Your Complete Humerus Fractures Summary: Diagnosis & Healing
Introduction & Epidemiology
Proximal humerus fractures represent a significant burden on healthcare systems, particularly in an aging population. These injuries are the third most common fracture in individuals over 65 years, following hip and distal radius fractures, and are definitively recognized as a hallmark osteoporotic fracture. The incidence demonstrates a bimodal distribution, occurring in younger, high-energy trauma patients and, more commonly, in elderly individuals following low-energy falls. The increasing life expectancy and prevalence of osteoporosis are contributing to a rising incidence, making comprehensive management strategies critically important.
The inherent biological capacity for healing in the proximal humerus is notable due to its rich vascularity and broad cancellous surfaces, allowing many fractures to be managed effectively without surgical intervention. Stable fracture patterns, particularly those with impaction or minimal displacement, often achieve satisfactory union and functional outcomes. However, the presence of significant displacement, articular involvement, or specific patient factors necessitates careful consideration of operative strategies. The complexity of these injuries is further compounded by the anatomical intricacies and biomechanical forces acting upon the proximal humerus, especially in the context of osteoporotic bone. Challenges in surgical management include precise reduction of small, often comminuted, bone fragments that are subjected to strong muscular forces, and achieving stable fixation in compromised bone stock. A variety of fixation options are available, ranging from plates, screws, and wires to intramedullary devices and arthroplasty.

Fractures of the proximal humerus are typically classified based on their anatomical location and the number of displaced fragments. The Neer classification system, widely utilized, categorizes fractures into 1-part, 2-part, 3-part, and 4-part injuries, considering the surgical neck, anatomical neck, greater tuberosity, and lesser tuberosity as distinct segments. A fragment is considered "displaced" if it exhibits >1 cm of displacement or >45 degrees of angulation. The AO/OTA classification provides a more comprehensive and reproducible description, categorizing fractures by type (A: extra-articular unifocal, B: extra-articular bifocal, C: articular) and subgroups. Both systems aid in prognosis, guiding treatment decisions, and facilitating communication among orthopedic surgeons.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy and biomechanics is paramount for effective diagnosis and management of proximal humerus fractures.
Anatomical Structures
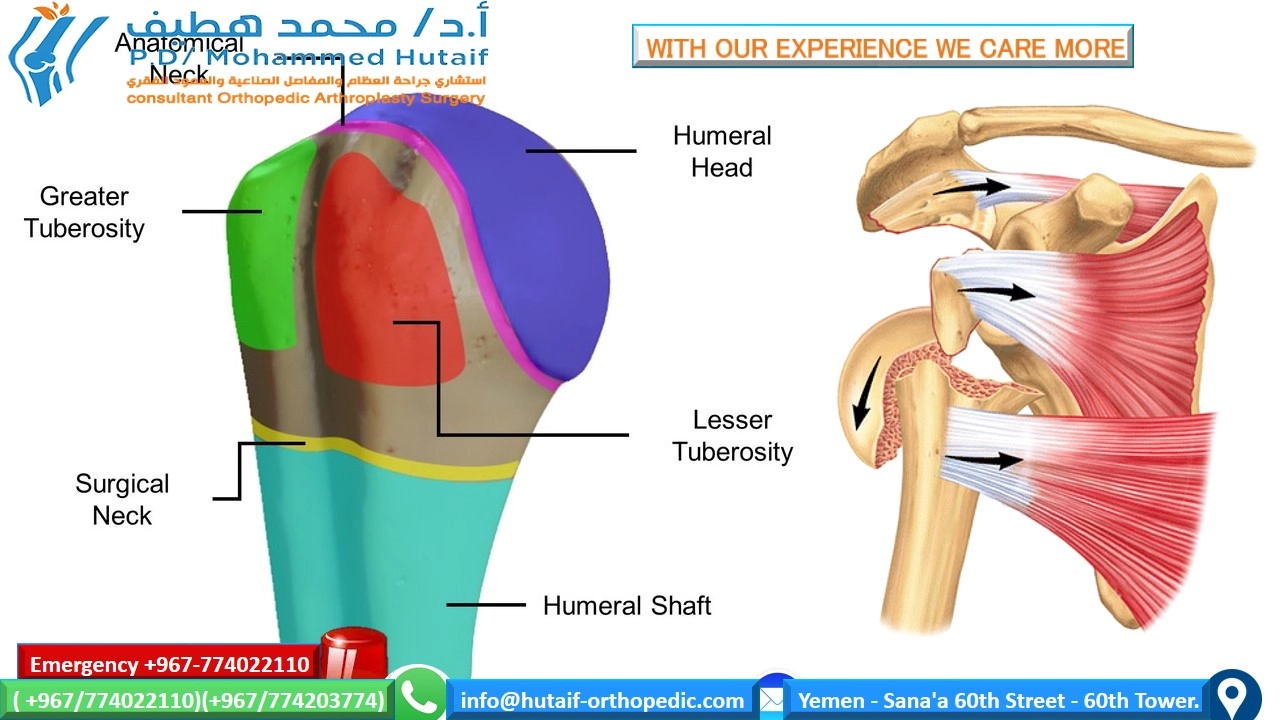
- Humeral Head: The articular surface, articulating with the glenoid fossa. Its smooth contour is vital for shoulder kinematics. Fractures involving the articular surface often carry a higher risk of avascular necrosis (AVN) and post-traumatic arthritis.
