Extremity Replantation: Principles, Surgical Techniques, and Functional Outcomes

Key Takeaway
Extremity replantation requires meticulous microvascular expertise and precise patient selection. This guide details the critical steps of replantation, from initial ischemia management and bone shortening to complex neurovascular anastomoses. By adhering to strict biomechanical principles and evidence-based postoperative protocols, orthopedic surgeons can maximize both limb survival and functional recovery, ensuring outcomes that surpass those of amputation and prosthetic fitting.
Introduction and Historical Context
The advent of extremity replantation represents one of the most profound advancements in modern orthopedic and reconstructive surgery. In 1962, Malt and McKhann in Boston successfully reattached a completely amputated human limb for the first time, forever altering the landscape of trauma surgery. This monumental achievement was built upon the excellent experimental and clinical foundations laid by Buncke and Schulz, alongside the persistent clinical innovations of Kleinert et al., who demonstrated that amputated digits could be replanted with reliable success.
Subsequent landmark reports by Komatsu and Tamai in Japan, and by Ch’en et al. at the Sixth People’s Hospital in Shanghai, provided the earliest accounts of completely amputated digits replanted via direct anastomoses of digital vessels. Since these pioneering efforts, digits, hands, feet, and major limbs have been successfully replanted globally. American centers led by Buncke and Schulz (California), Kleinert et al. (Kentucky), and Urbaniak (North Carolina) established the institutional blueprints for replantation centers across the United States. Equally significant were the international contributions from O’Brien (Australia), Ch’en (Shanghai), Biemer (Germany), Meyer (Switzerland), and Millesi (Austria).
Epidemiology and Mechanisms of Injury
Atroshi and Rosberg’s extensive review of international epidemiologic data reveals that 85% to 95% of replantations occur in young men, with a mean age of 25 to 30 years. Pediatric cases account for 3% to 10% of patients in series that include children.
The mechanism of injury is a critical determinant of both survival and functional outcome. The primary mechanisms reported in major replantation series include:
* Guillotine (Sharp) Amputations (14% to 53%): Yield the highest survival rates due to localized tissue damage and clean vascular transections.
* Crush Injuries (11% to 62%): Present significant challenges due to broad zones of injury, requiring extensive debridement and often necessitating vein grafts.
* Avulsion Injuries (16% to 29%): Carry the poorest prognosis. The intimal damage stretches far beyond the visible level of amputation, leading to a high risk of postoperative thrombosis.
The Replantation Team and Institutional Requirements
Replantation of amputated upper extremity parts demands a highly specialized infrastructure. Procedures must be performed by surgeons fellowship-trained in hand and upper extremity surgery. Furthermore, digital replantation requires absolute proficiency in operating microscope utilization, with surgeons demonstrating a predictable microvascular patency rate of 90% or better.
Clinical Pearl: While a single surgeon with highly motivated assistants can perform a replantation, it is vastly superior to utilize rotating teams of surgeons. This mitigates fatigue during procedures that can exceed 12 hours. During the microvascular phases, at least one scrubbed surgeon must be an expert in microneural and microvascular repair.
Institutions must provide 24-hour availability of the replantation team, dedicated surgical suites, specialized micro-instruments, and an intensive care unit staffed by nursing and anesthesia personnel trained in the hemodynamic management of prolonged microvascular cases.
General Considerations and Patient Selection
The fundamental prerequisite for replantation is that the anticipated functional outcome must surpass that of a well-fitted prosthesis or a revised amputation stump. The surgeon must carefully weigh the potential for useful motion and sensibility against the surgical risk, prolonged rehabilitation, and economic burden.
Key factors evaluated prior to replantation include:
* Age of the patient: Children have superior nerve regeneration and neuroplasticity.
* Severity and mechanism of injury: Avulsion vs. sharp cut.
* Level of amputation: Proximal vs. distal.
* Warm and cold ischemia times: Muscle tissue undergoes irreversible necrosis after 6 hours of warm ischemia, whereas digits (lacking muscle belly) can tolerate up to 12 hours of warm ischemia and 24 hours of cold ischemia.
* Multiple or bilateral amputations: Strong indications for replantation.
* Patient’s general condition: Life over limb; concomitant life-threatening injuries preclude prolonged replantation surgery.

