Proximal Hamstring Injury: Understand & Recover Effectively
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Proximal Hamstring Injury: Understand & Recover Effectively. A **proximal hamstring injury** is a stretch-induced injury common in athletes, ranging from a strain at the musculotendinous junction to a partial tear or complete avulsion of the hamstring complex from the ischial tuberosity. These injuries often result from eccentric activation under stretch, with avulsions being more severe and potentially requiring surgical intervention compared to more common musculotendinous strains.
Introduction and Epidemiology
Stretch-induced proximal hamstring injuries represent a significant and frequently encountered pathology within sports medicine and orthopedic surgery. These injuries exist along a continuum, ranging from low-grade strains at the musculotendinous junction to partial interstitial tears, and ultimately to complete avulsions of the hamstring muscle complex from the ischial tuberosity. The natural history of these injuries varies considerably based on the anatomical location and the degree of structural failure. More proximal injuries, particularly complete avulsions, correlate with prolonged recovery periods, significant functional deficits, and a higher likelihood of requiring surgical intervention.
Epidemiologically, these injuries are predominantly seen in athletes participating in sports that require high-speed sprinting, rapid acceleration, or extreme hip flexion combined with knee extension. The principal mechanism of injury involves eccentric activation of the hamstring complex while under significant stretch. This typically occurs during the late swing phase of the gait cycle in sprinting, as the hamstrings contract eccentrically to decelerate the extending tibia and control hip flexion. An alternative, albeit less common, mechanism involves an extreme, sudden stretch with variable muscle activation, classically described in waterskiing or competitive dancing, where the knee is forcefully extended while the hip is acutely flexed.
The greatest risk factor for a proximal hamstring injury is a history of a previous hamstring strain. Recurrence rates are reported to range from 12% to 31%. This high rate of reinjury underscores the necessity for orthopedic surgeons to accurately assess the degree of tissue disruption, understand the biological reparative processes of skeletal muscle and tendon, and implement precise surgical and rehabilitative strategies.
Surgical Anatomy and Biomechanics
A thorough understanding of the proximal hamstring anatomy is paramount for both accurate diagnosis and safe surgical intervention, particularly given the proximity of critical neurovascular structures. The hamstring muscle group consists of three primary bellies: the biceps femoris, the semitendinosus, and the semimembranosus. With the exception of the short head of the biceps femoris, which originates from the linea aspera of the posterior femur, all hamstring muscles originate from the ischial tuberosity of the pelvis.
The Ischial Footprint
The origin on the ischial tuberosity is anatomically distinct. The long head of the biceps femoris and the semitendinosus form a conjoint tendon that originates from the inferomedial aspect of the upper ischial tuberosity. The semimembranosus has a distinct, independent origin located superolateral and slightly anterior to the conjoint tendon origin. The footprint of the semimembranosus is crescent-shaped, whereas the conjoint tendon footprint is more oval.
Musculotendinous Architecture
The hamstrings are biarticular muscles, crossing both the hip and the knee joints, which subjects them to extreme mechanical disadvantage and high eccentric loads. The proximal tendons of the biceps femoris and semimembranosus extend significantly into their respective muscle bellies. Studies demonstrate that the proximal tendon of the biceps femoris extends for approximately 62% of the muscle belly length, while the semimembranosus tendon extends for about 73%. This extensive musculotendinous integration explains why strains most frequently occur at the musculotendinous junction rather than as pure mid-substance muscle tears.
Neurovascular Relationships
The most critical anatomical relationship during surgical exploration of the proximal hamstring is the sciatic nerve. The sciatic nerve exits the greater sciatic foramen deep to the piriformis and descends immediately lateral to the ischial tuberosity and the proximal hamstring origin. On average, the sciatic nerve lies merely 1.2 to 2.0 centimeters lateral to the lateral margin of the ischial footprint. In the setting of a complete avulsion, the resulting hematoma and subsequent scar tissue can tether the sciatic nerve to the retracted tendon stump, significantly altering this normal anatomical relationship and increasing the risk of iatrogenic injury during dissection.
Indications and Contraindications
The management of proximal hamstring injuries requires a nuanced approach based on the chronicity of the injury, the number of tendons involved, the degree of retraction, and the functional demands of the patient. Strains at the musculotendinous junction are almost universally managed non-operatively, whereas complete avulsions with significant retraction in active individuals typically warrant surgical repair to restore functional strength and prevent chronic disability.
Operative vs Non Operative Management Parameters
| Variable | Operative Indications | Non-Operative Indications |
|---|---|---|
| Injury Type | Complete 3-tendon avulsion | MTJ strains (Grade I-II) |
| Tendon Involvement | 2 or more tendons avulsed | Isolated single tendon tear |
| Retraction Distance | > 2 cm of retraction | < 2 cm of retraction |
| Symptomatology | Sciatic nerve tethering symptoms | Minimal weakness in deep flexion |
| Chronicity | Acute (< 4 weeks) or symptomatic chronic | Acute without significant retraction |
| Patient Profile | High-demand athletes active individuals | Low-demand or significant comorbidities |
Contraindications to surgical intervention include severe medical comorbidities precluding anesthesia, local soft tissue infection, and isolated single-tendon injuries with minimal retraction in low-demand patients. Furthermore, surgical intervention for chronic injuries (greater than 6 months) must be carefully weighed against the high likelihood of requiring allograft reconstruction and the increased risk of sciatic nerve complications due to dense perineural fibrosis.
