Proximal Hamstring Injury Module: Insights courtesy of Gary

Key Takeaway
For anyone wondering about Proximal Hamstring Injury Module: Insights courtesy of Gary, Proximal hamstring injury, common in athletes, encompasses a spectrum of damage to the hamstring muscle complex originating from the ischial tuberosity. This includes strains at the musculotendinous junction, partial tendon tears, or complete avulsions. These injuries typically occur from eccentric activation while under stretch, particularly during high-speed sports, courtesy of gary.
Introduction and Epidemiology
Proximal hamstring injuries represent a complex continuum of pathology that is frequently encountered in both recreational and elite athletic populations. Stretch-induced proximal hamstring injury is exceedingly common among athletes participating in sports that require explosive acceleration, rapid deceleration, or extreme ranges of motion. These injuries do not represent a single clinical entity but rather a continuum of tissue disruption. This spectrum includes low-grade strain at the musculotendinous junction, partial thickness tearing of the tendon, and complete avulsion of the hamstring muscle complex from its origin on the ischial tuberosity.
Historically, proximal hamstring injuries were often underdiagnosed or managed uniformly with conservative measures, leading to suboptimal outcomes in patients with high-grade structural disruption. Recognizing the precise location and severity of the injury is paramount, as the natural history and functional consequences vary significantly based on the degree of tendon retraction and muscle involvement.
Pathogenesis and Mechanism of Injury
The primary mechanism of injury is eccentric activation while the muscle-tendon unit is under extreme stretch. This biomechanical scenario is classically observed when the hip is flexed and the knee is extended. During the terminal swing phase of high-speed running, the hamstrings must eccentrically contract to decelerate the forward progression of the tibia and control knee extension. It is during this high-velocity, high-load eccentric phase that the structural integrity of the musculotendinous junction or the osseous footprint is overwhelmed, resulting in failure.
An additional, albeit less common, mechanism for proximal hamstring injury involves extreme stretch with an uncertain or variable amount of active muscle contraction. This mechanism is frequently observed in sports such as waterskiing, gymnastics, or dancing. In these scenarios, the knee is locked in extension while the hip is subjected to sudden, forceful flexion. This extreme passive stretch can lead to catastrophic failure at the ischial tuberosity, often resulting in complete avulsion of the hamstring complex.
Natural History and Recurrence Rates
The natural history of proximal hamstring injuries varies considerably depending on the anatomic location and the extent of the tear. More proximal injuries, particularly those involving the tendon directly or the osseous footprint, result in a significantly longer time for recovery to pre-injury status. Furthermore, proximal avulsions carry a much greater likelihood of requiring surgical intervention due to the persistent and significant disability associated with loss of the functional anchor point.
Partial or complete hamstring avulsions must be strictly differentiated from strains at the musculotendinous junction. Complete avulsions can be extremely disabling, causing profound symptoms of weakness, loss of eccentric muscle control, and severe cramping, especially during fast-paced running or high-demand activities. Unlike musculotendinous strains, which possess a robust healing capacity, retracted avulsions warrant early surgical intervention to restore the resting length of the muscle and re-establish the biomechanical fulcrum.
Fortunately, the vast majority of proximal hamstring injuries are strains at the musculotendinous junction, which are best managed non-operatively. Strains most often occur in the biceps femoris, and the most common location is near the muscle-tendon junction. The greatest risk factor for injury to the hamstring muscle complex is a history of previous injury to the same anatomic location. Literature indicates the recurrence rate for hamstring injury ranges from 12 percent to 31 percent. Whether this high rate of reinjury is attributed to insufficient rehabilitation, premature return to sport, or the persistence of pre-existing biomechanical risk factors, the treating orthopedic surgeon must possess the ability to accurately assess the degree of injury, understand the reparative process of healing muscle, and implement stringent rehabilitative measures.