- Anatomical Neck: The groove circumscribing the articular head, marking the attachment of the joint capsule. Fractures here, particularly if comminuted, disrupt critical vascular supply.
- Surgical Neck: Located distal to the tuberosities and anatomical neck, it is the most common site of fracture. Its name reflects its frequent involvement in surgical procedures.
- Greater Tuberosity: Located laterally, serving as the insertion point for the supraspinatus, infraspinatus, and teres minor tendons (forming the lateral rotator cuff). Fractures often result in superior and posterior displacement due to rotator cuff pull.
- Lesser Tuberosity: Located medially, serving as the insertion point for the subscapularis tendon (forming the anterior rotator cuff). Fractures typically result in medial and inferior displacement.
- Bicipital Groove: Located between the tuberosities, housing the long head of the biceps tendon. Its integrity is important for biceps function.
Vascular Supply
The vascularity of the humeral head is critical for fracture healing and prevention of AVN. The primary blood supply originates from the anterior and posterior circumflex humeral arteries, branches of the axillary artery.
*
Posterior Circumflex Humeral Artery (PCHA):
The dominant blood supply, particularly its ascending branch which forms the arcuate artery. This vessel typically enters the posteromedial aspect of the surgical neck and ascends to supply the majority of the humeral head. Disruption of this blood supply, especially in multi-part fractures with significant displacement, is a primary risk factor for AVN.
*
Anterior Circumflex Humeral Artery (ACHA):
Contributes to the blood supply, typically sending a deltoid branch and an ascending branch that travels within the bicipital groove.
*
Rotator Cuff Vessels:
Smaller contributions also arise from vessels supplying the rotator cuff tendons.
The posteromedial metaphyseal vessels, supplied by the PCHA, are considered the most crucial for humeral head viability.
Neural Structures
Several nerves are at risk during proximal humerus fractures and surgical interventions:
*
Axillary Nerve:
The most commonly injured nerve, coursing around the surgical neck approximately 5-7 cm distal to the acromion. It innervates the deltoid and teres minor muscles and provides sensation over the lateral shoulder. It is particularly vulnerable during deltopectoral approaches, especially with retractors placed on the inferior border of the deltoid.
*
Musculocutaneous Nerve:
Located more distally, it innervates the biceps and brachialis.
*
Radial Nerve:
Also more distally located, it spirals around the posterior humerus.
*
Suprascapular Nerve:
Located more posteriorly, it is rarely directly involved but can be affected by traction or glenoid fracture-dislocations.
Biomechanics
The proximal humerus is subjected to significant forces from the surrounding musculature.
*
Rotator Cuff:
The supraspinatus, infraspinatus, and teres minor (greater tuberosity) and subscapularis (lesser tuberosity) exert powerful deforming forces, leading to characteristic fracture fragment displacements. The supraspinatus tends to pull the greater tuberosity superiorly.
*
Deltoid:
Exerts an abducting force, which can displace the humeral shaft laterally relative to the head fragment in surgical neck fractures.
*
Pectoralis Major and Latissimus Dorsi:
Contribute to internal rotation and adduction, further influencing fragment alignment in complex fracture patterns.
*
Bone Quality:
In osteoporotic bone, the ability to achieve and maintain stable fixation is compromised. Screws may pull out, and plates may cut through the bone, necessitating specialized implants (e.g., locking plates with calcar screws) or alternative treatment strategies like arthroplasty. The mechanical environment post-fixation significantly influences healing.
