Meniscal Preservation, Repair, and Allograft Transplantation: A Comprehensive Surgical Masterclass
Key Takeaway
The meniscus plays a critical role in knee biomechanics, load transmission, and joint stability. Recognizing the devastating chondral consequences of total meniscectomy, modern orthopedic surgery prioritizes meniscal preservation. This comprehensive guide details the evidence-based indications, biomechanical principles, and step-by-step surgical techniques for meniscal repair and meniscal allograft transplantation (MAT), providing orthopedic surgeons with the essential framework to optimize joint longevity and patient outcomes.
Introduction to Meniscal Preservation
Historically, the meniscus was viewed as a functionless vestige, leading to the widespread practice of total meniscectomy for any meniscal pathology. However, landmark biomechanical and clinical studies over the past several decades have unequivocally established the meniscus as a vital structure for load transmission, shock absorption, joint stability, and articular cartilage nutrition. The seminal observations by Fairbank in 1948 detailed the predictable radiographic degenerative changes following meniscectomy—namely, joint space narrowing, squaring of the femoral condyle, and osteophyte formation.
Today, the orthopedic paradigm has shifted entirely toward meniscal preservation. This masterclass synthesizes the foundational biomechanical literature and details the advanced surgical techniques required for meniscal repair, the management of discoid menisci, and meniscal allograft transplantation (MAT).
Biomechanics and Functional Anatomy
To master meniscal surgery, the orthopedic surgeon must possess a profound understanding of knee biomechanics and meniscal microvasculature.
Load Transmission and Hoop Stresses
The menisci are wedge-shaped, fibrocartilaginous structures that increase the congruency of the tibiofemoral joint. By expanding the contact area, they dramatically reduce contact stresses on the underlying articular cartilage. Axial loads applied to the knee are converted into tensile "hoop stresses" within the circumferentially oriented Type I collagen fibers of the meniscus. A single radial tear that disrupts this peripheral circumferential rim functionally equates to a total meniscectomy, as the meniscus loses its ability to contain hoop stresses and extrudes peripherally.
Secondary Restraint to Translation
As demonstrated by Butler, Noyes, and Grood, the medial meniscus serves as a critical secondary restraint to anterior tibial translation. In the anterior cruciate ligament (ACL)-deficient knee, the posterior horn of the medial meniscus acts as a wedge against the medial femoral condyle. Consequently, medial meniscectomy in an ACL-deficient knee exponentially increases anterior laxity and accelerates chondral degradation.
The Vascular Watershed
Arnoczky and Warren’s classic microangiographic studies defined the vascular supply of the meniscus, originating from the medial and lateral geniculate arteries. The vascularity is divided into three zones:
* Red-Red Zone: The peripheral 10% to 30%, which is fully vascularized and possesses excellent healing potential.
* Red-White Zone: The middle third, representing the watershed area with variable healing capacity.
* White-White Zone: The inner avascular third, which relies entirely on diffusion from synovial fluid for nutrition. Tears in this zone historically required resection, though modern biologic augmentation techniques are expanding the indications for repair.
Clinical Pearl: The lateral meniscus covers approximately 70% of the lateral tibial plateau, whereas the medial meniscus covers only 50% of the medial plateau. Because the lateral compartment is inherently more convex and relies more heavily on the meniscus for congruency, lateral meniscectomy leads to more rapid and severe chondral degradation than medial meniscectomy.
Indications for Meniscal Surgery
Meniscal Repair
- Indications: Acute, longitudinal tears in the red-red or red-white zones; root tears; radial tears that can be anatomically reduced; tears in young, active patients; tears occurring concurrently with ACL reconstruction (which provides a biologically favorable hemarthrosis).
- Contraindications: Degenerative, complex, or macerated tears; tears in the avascular white-white zone without biologic augmentation; uncorrected knee instability (e.g., untreated ACL tear), which leads to a high rate of repair failure.