Surgical Anatomy and Biomechanics
A thorough understanding of the complex anatomy of the posterior thigh and gluteal region is requisite for accurate diagnosis and safe surgical intervention. The hamstring muscle group consists of three distinct muscles: the biceps femoris, the semitendinosus, and the semimembranosus. The biceps femoris is further divided into a long head and a short head. All three muscles, with the exception of the short head of the biceps femoris, originate from the ischial tuberosity of the pelvis.

Ischial Tuberosity Footprint
The origin of the hamstring complex on the ischial tuberosity is anatomically distinct and highly organized. The biceps femoris long head and the semitendinosus share a common origin, forming the conjoint tendon. This conjoint tendon originates from the posteromedial aspect of the ischial tuberosity. The semimembranosus has a distinct, separate origin located anterolateral to the conjoint tendon on the ischial tuberosity. The semimembranosus footprint is typically broader and more crescent-shaped.
The proximal tendons of the biceps femoris and semimembranosus are unique in their intramuscular architecture. Biomechanical and anatomic studies have shown that these proximal tendons extend distally into the muscle bellies for a considerable distance, approximately 62 percent and 73 percent of their respective muscle lengths. This extensive intramuscular tendinous network explains why musculotendinous junction strains can occur quite distally in the posterior thigh despite being classified as proximal injuries.
Neurovascular Relationships
The most critical anatomic relationship during the surgical approach to the proximal hamstring is the proximity of the sciatic nerve. The sciatic nerve exits the greater sciatic foramen deep to the piriformis muscle and descends into the posterior thigh. At the level of the ischial tuberosity, the sciatic nerve lies immediately lateral to the hamstring origin. The distance from the lateral edge of the ischial tuberosity to the medial border of the sciatic nerve is typically between 1.0 to 1.5 centimeters.
During a traumatic avulsion, the hamstring tendons often retract distally. The ensuing hematoma and subsequent fibrovascular scar tissue can encase the sciatic nerve, leading to secondary tethering or compression. Furthermore, the posterior femoral cutaneous nerve runs superficial to the long head of the biceps femoris and must be protected during the superficial dissection to prevent painful postoperative neuromas.
The hamstrings are biarticular muscles, meaning they cross and act upon both the hip and the knee joints. This biarticular nature is fundamental to their biomechanical function and their susceptibility to injury. They function as primary hip extensors and knee flexors. Their dual-joint spanning configuration places them at high risk for stretch-induced failure when simultaneous extreme hip flexion and knee extension occur.
Indications and Contraindications
The decision-making process regarding the management of proximal hamstring injuries hinges on the precise anatomic diagnosis, the degree of tendon retraction, the chronicity of the injury, and the functional demands of the patient. Strains at the musculotendinous junction are universally managed non-operatively. Conversely, complete avulsions with significant retraction in active individuals are generally considered absolute indications for surgical repair.
Operative Versus Non Operative Management Parameters
| Variable | Non Operative Management | Operative Management |
|---|---|---|
| Injury Type | MTJ strains, isolated single-tendon tears | 2-tendon or 3-tendon complete avulsions |
| Retraction | Minimal or < 2 cm | > 2 cm retraction |
| Patient Profile | Low demand, elderly, significant medical comorbidities | High demand, athletes, active middle-aged individuals |
| Chronicity | Acute low-grade injuries | Acute avulsions (< 4 weeks) or chronic symptomatic tears |
| Neurologic Status | Intact | Sciatic nerve symptoms (radiculopathy, tethering) |
| Bony Involvement | Minimally displaced avulsion fractures | Displaced bony avulsions (> 2 cm) |
Contraindications to surgical intervention include advanced patient age with low functional demands, severe medical comorbidities precluding safe prone anesthesia, active local or systemic infection, and chronic asymptomatic tears discovered incidentally. In cases of chronic, massive retraction where the muscle has undergone severe fatty infiltration and atrophy, primary repair may be impossible, and conservative management or complex reconstruction using allograft may be the only viable options.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for a successful surgical outcome. The cornerstone of preoperative evaluation is high-resolution Magnetic Resonance Imaging.