Indications & Contraindications
The decision-making process for managing proximal humerus fractures is complex, weighing patient factors, fracture characteristics, and potential risks and benefits of operative versus non-operative treatment.
Operative Indications
-
Displaced 2-part fractures:
- Surgical neck: Significant angulation (>45 degrees) or displacement (>1 cm) in active patients.
- Greater tuberosity: Displacement >5 mm (particularly in younger, active patients due to rotator cuff dysfunction).
- Lesser tuberosity: Less common in isolation, but significant displacement can indicate subscapularis dysfunction.
- Displaced 3-part fractures: Fractures involving the surgical neck and one tuberosity, with significant displacement.
- Displaced 4-part fractures: Highly unstable injuries involving the anatomical neck, surgical neck, and both tuberosities, often with articular displacement. High risk of AVN.
- Head-split fractures: Intra-articular fractures involving a portion of the articular surface, often requiring ORIF or arthroplasty if irreparable.
- Fracture-dislocations: Proximal humerus fracture combined with glenohumeral dislocation.
- Valgus-impacted fractures with articular depression: Although often stable, articular depression greater than 2-3 mm, particularly if involving a significant portion of the articular surface, warrants intervention to prevent post-traumatic arthritis.
- Open fractures: Requires emergent débridement and fixation.
- Vascular compromise: Urgent reduction and fixation or bypass if severe.
- Young, active patients: Higher functional demands and lower risk of osteoporosis typically favor anatomical reduction and stable fixation to restore optimal shoulder function.
- Failure of non-operative management: Persistent pain, malunion, or nonunion.
Non-Operative Indications
- Minimally displaced or stable 1-part fractures: The majority of proximal humerus fractures fall into this category.
- Impacted surgical neck fractures: Stable and minimally angulated.
- Non-displaced tuberosity fractures.
- Elderly, low-demand patients: With displaced fractures, especially 3- and 4-part, where the risks of surgery outweigh potential benefits, or where functional outcome may not differ significantly from non-operative treatment (e.g., PROXIMAL trial findings).
- Significant medical comorbidities: Patients with contraindications to anesthesia or prolonged surgery.
- Poor bone quality: When stable fixation is unlikely to be achieved with ORIF, and arthroplasty is not indicated or desired.
- Patient preference: After thorough discussion of risks, benefits, and expected outcomes of both options.
Relative Contraindications for Surgery
- Severe osteoporosis precluding stable implant fixation.
- Significant medical comorbidities (e.g., cardiac, pulmonary) increasing anesthetic or surgical risk.
- Poor soft tissue envelope or active skin lesions in the surgical field.
- Uncontrolled diabetes.
- Patient non-compliance with post-operative rehabilitation.
- Pre-existing irreparable rotator cuff pathology (may favor arthroplasty upfront).
Absolute Contraindications for Surgery
- Active infection in the surgical field.
- Severe, irreversible neurovascular injury precluding functional recovery of the limb.
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Type | Displaced 2, 3, 4-part fractures; Head-split; Fracture-dislocation; Open fractures; Displaced tuberosity fractures (>5mm/young) | Minimally displaced or stable 1-part fractures; Impacted surgical neck fractures; Non-displaced tuberosity fractures |
| Articular Involvement | Significant articular incongruity (>2-3mm); Valgus-impacted with substantial articular depression | Minimal or no articular involvement |
| Neurovascular | Vascular compromise requiring intervention; Progressive neurological deficit | Stable neurovascular status |
| Patient Factors | Young, active, high-demand patients; No significant comorbidities; Patient expectation of optimal function | Elderly, low-demand patients; Significant medical comorbidities (contraindication to surgery); Poor bone quality precluding stable fixation; Patient preference after shared decision-making |
| Associated Injuries | Polytrauma requiring stabilization; Associated glenoid or humeral shaft fractures | Isolated proximal humerus fracture without other critical injuries |
| Failure of Conservative Tx | Nonunion, malunion with pain/dysfunction | Stable fracture healing progression, improving function |

Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical outcomes for proximal humerus fractures.
Diagnostic Imaging
- Standard Radiographs: Anteroposterior (AP) shoulder, true scapular Y, and axillary views are essential. The axillary view is critical for assessing glenoid articulation and displacement of tuberosities in the sagittal plane. A transthoracic lateral view may be used if the axillary view is unobtainable due to pain or body habitus.