Age-Specific Indications
There are no absolute upper or lower age limits for replantation. Replantations have been successful in infants just a few weeks old and in adults over 70 years of age.
Pediatric Considerations: The young patient poses unique technical challenges due to vessel sizes often measuring only 0.5 mm. Placing micro-clamps on the distal segment can be exceedingly difficult. Venous outflow may require a volar venous anastomosis or controlled bleeding (often facilitated by medicinal leeches). Despite these challenges, pediatric replantations yield exceptional results. In a long-term follow-up of 26 children (44 digits), 96% achieved excellent results, with a mean total active motion (TAM) of 151 degrees and 88% regaining normal 2-point discrimination. Subsequent bone growth averaged 93% of normal, provided the physis was not directly injured.
Geriatric Considerations: The upper age limit is dictated by physiologic age rather than chronological age. Poor nerve regeneration and joint stiffness limit functional outcomes in the elderly. However, replantation above the elbow may be indicated to preserve joint length in anticipation of a subsequent below-elbow amputation, thereby allowing for a more functional prosthetic fitting.
Thumb and Multiple Digit Replantation
The thumb contributes to approximately 40% to 50% of hand function. Therefore, amputated thumbs should be replanted whenever technically feasible, even in cases of severe injury. Arakaki and Tsai reported a 71% overall survival rate for thumb replantations. Survival correlated heavily with the injury mechanism: 88% for minimally damaged amputations, 58% for avulsions, and 12% for severe crush/avulsion injuries.

Step-by-Step Surgical Technique
The sequence of replantation generally follows a standardized progression: Bone fixation, Extensor tendon repair, Arterial anastomosis, Nerve repair, Flexor tendon repair, Venous anastomosis, and Skin closure.
1. Preparation and Debridement
Meticulous debridement under tourniquet control is the most critical initial step. All devitalized tissue, including bone, muscle, and skin, must be excised. The neurovascular bundles are identified and tagged under loupe magnification.
2. Bone Preparation and Shortening
Bone shortening is mandatory. Attempting to maintain original bone length will result in excessive tension on the microvascular anastomoses and nerve repairs, leading to inevitable failure.
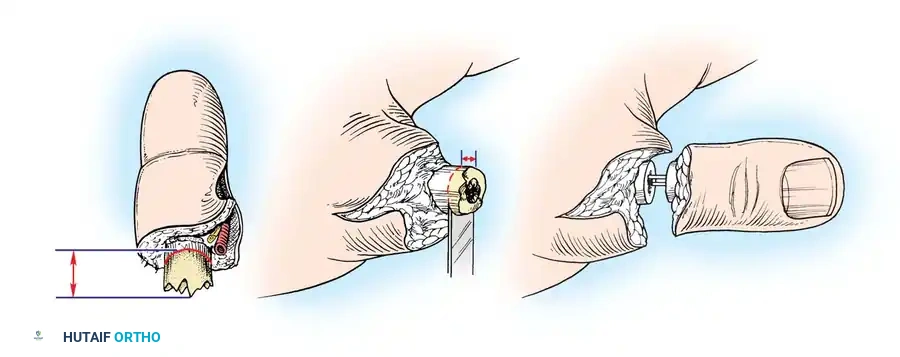
Surgical Warning: Inadequate bone shortening is a primary cause of vascular thrombosis. Shorten the bone until healthy, uninjured intima can be coapted without tension.
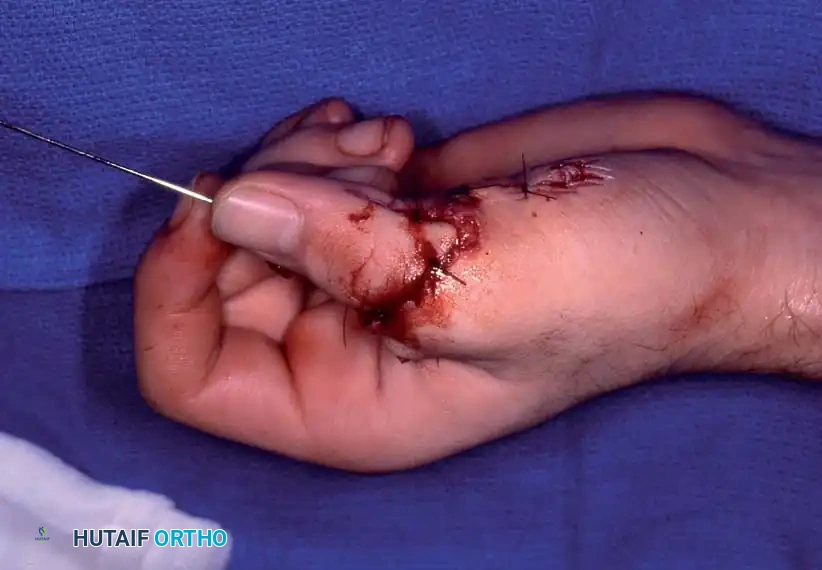
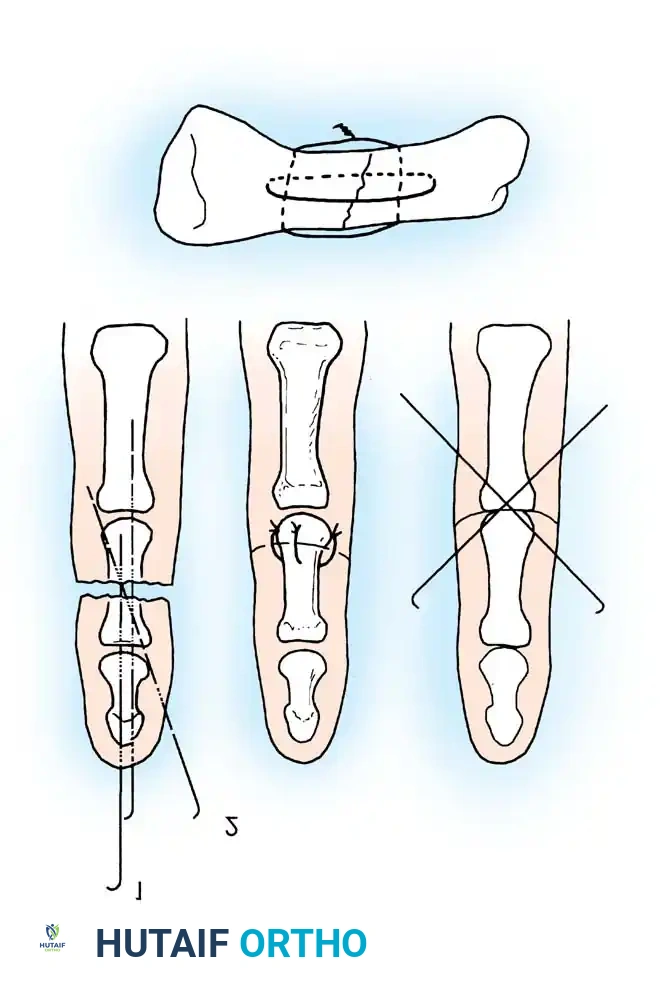
3. Osteosynthesis
Rigid or semi-rigid fixation is required to allow early mobilization. Techniques include longitudinal K-wires, crossed K-wires, intraosseous wiring (often combined with a K-wire for rotational stability), or mini-plates. Intraosseous wiring provides excellent biomechanical stability while maintaining a low profile.

