INTRODUCTION TO PELVIC RING DISRUPTIONS
Pelvic ring disruptions represent some of the most challenging injuries in orthopaedic trauma, often resulting from high-energy mechanisms such as motor vehicle collisions, crush injuries, or falls from significant heights. The initial assessment and management of these polytraumatized patients require a multidisciplinary approach, with the orthopaedic surgeon playing a critical role in identifying mechanical instability and controlling catastrophic hemorrhage.
The foundation of this assessment is a rigorous, standardized Radiographic Evaluation. Accurate interpretation of pelvic radiographs dictates the immediate resuscitation pathway, the application of damage control orthopaedics, and the formulation of a definitive surgical reconstruction plan.
STANDARD RADIOGRAPHIC PROJECTIONS
The standard radiographic projections required for the comprehensive evaluation of pelvic fractures include an anteroposterior (AP) view of the pelvis, supplemented by the 40-degree caudal inlet and 40-degree cephalad outlet views originally described by Pennal et al.
The Anteroposterior (AP) View
The AP pelvis radiograph is the primary screening tool in the Advanced Trauma Life Support (ATLS) protocol. It provides a global overview of the pelvic ring, allowing the surgeon to assess the symphysis pubis, the iliopectineal and ilioischial lines, the radiographic U (teardrop), the acetabular roofs, and the sacroiliac (SI) joints.
Clinical Pearl: Look for the "L5 transverse process fracture" on the AP view. This is a critical sentinel sign indicating a high-energy posterior pelvic ring disruption, often associated with iliolumbar ligament avulsion and vertical instability.
The Pelvic Inlet View
The inlet view is obtained by directing the X-ray beam 40 degrees caudally (from head to toe) relative to the patient's torso.
- Anatomical Focus: This projection provides an axial perspective of the pelvic ring.
- Pathology Identified: The inlet view is paramount for demonstrating rotational deformity or anteroposterior displacement of the hemipelvis. It clearly delineates internal or external rotation of the hemipelvis, widening of the symphysis pubis, and posterior translation of the SI joint or sacral fractures. It also profiles the sacral promontory and the spinal canal.
The Pelvic Outlet View
The outlet view is obtained by directing the X-ray beam 40 degrees cephalad (from toe to head).
- Anatomical Focus: This projection provides a true orthogonal view of the sacrum and the anterior pelvic ring (pubic rami).
- Pathology Identified: The outlet view is critical for identifying vertical displacement of the hemipelvis. It profiles the sacral foramina, allowing for the identification of transforaminal sacral fractures, and clearly demonstrates superior or inferior migration of the pubic symphysis or posterior pelvic elements.
DYNAMIC RADIOGRAPHIC STRESS TESTING
In cases where the static radiographs are equivocal, particularly in differentiating between Anteroposterior Compression Type I (AP-I) and Type II (AP-II) injuries, dynamic stress testing may be indicated.
The Push-Pull Maneuver
Under continuous fluoroscopic or radiographic control, the examiner applies dynamic forces to the lower extremities to unmask occult instability.
1. The surgeon pushes up (cephalad) on one lower extremity while simultaneously pulling down (caudally) on the contralateral extremity.
2. This maneuver is then reversed.
3. The maximal displacement between the two radiographic films is measured.
Interpretation: If more than 1 cm of cephalad displacement is possible with this test, the fracture is deemed vertically unstable (indicating a complete disruption of the posterior tension band, including the sacrospinous, sacrotuberous, and anterior/posterior sacroiliac ligaments).
Surgical Warning: This test should be performed one time only, with permanent films obtained for accurate measurement of cephalad migration. Repeated testing can exacerbate hemorrhage and soft tissue damage.
Contraindications to Stress Testing
Push-pull testing is strictly contraindicated in the following scenarios:
* Hemodynamic Instability: Acutely injured patients with ongoing shock or active pelvic hemorrhage.
* Zone II or Zone III Sacral Fractures: Dynamic manipulation in the presence of transforaminal or central sacral fractures carries a high risk of iatrogenic neurological injury to the sacral nerve roots.
Note: As the surgeon gains experience in evaluating pelvic injuries and with the ubiquitous availability of high-resolution Computed Tomography (CT), the clinical need for the push-pull test has significantly decreased.
CLASSIFICATION SYSTEMS FOR PELVIC RING FRACTURES
Understanding the relationship between various classification systems is essential for academic discourse and surgical planning. The most commonly utilized systems are the Young-Burgess (mechanistic) and the Tile/OTA (morphological/stability-based) classifications.
Table 56-1: Relationship of Classification Systems
| Stability Level | Bucholz | Tile | OTA/AO | Young-Burgess | Letournel | Denis |
|---|---|---|---|---|---|---|
| STABLE PELVIC RING | I | A1, B2 | 61A, 61B2 | Anterior-posterior compression I Lateral compression I Combined mechanical injury* |
||
| PARTIAL INSTABILITY | II | B1 | 61B2 | Anterior-posterior compression II Lateral compression II Combined mechanical injury* Lateral compression III |
||
| COMPLETE INSTABILITY | III | C | 61C | Anterior-posterior compression III Lateral compression III Vertical shear Combined mechanical injury* |
*Can be associated with all types of instability. OTA, Orthopaedic Trauma Association. Adapted from Olson SA, Burgess A: Classification and initial management of patients with unstable pelvic ring injuries, Instr Course Lect 54:383, 2005.
PELVIC DAMAGE CONTROL
In the hemodynamically unstable polytrauma patient, definitive fixation is deferred in favor of life-saving damage control interventions.
Box 56-2: Pelvic Damage Control Protocols
1. Closed Reduction of the Pelvis at Admission
* Wrapping the pelvis: Utilize a commercial pelvic binder or a simple bed sheet centered over the greater trochanters (NOT the iliac crests).
* Positioning: Apply internal rotation and slight flexion of the knees (often taping the knees or ankles together) to close the anterior pelvic volume.
2. External Fixation
* Anterior External Fixator: Utilized primarily for APC injuries to close the pelvic volume and stabilize the clot. Pins are placed in the iliac crest or supra-acetabular corridors.
* Pelvic C-Clamp: Indicated for posterior ring instability (Vertical Shear or severe APC III) to apply direct compression across the SI joints. Contraindicated in comminuted ilium fractures or transforaminal sacral fractures.
* Pneumatic Antishock Garment (PASG): Historically used, though largely replaced by modern binders and targeted resuscitation.
3. Control of Hemorrhage
* Pre-peritoneal Pelvic Packing: Direct surgical packing of the retrozius space through a midline incision to tamponade venous bleeding (which accounts for 80-90% of pelvic hemorrhage).
* Angiography and Embolization: Indicated for arterial hemorrhage (commonly the superior gluteal or internal pudendal arteries), often identified by a contrast "blush" on CT.
4. Control of Contamination
* Repair of genitourinary and rectal injuries (often requiring diverting colostomy or suprapubic catheters).
* Aggressive surgical débridement of necrotic tissue in the case of open pelvic fractures.
(Adapted from Ertel WK: General assessment and management of the polytrauma patient. In Tile M, Helfet DL, Kellam JF, editors: Fractures of the pelvis and acetabulum, ed 3, Philadelphia, 2003, Lippincott Williams & Wilkins.)
CLINICAL CASE STUDIES & RADIOGRAPHIC EXAMPLES
Case 1: Young-Burgess Anteroposterior Compression Type II (AP II)
An AP II injury is characterized by an "open book" pelvis. The mechanism is a direct anterior-to-posterior force causing symphyseal diastasis (>2.5 cm) and disruption of the anterior sacroiliac, sacrotuberous, and sacrospinous ligaments. The posterior sacroiliac ligaments remain intact, preventing vertical translation but allowing rotational instability.
Preoperative Evaluation:
The preoperative AP view demonstrates significant widening of the symphysis pubis.