-
Computed Tomography (CT) Scan:
Indispensable for complex fractures, particularly 3- and 4-part injuries, head-split fractures, or fracture-dislocations.
- Provides detailed information on fracture pattern, fragment displacement, articular involvement, and bone loss.
- Helps assess the integrity of the humeral head articular surface and the degree of comminution.
- 3D reconstructions are invaluable for visualizing complex fracture geometry and planning implant placement.
- Magnetic Resonance Imaging (MRI): Less commonly used in acute settings unless soft tissue injuries (e.g., rotator cuff tear, biceps pathology) or occult fractures are suspected or if neurovascular injury is a concern.
Classification and Assessment
- Neer and AO/OTA Classification: Standardized classification systems are used to characterize the fracture and guide treatment decisions. These should be applied consistently during planning.
-
Patient Assessment:
- Age and Functional Demands: Younger, active patients generally warrant more aggressive pursuit of anatomical reduction. Older, lower-demand patients may be candidates for non-operative treatment or arthroplasty.
- Bone Quality: Assess for osteoporosis. DEXA scans may be useful in equivocal cases. Poor bone quality influences implant choice and fixation strategy.
- Comorbidities: Optimize medical conditions pre-operatively. Review anticoagulant and antiplatelet medications; specific protocols should be followed for their management before surgery.
- Neurovascular Status: Thorough pre-operative neurovascular exam is crucial to document any deficits and to monitor for changes post-injury.
Implant Selection
The choice of implant depends on fracture pattern, bone quality, surgeon preference, and patient factors:
*
Plate Osteosynthesis (e.g., locking plates):
Most common for displaced 2-, 3-, and selected 4-part fractures. Locking plates provide angular stability, which is particularly advantageous in osteoporotic bone. Features like calcar screws provide essential medial column support to prevent varus collapse.
*
Intramedullary Nailing:
Less common for complex proximal humerus fractures due to limited control of articular fragments and tuberosities, but can be considered for stable 2-part surgical neck fractures, especially in younger patients, or those with ipsilateral forearm/hand injuries.
*
External Fixation:
Rarely used for definitive management, mostly for temporary stabilization in open fractures or severe soft tissue compromise.
*
Arthroplasty:
*
Hemiarthroplasty:
Indicated for irreparable 4-part fractures, head-split fractures, or high-risk for AVN (e.g., anatomical neck fractures) in patients with an intact or repairable rotator cuff. Requires robust tuberosity repair for good outcomes.
*
Reverse Total Shoulder Arthroplasty (rTSA):
Increasingly utilized for complex 3- and 4-part fractures in elderly patients with poor bone quality, pre-existing rotator cuff deficiency, or in scenarios where tuberosity repair is deemed unlikely to succeed. Offers predictable deltoid-powered elevation.
Patient Positioning
-
Beach Chair Position:
Preferred by many surgeons, offering excellent access to the shoulder and proximal humerus.
- Allows for easy manipulation of the arm, including abduction and rotation.
- Head and torso are elevated, reducing venous pressure and bleeding.
- Care must be taken to prevent brachial plexus traction, excessive cervical spine flexion/extension, and pressure on peripheral nerves.
- The patient is secured to the table to prevent movement during manipulation.
-
Supine Position:
An alternative, particularly for polytrauma patients or those who cannot tolerate the beach chair position.
- May require a bump under the ipsilateral shoulder to elevate it.
- Can be more challenging for accessing posterior aspects or for obtaining certain fluoroscopic views.
- Traction: Manual traction or a fracture table with traction may be used to reduce length and facilitate indirect reduction, particularly in humeral shaft fractures but sometimes useful for initial alignment in complex PHFs.
- C-arm Positioning: The fluoroscopy unit must be positioned to obtain high-quality AP, lateral (true scapular Y), and axillary views intraoperatively without repositioning the patient.
Anesthesia
General anesthesia is typically employed. A regional anesthetic (interscalene brachial plexus block) is often co-administered for post-operative pain control, reducing the need for systemic opioids. Careful communication with the anesthesia team regarding nerve monitoring is essential.
Detailed Surgical Approach / Technique
The primary surgical technique for displaced proximal humerus fractures is Open Reduction and Internal Fixation (ORIF) with a locking plate. Other options, such as intramedullary nailing or arthroplasty, are utilized in specific circumstances.
