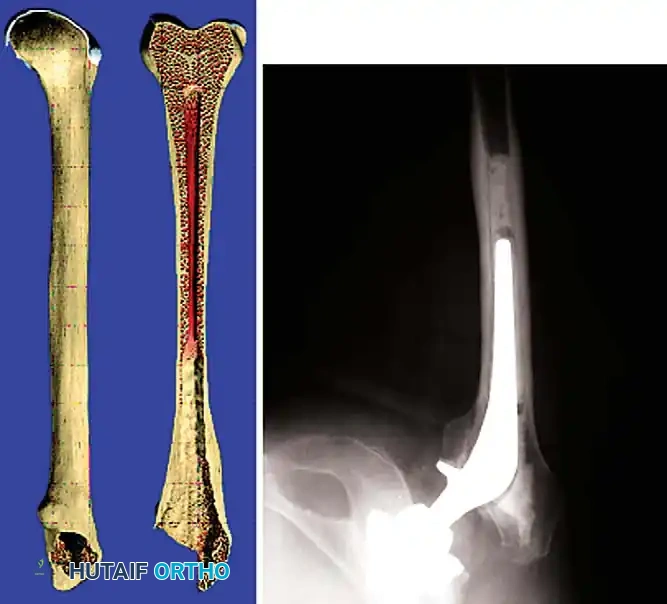
Femoral Reconstruction
Femoral bone loss dictates stem selection. The fundamental biomechanical principle of femoral revision is to achieve rigid fixation in healthy, diaphyseal bone, bypassing the proximal deficiency by a minimum of two cortical diameters (typically 4-6 cm).
Implant Options:
1. Fully Porous-Coated Cylindrical Stems: Excellent long-term survivorship in Type I and II femoral defects. They rely on extensive diaphyseal scratch fit.
2. Modular Fluted Tapered Stems: The modern workhorse for severe (Type III and IV) defects. The flutes provide rotational stability, while the 2-to-3 degree taper achieves axial stability via three-point fixation in the diaphysis. Modularity allows independent adjustment of version, offset, and leg length after the distal stem is rigidly seated.

Pitfall: When seating a diaphyseal-engaging stem, prophylactic cerclage cabling of the distal femur is highly recommended to prevent catastrophic intraoperative splitting of the diaphysis during final impaction.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative regimen must be tailored to the complexity of the reconstruction, the quality of bone stock, and the stability of the implants.
- Weight-Bearing: If rigid diaphyseal fixation and a stable acetabular construct are achieved, patients may be allowed touch-down or partial weight-bearing (20 lbs) for the first 6 weeks. If an ETO was performed, active abduction is restricted until radiographic union is evident (typically 6-8 weeks).
- Thromboembolism Prophylaxis: Due to the extended operative time and altered hemodynamics, aggressive DVT prophylaxis (e.g., LMWH, direct oral anticoagulants, or aspirin based on risk stratification) is mandatory for 28-35 days postoperatively.
- Dislocation Precautions: Patients are maintained on strict posterior (or anterior) hip precautions. In cases of severe abductor deficiency or high risk of instability, a constrained liner or dual-mobility articulation may be utilized intraoperatively, and a postoperative abduction brace may be prescribed.

CONCLUSION
Revision total hip arthroplasty is a demanding procedure that requires a comprehensive understanding of hip biomechanics, implant design, and advanced surgical exposures. Success hinges on meticulous preoperative templating, the ability to safely extract failed components without compromising residual bone stock, and the application of evidence-based reconstructive techniques to achieve durable, long-term biologic fixation. Through careful patient selection and precise execution, surgeons can reliably restore function and alleviate pain in this challenging patient population.