Surgical Management:
Treatment typically involves anterior fixation. The patient is positioned supine. A Pfannenstiel approach is utilized to access the symphysis. A multi-hole symphyseal plate is applied with alternating fully threaded cortical screws to reduce and stabilize the diastasis.
Postoperative Imaging:
Postoperative AP, inlet, and outlet views confirm anatomic reduction of the anterior ring and restoration of pelvic volume.


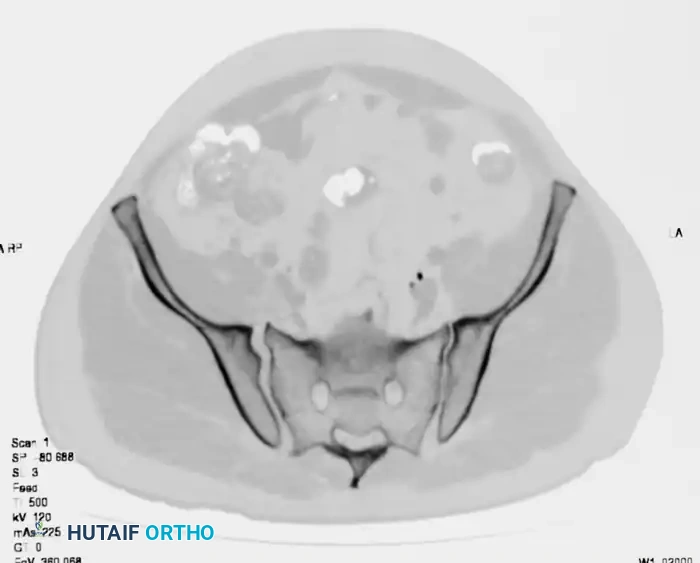
FIGURE 56-43: Young and Burgess anteroposterior type II (AP II) pelvic ring injury with pubic diastasis treated with anterior fixation. A and B, Preoperative views. C-E, Postoperative anteroposterior, inlet, and outlet views.
Case 2: Young-Burgess Lateral Compression Type II (LC II)
An LC II injury results from a lateral force vector. It is characterized by anterior transverse pubic rami fractures combined with a posterior iliac wing fracture (often a "crescent fracture" involving the posterior ilium extending into the SI joint). The hemipelvis is internally rotated.
Preoperative Evaluation:
The standard trauma series (AP, oblique, inlet, and outlet views) reveals the internal rotation deformity and the posterior crescent fracture.




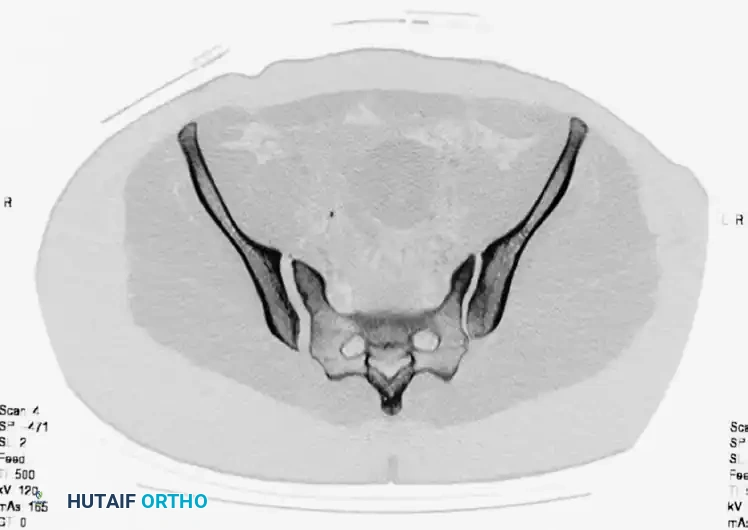
A preoperative CT scan is mandatory to assess the size of the crescent fragment and the integrity of the SI joint articulation.

Surgical Management:
Open reduction and internal fixation (ORIF) is performed. For a large crescent fragment, a posterior approach to the ilium is utilized. The fracture is reduced and stabilized using a 3.5-mm reconstruction plate with lag screws placed between the inner and outer iliac cortical tables.
Postoperative Imaging:
Postoperative films demonstrate restoration of the posterior pelvic ring contour.