Deltopectoral Approach (for ORIF)
This is the most common approach, offering broad access to the anterior and lateral aspects of the proximal humerus while preserving the deltoid muscle.
-
Patient Preparation and Draping:
- After anesthesia and positioning (typically beach chair), the entire arm, shoulder, and upper chest are prepped and draped to allow full range of motion of the shoulder and elbow. A sterile stockinette over the arm facilitates manipulation.
-
Skin Incision:
- A curvilinear incision is made, starting from the coracoid process, extending distally along the deltopectoral groove for approximately 8-12 cm. The incision can be extended proximally or distally as needed.
-
Internervous Plane & Dissection:
- Identify the deltopectoral groove , which lies between the deltoid muscle (laterally) and the pectoralis major muscle (medially).
- The cephalic vein typically runs within this groove. It is usually retracted laterally with the deltoid muscle. Meticulous cautery or ligation of small venous branches is performed.
- Deep to the cephalic vein, identify the clavipectoral fascia. Incise this fascia to expose the underlying structures.
- Retract the conjoined tendon (coracobrachialis and short head of biceps) and pectoralis major medially, and the deltoid laterally. Care must be taken to protect the axillary nerve.
-
Exposure and Axillary Nerve Protection:
- The axillary nerve courses approximately 5-7 cm distal to the acromial tip, winding around the surgical neck. It emerges from the quadrangular space and passes inferiorly to the shoulder joint capsule, then curves around the posterior and lateral aspect of the surgical neck to innervate the deltoid.
- Identify and protect the axillary nerve. Aggressive retraction of the deltoid inferiorly can put the nerve at risk. This can be done by palpating the nerve or by dissecting carefully. A limited inferior dissection should be used unless further distal exposure is required.
-
Hematoma Evacuation & Fracture Visualization:
- Evacuate the hematoma to improve visualization. Identify the major fracture fragments: humeral head, surgical neck shaft, greater tuberosity, and lesser tuberosity.
-
Reduction Techniques:
- Ligamentotaxis: Gentle longitudinal traction on the arm can help align the shaft with the humeral head.
- Joy-sticks / K-wires: Sterilized K-wires can be inserted into the humeral head fragment, tuberosities, or humeral shaft to manipulate them into anatomical position.
- Blunt Hohmann Retractors: Can be used to lever and reduce fragments.
- Rotator Cuff Suture Tags: For tuberosity fractures, non-absorbable sutures can be passed through the rotator cuff tendons (supraspinatus, infraspinatus, subscapularis) to aid in reduction and reattachment to the plate.
- Prioritize reduction of the articular segment to the shaft, then tuberosities to the head and shaft.
- Confirm anatomical reduction using intraoperative fluoroscopy (AP, lateral, and axillary views). Ensure the humeral head is not malreduced in varus (increased risk of AVN and screw cutout) or excessive valgus.
-
Plate Application (Locking Plate Osteosynthesis):
- Select an appropriately sized locking plate (e.g., PHILOS plate system).
- Position the plate laterally on the humeral shaft, typically just posterior to the bicipital groove. The superior edge of the plate should be approximately 5-8 mm distal to the superior border of the greater tuberosity to avoid impingement.
- Secure the plate to the humeral shaft with cortical locking screws, ensuring proper length and trajectory.
- Calcar Screws: Crucial for medial column support, especially in osteoporotic bone. These are divergent locking screws directed towards the inferior-medial cortex (calcar region) of the humeral head. They resist varus collapse.
- Head Screws: Insert multiple locking screws into the humeral head, aiming for divergent trajectories to maximize purchase. Avoid placing screws into the articular surface; confirm with fluoroscopy.
- Tuberosity Fixation: If the tuberosities are comminuted or detached, use sutures through the rotator cuff tendons and incorporate them into the plate constructs via plate holes or drill holes in the bone and then tie over the plate, thus compressing them against the humeral head. This provides biological fixation and aids in rotator cuff function.
-
Final Fluoroscopy:
Obtain multiple fluoroscopic views (AP, Y-scapular, axillary) to confirm reduction, implant position, screw length, and absence of intra-articular screw penetration. Perform gentle shoulder range of motion to check for impingement or instability.



Intramedullary Nailing
- Indications: Primarily for selected 2-part surgical neck fractures, particularly in younger patients, or certain metaphyseal comminution patterns. Less effective for complex 3- and 4-part fractures due to poor control of tuberosity and head fragments.