Meniscal Allograft Transplantation (MAT)
- Indications: Prior total or subtotal meniscectomy; localized pain in the affected compartment; age generally under 50 years; stable knee (or concurrent ligamentous reconstruction); normal mechanical alignment (or concurrent osteotomy).
- Contraindications: Advanced osteoarthritis (Outerbridge Grade III/IV on the opposing articular surface); uncorrected malalignment; uncorrected ligamentous instability; inflammatory arthropathy; obesity (BMI > 30).
Surgical Positioning and Setup
- Anesthesia and Positioning: The patient is placed supine under general or regional anesthesia. A tourniquet is applied to the proximal thigh.
- Leg Holder vs. Post: The operative leg is placed in a standard circumferential leg holder or against a lateral post to allow for valgus/varus stress. The foot of the bed is lowered to allow the knee to flex to 120 degrees.
- Portal Placement: Standard anterolateral (viewing) and anteromedial (working) portals are established adjacent to the patellar tendon. Accessory portals may be required depending on the technique.
Meniscal Repair Techniques
The choice of repair technique depends on the location and morphology of the tear.
1. The Inside-Out Technique
Considered the gold standard for tears of the posterior and middle thirds of the meniscus, this technique allows for precise suture placement and excellent biomechanical strength.
- Approach:
- For medial repairs, a posteromedial incision is made posterior to the medial collateral ligament (MCL). The sartorial fascia is incised, and the interval between the medial head of the gastrocnemius and the posterior capsule is developed. A retractor (e.g., Henning retractor) is placed anterior to the gastrocnemius to protect the saphenous nerve and vessels.
- For lateral repairs, a posterolateral incision is made. The interval between the biceps femoris and the lateral head of the gastrocnemius is developed. The common peroneal nerve must be identified and protected.
- Suture Passing: Zone-specific cannulas are introduced through the anterior portals. Long, flexible needles carrying non-absorbable sutures (e.g., 2-0 braided polyester or ultra-high-molecular-weight polyethylene) are passed across the tear and retrieved in the posterior incision.
- Knot Tying: Sutures are tied directly over the joint capsule while the knee is held in 90 degrees of flexion to ensure appropriate tensioning and avoid capturing the capsule in a non-anatomic position.
Surgical Warning: When performing a lateral inside-out repair, the needles must exit anterior to the biceps femoris tendon to avoid catastrophic injury to the common peroneal nerve.
2. The Outside-In Technique
This technique is highly effective for tears of the anterior horn and middle third of the meniscus.
- Approach: An 18-gauge spinal needle is passed from the outside of the knee, through the capsule, and across the meniscal tear under direct arthroscopic visualization.
- Suture Passing: A monofilament suture (e.g., PDS) is passed through the needle into the joint. A second needle is passed adjacent to the first, and a suture shuttle (e.g., a wire loop) is introduced. The first suture is pulled through the second needle tract, creating a horizontal or vertical mattress stitch.
- Knot Tying: A small stab incision is made between the needle entry points, and the knot is tied subcutaneously over the capsule.
3. The All-Inside Technique
Advancements in implant technology have made all-inside repairs popular for posterior horn tears, avoiding the need for posterior accessory incisions.
- Implant Deployment: Modern devices utilize pre-tied, sliding knots with PEEK or polymer anchors. The device is inserted through the working portal, passed across the tear, and the first anchor is deployed behind the capsule. The needle is withdrawn slightly, repositioned, and the second anchor is deployed to create a mattress construct.
- Tensioning: The pre-tied knot is advanced using a knot pusher, compressing the tear.
- Pitfalls: Care must be taken to use the depth limiter on the insertion device. Plunging too deeply through the posterior capsule can result in popliteal artery or nerve injury.
Biologic Augmentation
To enhance healing, particularly in the red-white or white-white zones, biologic augmentation is highly recommended.