Clinical Evaluation and Imaging
Proximal hamstring injury typically results in the sudden onset of sharp pain in the posterior proximal thigh during athletic competition or training. Severe injury, such as a complete avulsion, may present with a visible deformity, significant posterior thigh swelling, extensive ecchymosis tracking down to the popliteal fossa, and a palpable defect at the ischial origin.
With the patient lying prone and the hamstrings activated via resisted knee flexion, careful palpation of the proximal hamstring origin is undertaken. A palpable defect just distal to the ischial tuberosity strongly implies a proximal avulsion. Focal tenderness to palpation and pain on provocation with resisted knee flexion are consistent findings. Avulsions cause profound symptoms of weakness and loss of eccentric muscle control.

MRI is the gold standard for defining the injury architecture. Fluid-sensitive sequences (T2 fat-suppressed or STIR) in axial, coronal, and sagittal planes are mandatory. The surgeon must evaluate the number of tendons involved (conjoint tendon vs. semimembranosus), the exact distance of distal retraction from the ischial tuberosity, and the integrity of the muscle belly.
Recovery time has been correlated directly with the percentage of muscle involved by measuring the cross-sectional area or the longitudinal length of abnormal muscle signal on MRI. Injuries involving over 50 percent of the cross-sectional area result in a recovery period longer than 6 weeks, whereas normal or near-normal imaging findings result in a recovery period of approximately 1 week. Furthermore, the MRI must be scrutinized for the position of the sciatic nerve relative to the hematoma or retracted tendon stump.
Positioning and Operating Room Setup
Surgical repair of proximal hamstring avulsions is performed with the patient under general anesthesia. The patient is positioned prone on a radiolucent operating table. Careful padding of all bony prominences is mandatory.
The surgical table is often configured to allow for independent manipulation of the operative leg. A "jackknife" position is generally avoided as it places the hamstrings under tension. Instead, the patient is positioned flat, and a sterile bump or specialized leg positioner is used to maintain the knee in approximately 30 to 45 degrees of flexion. Flexing the knee and slightly extending the hip reduces tension on the hamstring complex, facilitating mobilization and anatomic reduction of the retracted tendon to the ischial footprint. Intraoperative fluoroscopy should be available to confirm the location of the ischial tuberosity and verify suture anchor placement.
Detailed Surgical Approach and Technique
The surgical approach to the proximal hamstring requires meticulous dissection to avoid iatrogenic injury to the sciatic nerve and to adequately mobilize the retracted tendon.
Incision and Superficial Dissection
The choice of incision depends on the chronicity of the injury and the degree of retraction. For acute injuries with minimal retraction, a transverse incision placed directly within the gluteal crease offers an excellent cosmetic result. However, for chronic injuries or acute injuries with significant distal retraction (> 3 cm), a longitudinal incision is preferred. The longitudinal incision begins at the level of the gluteal crease, centered over the ischial tuberosity, and extends distally along the posterior midline of the thigh.

Subcutaneous dissection is carried down to the fascia lata. Care must be taken during this superficial dissection to identify and protect the posterior femoral cutaneous nerve, which courses deep to the fascia lata but sends sensory branches superficially. The fascia is incised longitudinally in line with the skin incision.
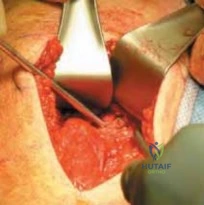
Deep Dissection and Sciatic Nerve Identification
Once the fascia is opened, the inferior border of the gluteus maximus is identified and retracted superiorly. This exposes the subgluteal space and the proximal hamstring anatomy. In the setting of an acute avulsion, a large hematoma is typically encountered. This hematoma should be carefully evacuated to improve visualization.