- Technique: Antegrade insertion from the greater tuberosity. Requires reaming and interlocking screws. Advantages include less soft tissue disruption compared to plating, but risks include rotator cuff damage at the entry point and potential for impingement.
Arthroplasty (Hemiarthroplasty or Reverse Total Shoulder Arthroplasty)
- Indications: Irreparable 4-part fractures, head-split fractures, high risk of AVN, severe osteopenia preventing stable ORIF, or failed prior fixation.
- Approach: Typically a deltopectoral approach.
-
Hemiarthroplasty:
- Remove fragmented humeral head.
- Prepare humeral canal for prosthetic stem.
- Select appropriate head size and retroversion.
- Crucial step: Tuberosity repair. The greater and lesser tuberosities are anatomically reduced and securely fixed around the prosthetic stem using strong non-absorbable sutures. This determines post-operative rotator cuff function.
-
Reverse Total Shoulder Arthroplasty (rTSA):
- Remove fragmented humeral head.
- Prepare glenoid for baseplate and glenosphere.
- Prepare humeral canal for reverse stem.
- Component placement: Glenosphere medially offsets, humeral cup creates tension in the deltoid.
-
Tuberosity repair is still performed if possible, but the primary function of the shoulder relies on the deltoid, not the rotator cuff, making it suitable for rotator cuff deficient shoulders or failed tuberosity repair.

Wound Closure
- Meticulous hemostasis.
- Placement of a drain if significant bleeding is anticipated.
- Closure of deep fascia and subcutaneous layers.
- Skin closure.
- Application of a sterile dressing and appropriate immobilization (e.g., sling with or without abduction pillow).
Complications & Management
Proximal humerus fractures, particularly when surgically managed, are associated with a range of potential complications. Proactive recognition and appropriate management are crucial for optimizing patient outcomes.
| Complication | Incidence (Approximate) | Salvage Strategies
Avascular Necrosis (AVN) of the Humeral Head:
*
Incidence:
Highly variable, from 0% in 1-part fractures to over 30% in 4-part fractures.
*
Risk Factors:
Disruption of posteromedial metaphyseal blood supply (ascending branch of PCHA), severe displacement (>1 cm, >45 degrees angulation), comminution of articular fragments, age, and specific fracture patterns (e.g., anatomical neck fractures, true 4-part valgus-impacted fractures).
*
Management:
*
Early:
If identified early and symptomatic, often requires conversion to arthroplasty.
*
Late:
* If asymptomatic, observation. If symptomatic, arthroplasty (hemiarthroplasty or rTSA) is the definitive treatment.
-
Nonunion/Malunion:
- Incidence: Varies significantly based on fracture type, bone quality, and fixation stability. Nonunion rates can be 5-20%.
- Risk Factors: Poor bone quality, inadequate reduction or fixation, early aggressive mobilization, infection, significant comminution, and poor soft tissue coverage. Varus malunion is a common issue with plate fixation.
-
Management:
- Asymptomatic Malunion: Observation.
-
Symptomatic Malunion/Nonunion:
- Revision ORIF with bone grafting: For younger patients with good bone stock.
- Corrective osteotomy: For varus malunion causing impingement.
- Arthroplasty: Hemiarthroplasty or rTSA for elderly patients, especially with significant pain, limited function, or irreparable changes.
-
Hardware Complications:
- Incidence: Common, with screw cutout rates up to 10-15%. Plate impingement can also occur.
- Types: Screw cutout (especially superior screws into the humeral head due to varus collapse or inadequate fixation), plate impingement (superiorly placed plate causing subacromial impingement), screw penetration into the joint, hardware loosening or migration.
-
Management:
- Symptomatic Hardware: Hardware removal once union is achieved.
- Screw Cutout/Failure: Revision ORIF, conversion to arthroplasty (hemi or rTSA), or non-operative management if low demand.
- Intra-articular Screw: Urgent surgical removal to prevent articular damage.
-
Infection:
- Incidence: Relatively low, generally <5% for open fractures, lower for closed.
- Types: Superficial vs. deep.
-
Management:
- Superficial: Oral antibiotics, local wound care.
- Deep: Surgical débridement, intravenous antibiotics. If implants are stable and union is progressing, implant retention may be considered. If unstable or chronic, implant removal and staged revision or arthroplasty may be necessary.