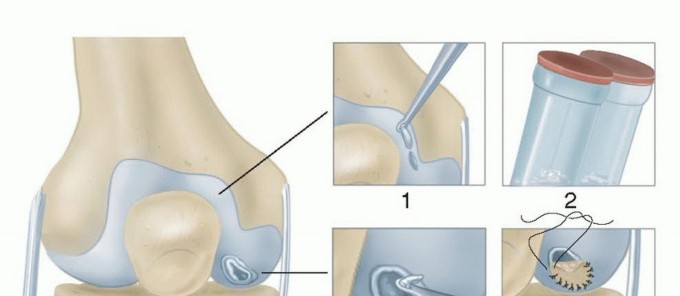
* Fibrin Clot: As described by Arnoczky and Henning, an exogenous fibrin clot can be harvested from the patient's peripheral blood and sutured into the meniscal defect to provide a chemotactic and mitogenic scaffold.
* Marrow Venting: Trephination of the peripheral rim or microfracture of the intercondylar notch releases bone marrow elements (mesenchymal stem cells and growth factors) into the joint, simulating the favorable healing environment of a concurrent ACL reconstruction.
Management of the Discoid Meniscus
A discoid meniscus is a congenital morphological variant, most commonly affecting the lateral meniscus, characterized by a thickened, disc-like shape. It is prone to tearing due to abnormal biomechanics and poor vascularity.
- Wrisberg Ligament Variant: Lacks normal posterior capsular attachments, leading to hypermobility and the classic "snapping knee" syndrome.
- Surgical Technique (Saucerization): The goal is to resect the central portion of the discoid meniscus, leaving a stable, peripheral rim of approximately 6 to 8 mm. This is achieved using arthroscopic punches and shavers.
- Peripheral Repair: If the remaining peripheral rim is unstable (as in the Wrisberg variant), it must be repaired to the capsule using inside-out or all-inside techniques to restore hoop stress containment.
Meniscal Allograft Transplantation (MAT)
When a meniscus is irreparably damaged or previously excised, MAT offers a biologic solution to restore joint mechanics, alleviate pain, and potentially delay the onset of osteoarthritis.
Graft Sizing and Processing
- Sizing: Accurate sizing is paramount. Mismatch leads to altered contact mechanics and graft failure. Sizing is typically performed using plain radiographs (measuring the tibial plateau width and AP dimensions) or MRI.
- Processing: Fresh-frozen (cryopreserved) allografts are the standard of care. They maintain the collagen matrix architecture while minimizing immunogenicity. Viable chondrocytes are not strictly necessary for the biomechanical function of the graft.
Surgical Technique: Bone Plug vs. Bone Bridge
The meniscus must be securely anchored to the tibia to restore hoop stresses. Soft tissue fixation alone is biomechanically inferior and leads to graft extrusion.
- Medial MAT (Bone Plug Technique): The anterior and posterior horns of the medial meniscus are separated by a wide distance. Therefore, the graft is prepared with two separate cylindrical bone plugs attached to the horns. Corresponding tunnels are drilled in the patient's medial tibial plateau. The graft is introduced, the bone plugs are pulled into the tunnels, and fixed with interference screws or tied over a cortical button.
- Lateral MAT (Bone Bridge/Slot Technique): The anterior and posterior horns of the lateral meniscus insert in close proximity. The graft is prepared with a continuous rectangular bone bridge connecting the two horns. A corresponding rectangular slot is created in the patient's lateral tibial plateau. The graft is introduced via a keyhole approach, and the bone bridge is impacted into the slot, providing rigid anatomic fixation.
- Capsular Fixation: Once the bony attachments are secured, the periphery of the allograft is sutured to the host capsule using inside-out or all-inside techniques, placing sutures every 5 mm to ensure a watertight seal.
Surgical Pitfall: Failure to achieve anatomic placement of the meniscal roots will result in a non-functional graft. A graft placed too far peripherally will extrude, while a graft placed too centrally will experience excessive shear forces and tear.
Postoperative Rehabilitation Protocols
Rehabilitation following meniscal repair or MAT requires a delicate balance between protecting the healing tissue and preventing arthrofibrosis.