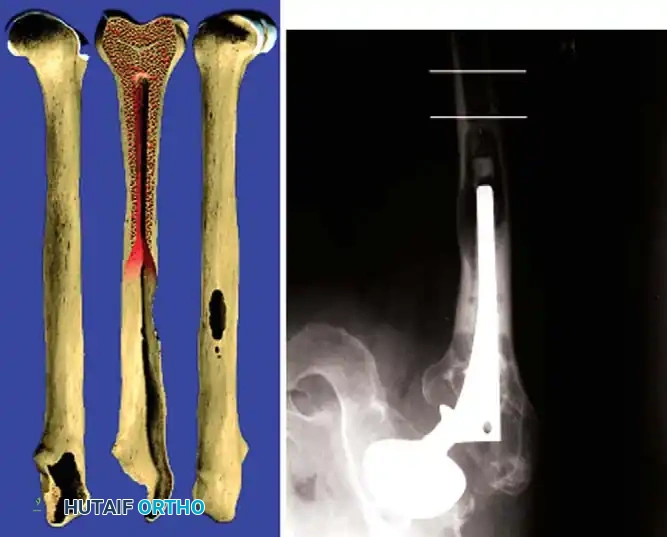
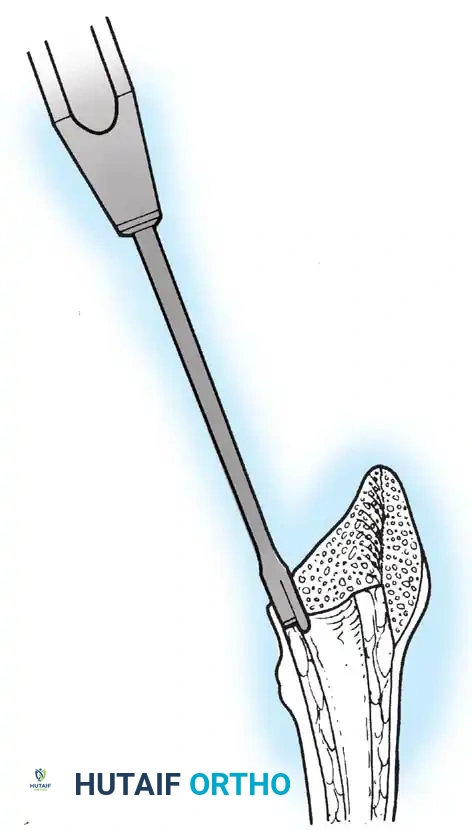
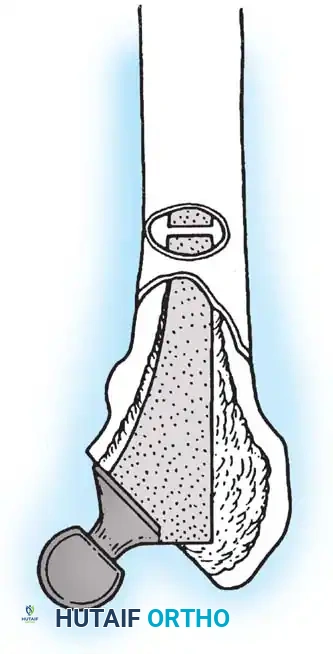
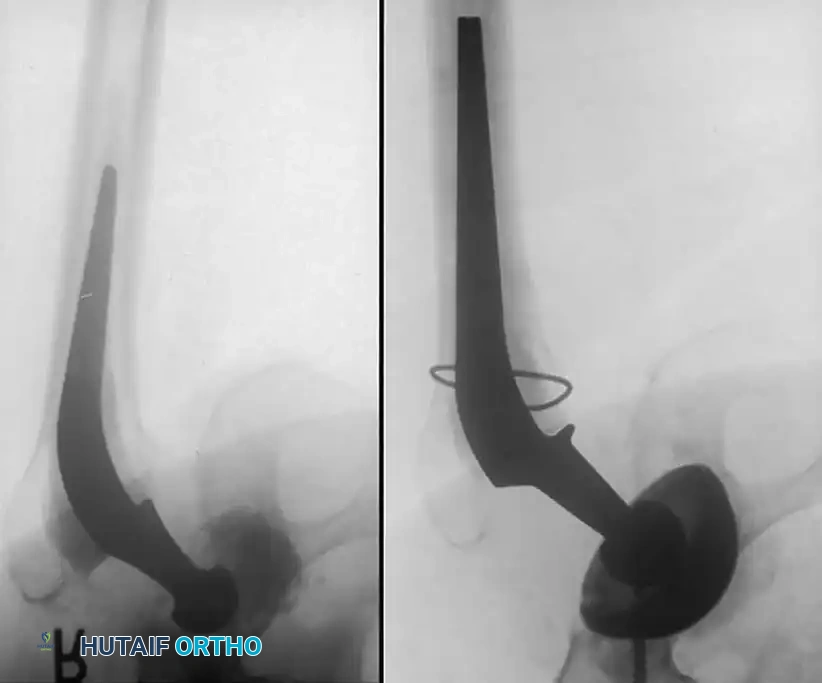
Associated Surgical & Radiographic Imaging


















📚 Medical References
- revision hip arthroplasty, Clin Orthop Relat Res 429:201, 2004.
- Oh I, Sander TW, Treharne RW: Total hip acetabular cup fl ange design and its effect on cement fi xation, Clin Orthop Relat Res 195:304, 1985.
- Otani T, Whiteside LA, White SE: The effect of axial and torsional loading on strain distribution in the proximal femur as related to cementless total hip arthroplasty, Clin Orthop Relat Res 292:376, 1993.