-
Neurovascular Injury:
- Incidence: Axillary nerve injury is the most common, ranging from 5-10%. Brachial plexus or arterial injuries are rare but more severe.
-
Management:
- Axillary Neuropraxia: Often resolves spontaneously. Observation, serial clinical exams, and EMG at 3-6 weeks if no improvement.
- Persistent Neurological Deficit: Nerve exploration and possible repair (grafting or neurolysis) if no signs of recovery.
- Vascular Injury: Urgent surgical exploration and repair.
-
Stiffness/Adhesive Capsulitis:
- Incidence: Very common, affecting up to 20-50% of patients.
- Risk Factors: Prolonged immobilization, inadequate rehabilitation, patient comorbidities (e.g., diabetes), complex fracture patterns, delayed surgery.
-
Management:
- Prevention: Early, controlled, progressive rehabilitation according to established protocols.
- Established Stiffness: Aggressive physical therapy, steroid injections, manipulation under anesthesia (MUA), or arthroscopic capsular release.
-
Rotator Cuff Failure (after tuberosity repair):
- Incidence: Significant challenge, particularly after hemiarthroplasty for fracture.
- Risk Factors: Poor bone quality of tuberosities, inadequate repair technique, early excessive motion.
- Management: Revision repair if possible; conversion to rTSA if irreparable and patient is symptomatic.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as surgical execution for achieving optimal functional outcomes following proximal humerus fracture fixation or arthroplasty. Protocols must be individualized based on the fracture pattern, stability of fixation, bone quality, implant type, and patient's baseline function and compliance.
General Principles
- Pain Management: Effective analgesia is crucial to allow participation in therapy.
- Protection of Healing Structures: Immobilization is used to protect surgical repairs and promote bone healing, but duration is balanced against the risk of stiffness.
- Gradual Progression: Exercises progress from passive to active-assisted, then active, and finally resisted, based on bone healing and soft tissue integrity.
- Patient Education: Crucial for adherence to the protocol and understanding limitations.
Phase I: Immediate Post-Operative (0-6 weeks)
Goal: Pain control, protect healing fracture/repair, minimize stiffness of adjacent joints.
-
Immobilization:
- Sling, typically with an abduction pillow, for comfort and to minimize internal rotation.
- Duration: 4-6 weeks, depending on fracture stability and surgeon preference. Tuberosity fractures or repairs may require longer immobilization.
-
Exercises (Non-shoulder):
- Elbow, wrist, and hand active range of motion (AROM) exercises (e.g., gripping, forearm pronation/supination, elbow flexion/extension).
- Pendulum exercises: Gentle, gravity-assisted circular motions of the arm while leaning forward. Initiated early (within days) to encourage gentle glenohumeral motion without muscle activation.
-
Passive Range of Motion (PROM) (initiated cautiously, often 3-4 weeks post-op for stable fixation):
- External rotation: Limited to 0-30 degrees, often in the scapular plane, using the contralateral arm or therapist assistance.
- Flexion: Limited to 90-120 degrees in the scapular plane, avoiding hyperextension.
- Abduction: Limited to 90 degrees.
- NO active shoulder motion or strengthening during this phase. Avoid lifting, pushing, or pulling.
- Dressing care and wound management.
Phase II: Intermediate (6-12 weeks)
Goal: Restore active range of motion, begin gentle strengthening as fracture healing progresses.
- Discontinue Sling: As tolerated, usually around 6 weeks, allowing for greater freedom of movement.
-
Active-Assisted Range of Motion (AAROM):
- Self-assisted pulley exercises, cane exercises (e.g., forward elevation, external rotation, internal rotation).
- Progressive increase in all planes of motion, aiming for functional range.
-
Active Range of Motion (AROM):
- Initiated cautiously in pain-free ranges once radiographic signs of healing are evident (typically 8-10 weeks).
- Avoid compensatory movements (e.g., shoulder shrugging).
-
Gentle Isometric Strengthening (around 8-10 weeks):
- Against resistance from a wall or therapist, for deltoid, rotator cuff, and periscapular muscles.
- Start with minimal resistance, ensuring no pain or fracture site discomfort.
- Scapular Stabilization Exercises: Important for maintaining proper glenohumeral rhythm.
- NO heavy lifting or unsupported activities.