The most critical step of the procedure is the positive identification and protection of the sciatic nerve. The nerve is consistently found immediately lateral to the ischial tuberosity and deep to the biceps femoris. The surgeon must locate the nerve proximally, in an area of uninjured tissue, and trace it distally past the zone of injury. In chronic cases, dense fibrovascular scar tissue often encases the nerve, tethering it to the retracted tendon stump. A meticulous neurolysis using surgical loupes and micro-dissection techniques is mandatory to free the nerve and prevent postoperative neuropathic pain or motor deficits.
Tendon Mobilization and Footprint Preparation
After the sciatic nerve is protected, attention is turned to the avulsed hamstring tendons. The proximal stump of the tendon is identified and grasped with a heavy traction suture or an Allis clamp. Adhesions between the tendon and the surrounding fascia or the sciatic nerve are sharply released. The knee is flexed to 45 degrees to relax the muscle-tendon unit, allowing the surgeon to assess the excursion of the tendon and its ability to reach the ischial footprint without excessive tension.
The ischial tuberosity footprint is then prepared. Soft tissue debris and remnants of the native tendon are debrided using an electrocautery and a periosteal elevator. The cortical surface of the ischial tuberosity is lightly decorticated using a high-speed burr or an osteotome to expose bleeding cancellous bone. This decortication is crucial for optimizing the biological environment for tendon-to-bone healing.
Suture Anchor Fixation and Closure
Fixation is typically achieved using multiple suture anchors. Depending on the size of the footprint and the number of avulsed tendons, two to four double- or triple-loaded suture anchors are utilized. The anchors are placed into the decorticated ischial tuberosity. Biomechanical studies suggest that a dual-row configuration or a broad footprint placement optimizes contact area and load to failure, though single-row configurations with robust anchors are frequently sufficient.

The sutures are then passed through the proximal end of the avulsed tendon. A locking stitch configuration, such as a Krackow or a modified Mason-Allen technique, is imperative to secure a strong hold on the tendinous tissue and prevent suture pull-through. The sutures are sequentially tied while an assistant maintains the knee in 45 degrees of flexion and applies proximal traction on the tendon to ensure anatomic reduction against the decorticated bone.
Following secure fixation, the surgical site is copiously irrigated. The fascial layer is closed meticulously over a closed-suction drain to prevent postoperative hematoma formation, which can compress the sciatic nerve. The subcutaneous tissues and skin are closed in a standard layered fashion.
Complications and Management
Surgical repair of proximal hamstring avulsions is a highly successful procedure, but it is not without significant risks. The proximity of major neurovascular structures and the high biomechanical forces across the repair site necessitate careful surgical technique and strict postoperative compliance.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology and Presentation | Management and Salvage Strategy |
|---|---|---|---|
| Sciatic Nerve Palsy | 2% - 5% | Iatrogenic injury during dissection, retraction neuropraxia, or postoperative hematoma compression. Presents as foot drop or severe radicular pain. | Immediate evaluation. If hematoma is suspected, emergent evacuation. If intraoperative stretch, observe (usually resolves in 3-6 months). Gabapentinoids for neuropathic pain. |
| Re-rupture | 5% - 8% | Non-compliance with postoperative bracing, premature return to sport, or inadequate fixation. Presents as sudden pop and recurrent weakness. | Revision surgery is technically demanding. May require Achilles tendon allograft augmentation if native tissue is poor. |
| Infection | 1% - 3% | Proximity to the perianal region increases risk. Presents as erythema, drainage, or systemic signs. | Superficial: Oral antibiotics. Deep: Emergent surgical debridement, implant retention if stable, targeted IV antibiotics. |
| Ischial Apophysitis / Bursitis | 10% - 15% | Prominent suture knots, inadequate decortication, or altered biomechanics. Presents as pain with sitting. | Conservative management: NSAIDs, targeted corticosteroid injections, cushion seating. Rarely requires hardware removal. |
| Deep Vein Thrombosis (DVT) | 1% - 2% | Prone positioning, lower extremity immobilization. Presents as calf swelling and pain. | Routine mechanical prophylaxis post-op. Chemical prophylaxis in high-risk patients. Treat with therapeutic anticoagulation if diagnosed. |
Post Operative Rehabilitation Protocols
Rehabilitation following proximal hamstring repair is a lengthy and highly structured process. The protocol must balance the need to protect the healing tendon-to-bone interface with the necessity of preventing severe muscle atrophy and joint contracture.