- Parvizi J, Sharkey PF, Hozack WJ, et al: Prospective matchedpair analysis of hydroxyapatite-coated and uncoated femoral stems in total hip arthroplasty: a concise follow-up of a previous report, J Bone Joint Surg 86A:783, 2004.
- Phillips TW: The Bateman bipolar femoral head replacement: a fl uoroscopic study of movement over a four-year period, J Bone Joint Surg 69B:761, 1987.
- Prudhommeaux F, Hamadouche M, Nevelos J, et al: Wear of alumina-on-alumina total hip arthroplasties at a mean 11-year followup, Clin Orthop Relat Res 379:113, 2000.
- Rieker CB, Schon R, Kottig P: Development and validation of a second-generation metal-on-metal bearing: laboratory studies and analysis of retrievals, J Arthroplasty 19:5, 2004.
- Ries MD, Harbaugh MS, Shea J, et al: Effect of cementless acetabular cup geometry on strain distribution and press-fi t stability, J Arthroplasty 12:207, 1997.
- Ritter MA, Keating EM, Faris PM, et al: Metal-backed acetabular cups in total hip arthroplasty, J Bone Joint Surg 72A:672, 1990.
- Ritter MA, Vaughn BK, Frederick LD: Single-stage, bilateral, cementless total hip arthroplasty, J Arthroplasty 10:151, 1995.
- Rockborn P, Olsson SS: Loosening and bone resorption in Exeter hip arthroplasties, J Bone Joint Surg 75:865, 1993.
- Rose RM, Goldfarb EV, Ellis E, et al: Radiation sterilization and the wear rate of polyethylene, J Orthop Res 2:393, 1984.
- Rose RM, Nusbaum HJ, Schneider H, et al: On the true wear rate of ultra high-molecular-weight polyethylene in the total hip prosthesis, J Bone Joint Surg 62A:537, 1980.
- Rydell NW: Forces acting on the femoral head prosthesis: a study on strain gauge supplied prostheses in living persons, Acta Orthop Scand 37(suppl 88):1, 1966.
- Saito M, Saito S, Ohzono K, et al: Effi cacy of alumina ceramic heads for cemented total hip arthroplasty, Clin Orthop Relat Res 283:171, 1992.
- Salvati EA, Betts F, Doty SB: Particulate metallic debris in cemented total hip arthroplasty, Clin Orthop Relat Res 293:160, 1993.
- Schmalzried TP, Jasty M, Harris WH: Periprosthetic bone loss in total hip arthroplasty: polyethylene wear debris and the concept of the effective joint space, J Bone Joint Surg 74A:849, 1992.
- Schmalzried TP, Kwong LM, Jasty M, et al: The mechanism of loosening of cemented acetabular components in total hip arthroplasty: analysis of specimens retrieved at autopsy, Clin Orthop Relat Res 274:60, 1992.
- Schmidt M, Weber H, Schon R: Cobalt chromium molybdenum metal combination for modular hip prostheses, Clin Orthop Relat Res 329:S35, 1996.
- Schuller HM, Marti RU: Ten-year socket wear in 66 hip arthroplasties: ceramic versus metal heads, Acta Orthop Scand 61:240, 1990.
- Semlitsch M, Lehmann M, Weber H, et al: New prospects for a prolonged functional life span of artifi cial hip joints by using the material combination polyethylene/aluminum oxide ceramic/metal, J Biomed Mater Res 11:537, 1977.
- Sioen W, Simon JP, Labey L, et al: Posterior transosseous capsulotendinous repair in total hip arthroplasty: a cadaver study, J Bone Joint Surg 84A:1793, 2002.
- Steinberg B, Harris WH: The “offset” problem in total hip arthroplasty, Contemp Orthop 24:556, 1992.
- Stiehl JB, MacMillan E, Skrade DA: Mechanical stability of porous-coated acetabular components in total hip arthroplasty, J Arthroplasty 6:295, 1991.
- Su EP, Pellicci PM: The role of constrained liners in total hip arthroplasty, Clin Orthop Relat Res 420:122, 2004.
- Sugano N, Nishii T, Nakata K, et al: Polyethylene sockets and alumina ceramic heads in cemented total hip arthroplasty, J Bone Joint Surg 77B:548, 1995.
- Swanson TV: The tapered press fi t total hip arthroplasty: a European alternative, J Arthroplasty 20:63, 2005.
- Sylvain GM, Kassab S, Coutts R, et al: Early failure of a roughened surface, precoated femoral component in total hip arthroplasty, J Arthroplasty 16:142:2001.
- Tooke SM, Amstutz HC, Delaunay C: Hemiresurfacing for femoral head