Phase III: Advanced Strengthening & Return to Activity (>12 weeks)
Goal: Restore full strength, endurance, and return to functional or sport-specific activities.
-
Progressive Strengthening:
- Resistance band exercises (internal/external rotation, abduction, flexion).
- Light free weights, gradually increasing load.
- Eccentric strengthening.
- Focus on global shoulder musculature, including deltoid, rotator cuff, and scapular stabilizers.
- Proprioceptive and Neuromuscular Training: Exercises on unstable surfaces, plyometrics (for athletes).
- Endurance Training:
- Return to Activity: Gradually reintroduce sport-specific or work-related activities. Full return to overhead activities or contact sports may take 6-12 months and depends on bone healing and functional recovery.
- Patient Specific Considerations: For arthroplasty, especially rTSA, protocols may differ significantly, with potentially earlier AROM but specific restrictions on lifting or certain motions to protect the deltoid. Tuberosity repair in hemiarthroplasty requires similar caution regarding active rotator cuff use.
Summary of Key Literature / Guidelines
The management of proximal humerus fractures has evolved considerably, influenced by seminal classification systems, biomechanical studies, and high-quality clinical trials.
-
Neer's Classification (1970s): Malcolm Neer's comprehensive classification provided a framework for understanding fracture patterns and guiding treatment, correlating specific fracture types (e.g., 4-part) with a higher risk of AVN, which often favored arthroplasty. His work significantly influenced the initial shift towards surgical intervention for displaced fractures.
-
Locking Plate Technology (early 2000s): The advent of locking plate systems (e.g., PHILOS plate) marked a significant advancement in ORIF for osteoporotic bone. These plates provide angular stable fixation, reducing screw cutout rates and improving fixation stability compared to conventional plates. This technology fueled an increase in ORIF for complex PHFs.
-
The PROXIMAL Trial (2015, The Lancet ): This landmark randomized controlled trial (RCT) compared surgical fixation with locking plates to non-operative treatment for displaced proximal humerus fractures in older patients.
- Key Finding: The study found no significant difference in shoulder function (measured by Oxford Shoulder Score) at 2 years between surgical and non-surgical groups. Complication rates were higher in the surgical group.
- Implication: This trial critically questioned the routine use of ORIF for many displaced proximal humerus fractures in elderly patients, advocating for a more selective approach and emphasizing the efficacy of non-operative management in well-selected cases.
-
Other RCTs and Meta-analyses: Subsequent trials (e.g., studies on hemiarthroplasty vs. reverse TSA for complex fractures) have further refined treatment algorithms:
- For irreparable 4-part fractures or fracture-dislocations in the elderly, reverse total shoulder arthroplasty (rTSA) has shown increasingly favorable outcomes compared to hemiarthroplasty, particularly in patients with poor bone quality or pre-existing rotator cuff dysfunction, primarily due to more predictable pain relief and active elevation. Tuberosity healing remains a challenge for hemiarthroplasty.
- Meta-analyses generally support the notion that for many displaced 3- and 4-part fractures in the elderly, the benefits of ORIF over non-operative treatment or arthroplasty are not consistently clear, especially when considering complication rates.
-
AAOS Clinical Practice Guidelines: The American Academy of Orthopaedic Surgeons (AAOS) provides evidence-based guidelines, which generally recommend considering non-operative management for many displaced 2-part fractures and highlight the ongoing debate regarding the optimal treatment for 3- and 4-part fractures, emphasizing shared decision-making with patients.
-
Evolution of Treatment Philosophy: The modern approach to proximal humerus fractures is highly individualized. It has shifted from a "one size fits all" surgical paradigm to a more nuanced, evidence-based approach considering:
- Patient age and functional demands: High-demand patients generally benefit more from anatomical restoration.
- Bone quality: Dictates implant choice and stability.
- Fracture pattern and stability: Determines the feasibility of non-operative vs. operative treatment and the type of surgery.
- Comorbidities: Affects surgical risk.
- Surgeon experience: Plays a role in choosing complex procedures like arthroplasty.
- Shared decision-making: Informing patients of the risks, benefits, and uncertainties of each treatment option is paramount.
In conclusion, while the proximal humerus has a robust healing capacity, the diversity of fracture patterns and patient demographics necessitates a sophisticated diagnostic and therapeutic approach. Advances in imaging, implant technology, and a growing body of evidence continue to refine our understanding and management strategies for these challenging injuries.
Clinical & Radiographic Imaging