Phase I: Protection (Weeks 0-6)
- Weight-Bearing: Restricted. Touch-down weight-bearing (TDWB) with crutches is typically enforced to prevent axial loading and shear stresses.
- Range of Motion (ROM): Locked in extension for ambulation. Passive ROM is initiated early but restricted to 0-90 degrees. Flexion past 90 degrees places excessive shear stress on the posterior horn.
- Bracing: A hinged knee brace is worn at all times.
Phase II: Early Strengthening (Weeks 6-12)
- Weight-Bearing: Progressive return to full weight-bearing.
- ROM: Progression to full, unrestricted ROM.
- Exercises: Closed kinetic chain exercises (e.g., mini-squats, leg presses) are initiated. Open kinetic chain hamstring exercises are avoided if a posterior inside-out repair was performed near the hamstring insertions.
Phase III: Return to Play (Months 4-6+)
- Criteria: Full, painless ROM; no effusion; quadriceps and hamstring strength >90% of the contralateral limb.
- Activity: Gradual reintroduction of pivoting, cutting, and sport-specific drills. For MAT patients, return to high-impact sports is generally discouraged to protect the longevity of the allograft, though low-impact activities are fully supported.
Conclusion
The evolution from routine meniscectomy to meticulous meniscal preservation represents one of the most significant advancements in modern orthopedic sports medicine. By understanding the intricate biomechanics of the knee and mastering the technical nuances of inside-out repair, biologic augmentation, and meniscal allograft transplantation, the orthopedic surgeon can effectively restore joint kinematics, alleviate pain, and alter the natural history of the meniscus-deficient knee. Strict adherence to indications, precise surgical execution, and controlled postoperative rehabilitation are the cornerstones of successful outcomes in meniscal surgery.
📚 Medical References
- [meniscal repair
Bassett FH III, Billys JB, Gates HS III: A simple surgical approach to the posteromedial ankle, Am J Sports Med 21:144, 1993.](https://pubmed.ncbi.nlm.nih.gov/?term=meniscal%20repair%0A%0ABassett%20FH%20III%2C%20Billys%20JB%2C%20Gates%20HS%20III%3A%20A%20simple%20surgical%20approach%20to%20the%20posteromedial%20ankle%2C%20Am%20J%20Sports%20Med%2021%3A144%2C%201993.)
- Bassett FH III, Gates HS III, Billys JB, et al: Talar impingement by the anteroinferior tibiofi bular ligament, J Bone Joint Surg 72A:55, 1990.
- Bauer M, Jonsson K, Linden B: Osteochondritis dissecans of the ankle: a 20-year follow-up study, J Bone Joint Surg 69B:93, 1987.
- Baums MH, Heidrich G, Schultz W, et al: Autologous chondrocyte transplantation for treating cartilage defects of the talus, J Bone Joint Surg 88A:303, 2006.
- Becker HP, Rosenbaum D, Zeithammel G, et al: Tenodesis versus carbon fi ber repair of ankle ligaments: a clinical comparison, Clin Orthop Relat Res 325:194, 1996.
- Berg EE: The symptomatic os subfi bulare: avulsion fracture of the fi bula associated with recurrent instability of the ankle, J Bone Joint Surg 73A:1251, 1991.
- Berg EE: Intraoperative peroneus brevis tendon rupture: a technique to salvage the graft during ankle ligament reconstruction, Foot Ankle Int 17:349, 1996.
- Berndt AL, Harty M: Transchondral fractures (osteochondritis dissecans) of the talus, J Bone Joint Surg 41A:988, 1959.
- Björkenheim JM, Sandelin J, Santavirta S: Evans’ procedure in the treatment of chronic instability of the ankle, Injury 19:70, 1988.
- Black H: Roentgenographic consideration of the ankle, Am J Sports Med 5:238, 1977.
- Bonnin JG: Injuries to the ankle, London, 1950, William Heinemann. Bonnin M, Tavernier T, Bouysset M: Split lesions of the peroneus brevis tendon in chronic ankle laxity, Am J Sports Med 25:699, 1997.