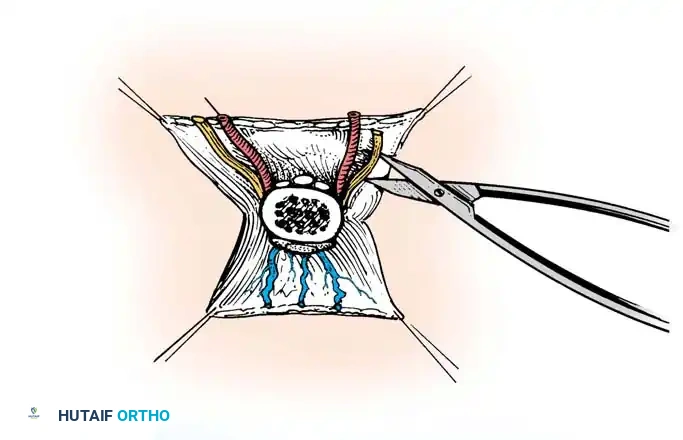
4. Microvascular Anastomosis
The operating microscope is brought into the field. Arteries are repaired first to minimize ischemia time, though some surgeons prefer repairing veins first to reduce blood loss. The intima must be inspected under high magnification; any "ribbon sign" or intimal separation dictates further resection and the use of an interpositional vein graft.
5. Nerve Repair
Primary epineurial or group fascicular repair is performed. If a tension-free repair is impossible, nerve grafts (e.g., medial antebrachial cutaneous nerve or sural nerve) are utilized.
Clinical Pearl: With perfect coaptation of the nerve graft to the stump ends, many additional sutures may not be required. If the grafts are not perfectly coapted, rotate them around the first suture and add as few additional sutures as necessary to minimize foreign body reaction and scarring.
6. Soft Tissue and Skin Closure
Skin must be closed loosely. The graft or repaired vessels must not be displaced by shearing forces during wound closure.
Surgical Warning: If closure is tight in the distal forearm, Millesi recommends making an ulnar midlateral incision to relax the suture line over the graft site, followed by skin grafting the midlateral defect.
Avoid the use of suction drainage, which can induce vasospasm or disrupt anastomoses. Accomplish drainage using passive Silastic drains.