Phased Recovery Strategy
Phase 1: Maximum Protection (Weeks 0 to 6)
The primary goal during this phase is to protect the surgical repair. The patient is placed in a hinged knee brace locked at 30 to 40 degrees of flexion to remove tension from the hamstring origin. Weight-bearing is strictly limited to toe-touch or non-weight-bearing using crutches. Active hamstring contraction is entirely prohibited. Passive range of motion of the knee is permitted within a restricted arc (e.g., 40 to 90 degrees), strictly avoiding simultaneous hip flexion and knee extension.
Phase 2: Moderate Protection and Early Motion (Weeks 6 to 12)
At 6 weeks, the brace is gradually unlocked to allow full knee extension, and weight-bearing is progressively advanced to full weight-bearing as tolerated. The focus shifts to restoring normal gait mechanics. Gentle, active-assisted and active range of motion exercises are initiated. Isometric hamstring contractions are introduced at various angles of knee flexion, ensuring the hip remains in a neutral or extended position.
Phase 3: Strengthening and Proprioception (Weeks 12 to 16)
Once full, pain-free range of motion is achieved, concentric strengthening is initiated. Exercises such as prone leg curls and bridging are utilized. As tolerance improves, eccentric strengthening is cautiously introduced. Eccentric loading is critical for restoring the muscle's ability to absorb energy during the deceleration phase of the gait cycle, thereby reducing the risk of reinjury.
Phase 4: Return to Sport (Weeks 16 to 24+)
The final phase focuses on sport-specific functional training. Advanced plyometrics, agility drills, and high-speed running are incorporated. Return to unrestricted athletic competition is typically permitted between 5 and 6 months postoperatively, contingent upon the patient demonstrating symmetrical hamstring strength (at least 90% of the contralateral limb on isokinetic testing), no pain with explosive movements, and psychological readiness.
Summary of Key Literature and Guidelines
The management of proximal hamstring injuries has evolved significantly over the past two decades, driven by advancements in MRI diagnostics and improved surgical techniques.
Classic studies by Wood et al. established the foundation for recognizing the severe functional deficits associated with non-operative management of complete 3-tendon avulsions. Their work demonstrated that surgical repair yields superior outcomes regarding return to pre-injury activity levels and isokinetic strength restoration compared to conservative care in the athletic population.
Cohen and colleagues provided critical insights into the MRI evaluation of these injuries. They established the correlation between the cross-sectional area of muscle involvement and the anticipated recovery time for non-operative strains. As noted, injuries involving over 50 percent of the cross-sectional area reliably dictate a recovery period extending beyond 6 weeks, providing surgeons with a valuable prognostic tool for counseling patients.
Furthermore, Lempainen's extensive work on both acute and chronic proximal hamstring ruptures highlighted the importance of early surgical intervention. Their data indicated that while chronic repairs are feasible and significantly improve function, acute repairs (performed within 4 weeks of injury) result in anatomically superior reductions, lower rates of sciatic nerve tethering, and a higher percentage of athletes successfully returning to elite-level competition.
Finally, the high recurrence rate of 12 percent to 31 percent reported by Peterson underscores the necessity of strict adherence to multiphase rehabilitation protocols. The literature universally supports the concept that premature return to high-speed eccentric loading is the primary driver of catastrophic re-rupture, emphasizing the surgeon's role in moderating patient expectations and enforcing objective functional criteria before clearing an athlete for return to play.
Clinical & Radiographic Imaging