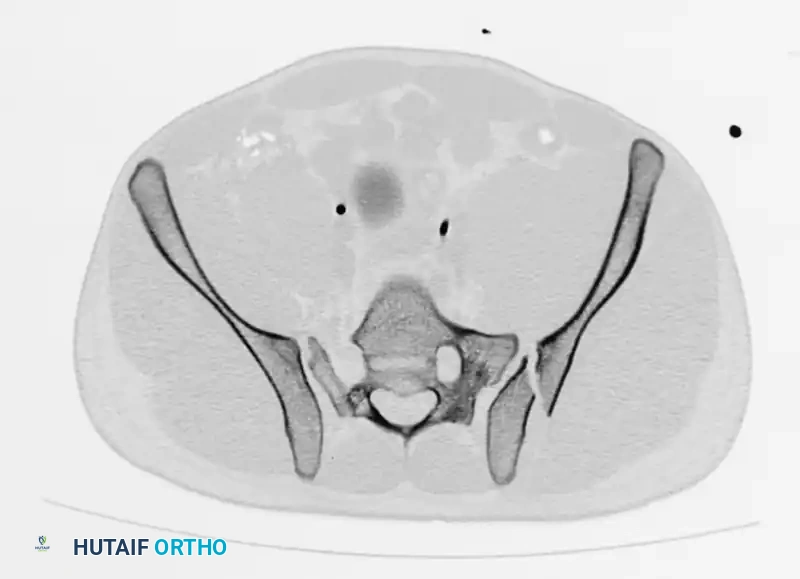
FIGURE 56-44: Young and Burgess lateral compression type II (LC II) pelvic ring injury with posterior crescent fracture. A-D, Preoperative anteroposterior, oblique, inlet, and outlet views. E, Preoperative CT scan. F and G, After open reduction and internal fixation with 3.5-mm reconstruction plate with two lag screws in between iliac cortical tables.
Case 3: Young-Burgess Anteroposterior Compression Type III (AP III)
An AP III injury is a completely unstable pelvic ring disruption. It involves complete disruption of the symphysis pubis (or anterior rami) and complete disruption of both the anterior and posterior sacroiliac ligamentous complexes. The hemipelvis is both rotationally and vertically unstable.
Preoperative Evaluation:
The preoperative AP, inlet, and outlet views demonstrate severe pubic diastasis, bilateral pubic rami fractures, and gross widening/displacement of the posterior SI joints.


Axial CT imaging confirms the complete dissociation of the sacroiliac articulation, highlighting the profound instability of the posterior tension band.

FIGURE 56-45: Young and Burgess anteroposterior type III (AP III) pelvic ring injury with pubic diastasis and bilateral pubic rami fractures. A-C, Preoperative anteroposterior, inlet, and outlet views, respectively. D, Preoperative CT scan.
Surgical Management:
AP III injuries require robust anterior and posterior fixation. Anteriorly, a symphyseal plate or external fixator is applied. Posteriorly, percutaneous iliosacral screws (placed into the S1 and/or S2 vertebral bodies) or posterior tension band plating is required to counteract vertical shear forces and allow for early mobilization.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Following definitive surgical stabilization of pelvic ring injuries, a strict, evidence-based postoperative protocol is essential to prevent hardware failure and ensure optimal functional recovery.
Weight-Bearing Status
- Stable Fixation (e.g., AP II with robust anterior plating): Patients may be allowed touch-down weight-bearing (TDWB) or flat-foot weight-bearing (FFWB) on the affected side for 6 to 8 weeks.
- Unstable/Complex Fixation (e.g., AP III, Vertical Shear): Strict non-weight-bearing (NWB) or TDWB is mandated for a minimum of 8 to 12 weeks to protect the posterior ring fixation (iliosacral screws).
Deep Vein Thrombosis (DVT) Prophylaxis
Pelvic trauma patients are at an exceptionally high risk for venous thromboembolism. Chemical prophylaxis (e.g., Low Molecular Weight Heparin) should be initiated as soon as bleeding is controlled and cleared by the trauma and neurosurgical teams, typically continuing for 4 to 6 weeks post-injury. Mechanical prophylaxis (SCDs) should be used continuously while the patient is immobile.
Radiographic Surveillance
Routine postoperative radiographic surveillance is critical. AP, inlet, and outlet views should be obtained at:
* 2 weeks post-op (to check for early loss of reduction or hardware back-out).
* 6 weeks post-op (to assess early callus formation and maintain alignment).
* 12 weeks post-op (to confirm clinical and radiographic union prior to advancing to full weight-bearing).
Pitfall: Failure to obtain true orthogonal inlet and outlet views during postoperative follow-up can lead to missed subtle vertical or rotational displacement, resulting in malunion, chronic pelvic pain, and leg length discrepancies. Always insist on high-quality, standardized Pennal views.