Postoperative Protocol
The extremity must be immobilized in a well-padded plaster splint in the exact position that was maintained throughout the microvascular procedure. Elevation is critical to promote venous drainage, but excessive elevation can compromise arterial inflow.

Postoperative monitoring includes clinical observation (color, capillary refill, turgor, temperature) and objective monitoring (surface temperature probes, pulse oximetry, or laser Doppler). Anticoagulation protocols vary by institution but frequently include aspirin, dextran, or heparin, particularly in crush injuries or when vein grafts are utilized.
Survival Rates and Functional Outcomes
Overall survival rates reported by U.S. and international centers range from 50% to 92% for replanted and revascularized parts. Major limb replantations have a survival rate of 40% to 80%.
Level of amputation significantly impacts survival:
* Above-Elbow vs. Below-Elbow: Below-elbow replantations generally fare better. The Beijing Trauma Hospital reported 61% survival for above-elbow and 37% for below-elbow, whereas Ikuta reported 88% and 80%, respectively.
* Wrist Level: Replantations at or just proximal to the wrist show uniformly optimistic survival rates in the 80% to 90% range.
Assessing Functional Success
Success cannot be measured by survival alone; it is dictated by the return of useful function. Graham et al. evaluated 22 patients with successful upper extremity replantations at or proximal to the wrist against 22 matched amputees fitted with prosthetics. In closely matched adult below-elbow injuries, the replantation group had 50% good/excellent outcomes, whereas the prosthetic group had none.
Ch’en et al. developed a comprehensive grading system for evaluating function after extremity replantation, which remains a gold standard for assessing multisystem injuries:
Ch’en Criteria for Evaluation of Function:
* Grade I: Able to resume original work; Range of Motion (ROM) > 60% of normal; complete or nearly complete recovery of sensibility; muscle power grade 4-5.
* Grade II: Able to resume some suitable work; ROM > 40% of normal; nearly complete sensibility; muscle power grade 3-4.
* Grade III: Able to carry out activities of daily living; ROM > 30% of normal; partial recovery of sensibility; muscle power grade 3.
* Grade IV: Almost no usable function of the survived limb.
Using these criteria, Tamai reported 72% excellent and good results, and Ch’en reported 67.7%. Berger et al. found that 78% of patients successfully integrated the replanted part into their usual activities.



Complications and Patient Satisfaction
Despite the rigorous nature of the surgery, most patients are satisfied and state they would undergo replantation again. However, Lukash et al. noted that in single- or double-digit replantations (often from power tool injuries), dissatisfaction can arise due to emotional stress, financial loss, and the need for subsequent tenolyses or capsulotomies. The mean cost per digit replantation was approximately $20,330 in 1996, a figure that has exponentially increased.
Cold Intolerance: This is experienced by almost all replantation patients. Povlsen et al. demonstrated in a 12-year follow-up that cold-induced vasospasm does not physiologically improve over time; rather, patients perceive improvement because they adapt their habits to avoid cold exposure.
Sensory Recovery: While most patients regain protective sensibility, 2-point discrimination (especially in proximal injuries) rarely returns to less than 10 mm. Fine tactile discrimination is seldom fully restored.
Return to Work: The more proximal the injury, the longer the delay in returning to employment. Some return within 3 weeks, while complex proximal injuries may require 1.5 to 2 years of intensive hand therapy.
Conclusion
Extremity replantation is a triumph of modern microsurgery, requiring a synthesis of orthopedic biomechanics and vascular precision. While transmetacarpal and proximal muscle-belly amputations carry a guarded prognosis, adherence to strict surgical principles—adequate bone shortening, tension-free nerve coaptation, meticulous intimal repair, and aggressive postoperative rehabilitation—ensures that the functional capacity of the replanted limb frequently exceeds that of the best available prosthetics.
You Might Also Like