- Boytim MJ, Fischer DA, Neumann L: Syndesmotic ankle sprains, Am J Sports Med 19:294, 1991.
- Brand RL, Black HM, Cox JS: The natural history of inadequately treated ankle sprain, Am J Sports Med 5:248, 1977.
- Broström L: Sprained ankles: Part III. Clinical observations in recent ligament ruptures, Acta Chir Scand 130:560, 1965.
- Broström L: Sprained ankles: Part V. Treatment and prognosis in recent ligament ruptures, Acta Chir Scand 132:537, 1966.
- Broström L: Sprained ankles: Part VI. Surgical treatment of “chronic” ligament ruptures, Acta Chir Scand 132:551, 1966.
- Brown JE: The sinus tarsi syndrome, Clin Orthop 18:231, 1960.
- Bryant DD, Siegel MG: Osteochondritis dissecans of the talus: a new technique for arthroscopic drilling, Arthroscopy 9:283, 1993.
- Canale ST, Beaty JH: Osteochondral lesions of the talus. In Hamilton WC, ed: Traumatic disorders of the ankle, New York, 1984, Springer-Verlag. Canale ST, Belding RH: Osteochondral lesions of the talus, J Bone Joint Surg 62A:97, 1980.
- Castaing J, Delplace J: Entorses de la cheville, Intérât de l’étude de la stabilité dans le plan sagittal pour le diagnostic de gravité: recherché radiographique du tiroir astragalien antérieur, Rev Chir Orthop 58:51, 1972.
- Cedell CA: Ankle lesions, Acta Orthop Scand 46:425, 1975.
- Chrisman OD, Snook GA: Reconstruction of lateral ligament tears of the ankle, J Bone Joint Surg 51A:904, 1969.
- Clanton TO, Schon LC: Athletic injuries to the soft tissues of the foot and ankle. In Mann RA, Coughlin MJ, eds: Surgery of the foot and ankle, 6th ed, St Louis, 1993, Mosby. Cohen BE, Davis H, Anderson RB: Chevron-type transmalleolor osteotomy—an appnoach to medial talar dome lesions, Orthop Trans 21:43, 1997.
- Cohen BE, Anderson RB: Chevron-type transmalleolar osteotomy: an approach to medial talar dome lesions, Tech Foot Ankle Surg 1:158, 2002.
- Colville MR: Reconstruction of the lateral ankle ligaments, J Bone Joint Surg 76A:1092, 1994.
- Colville MR, Grondel RJ: Anatomic reconstruction of the lateral ankle ligaments using a split peroneus brevis tendon graft, Am J Sports Med 23:210, 1995.
- Cox J: Personal communication, 1989.
- Davidson AM, Steele HD, MacKenzie DA, et al: A review of twenty-one cases of transchondral fracture of the talus, J Trauma 7:378, 1967.
- Dixon DJ, Monroe MT, Gabel SJ, et al: Excrescent lesion: a diagnosis of lateral talar exostosis in chronically symptomatic sprained ankles, Foot Ankle Int 20:331, 1999.
- DuVries HL: Surgery of the foot, St Louis, 1959, Mosby. Elmslie RC: Recurrent subluxation of the ankle-joint, Ann Surg 100:364, 1934.
- Espinosa N, Smerek J, Kadakia AR, Myerson MS: Operative management of ankle instability: reconstruction with open and percutaneous methods, Foot Ankle Clin 11:547, 2006.
- Evans DL: Recurrent instability of the ankle—a method of surgical treatment, Proc R Soc Med 46:343, 1953.
- Evans GA, Hardcastle P, Frenyo AD: Acute rupture of the lateral ligaments of the ankle: to suture or not to suture, J Bone Joint Surg 66B:209, 1984.
- Eyring EJ, Guthrie WD: A surgical approach to the problem of severe lateral instability at the ankle, Clin Orthop Relat Res 206:185, 1986.
- Ferkel RD, Cheng JC: Ankle and
You Might Also Like