Pre Operative Planning and Patient Positioning
Thorough preoperative clinical and radiographic evaluation is necessary to formulate an appropriate surgical strategy. The clinical examination typically reveals a sudden onset of severe pain in the posterior proximal thigh. In cases of complete avulsion, a visible deformity, extensive ecchymosis, and a palpable defect distal to the ischial tuberosity are pathognomonic.
Clinical Examination Techniques
With the patient lying prone, palpation of the proximal hamstring origin is performed while the patient actively engages the hamstrings against resistance. A palpable defect implies proximal retraction of the tendon. Provocative testing with resisted knee flexion, particularly with the hip in varying degrees of flexion, will elicit profound weakness and pain in the setting of an avulsion.
Advanced Imaging Protocols
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating proximal hamstring injuries. T2-weighted fat-suppressed sequences in both the axial and coronal planes are essential for assessing the extent of tendon involvement, the exact distance of retraction, and the quality of the remaining muscle tissue. In acute avulsions, a large hematoma is often visible between the ischial tuberosity and the retracted tendon stump. The radiologist and surgeon must meticulously evaluate the axial images to determine the proximity of the retracted stump to the sciatic nerve.

Patient Positioning Considerations
Surgical intervention is performed with the patient in the prone position. Optimal positioning involves placing the patient on a specialized operative table (such as a Jackson table) with all bony prominences meticulously padded. The knee on the operative side should be draped free to allow for intraoperative flexion. Flexing the knee to 90 degrees and slightly extending the hip significantly reduces tension on the hamstring complex, facilitating mobilization of the retracted tendon and anatomical reduction to the ischial footprint.
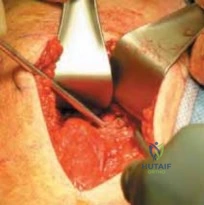
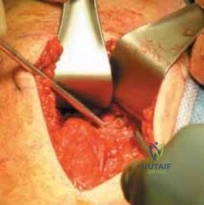
Detailed Surgical Approach and Technique
The surgical repair of a proximal hamstring avulsion is a technically demanding procedure that requires meticulous dissection, precise neurolysis, and robust osseous fixation. The procedure can be broadly divided into exposure, sciatic nerve identification, tendon mobilization, footprint preparation, and fixation.
Incision and Superficial Dissection
A transverse incision within the gluteal crease is often utilized for aesthetic purposes in acute injuries with minimal retraction. However, for chronic injuries or acute injuries with retraction exceeding 3 to 4 centimeters, a longitudinal incision centered over the palpable tendon stump and extending proximally toward the ischial tuberosity provides superior extensile exposure.
The subcutaneous tissue is divided to expose the fascia overlying the gluteus maximus. The inferior border of the gluteus maximus is identified and mobilized superiorly. In some cases, the gluteal fascia must be incised to allow adequate superior retraction of the muscle belly, thereby exposing the ischial tuberosity and the deep space containing the avulsed tendons.
Deep Dissection and Sciatic Nerve Neurolysis
The most critical step of the procedure is the identification and protection of the sciatic nerve. The nerve is typically located deep and lateral to the ischial tuberosity. In acute cases, the nerve may be obscured by hematoma; in chronic cases, it is often encased in dense fibrotic scar tissue tethering it to the retracted tendon stump.
Dissection must proceed with extreme caution using blunt and sharp techniques. The surgeon should identify the nerve in an area of normal anatomy, typically distal to the zone of injury, and trace it proximally. Complete neurolysis is mandatory to ensure the nerve is free from the tendon stump and will not be subjected to tension during tendon reduction.
Tendon Mobilization and Preparation
Once the sciatic nerve is safely isolated and protected, attention is turned to the retracted tendon stump. The stump is mobilized by releasing any peripheral adhesions. A heavy, non-absorbable suture (e.g., #2 or #5 high-strength polyethylene) is woven through the distal tendon stump using a locked Krackow or similar grasping configuration. Multiple passes are made to ensure a secure hold on the tendinous tissue. Traction is then applied to the sutures while the knee is flexed to assess the excursion of the tendon and its ability to reach the ischial footprint.
Ischial Tuberosity Footprint Preparation
The ischial tuberosity must be cleared of all soft tissue debris and hematoma. A curette or a high-speed burr is utilized to lightly decorticate the anatomical footprint, exposing bleeding cancellous bone to optimize the biological environment for tendon-to-bone healing. The surgeon must remain cognizant of the anatomical origins, ensuring the conjoint tendon and semimembranosus are reduced to their respective anatomical locations.

Suture Anchor Fixation Technique
Fixation is typically achieved using multiple suture anchors. Depending on the size of the footprint and the number of avulsed tendons, two to four double- or triple-loaded suture anchors (typically 4.5 mm to 5.5 mm in diameter) are placed into the decorticated ischial tuberosity.
The sutures from the anchors are passed through the mobilized tendon stump using a free needle. A combination of horizontal mattress and simple stitches is utilized to compress the tendon broadly against the bone. The sutures are tied with the knee flexed to 45-90 degrees to eliminate tension.
Management of Chronic Retracted Tears
In chronic cases where the tendon cannot be mobilized to the ischial tuberosity despite extensive soft tissue release and maximal knee flexion, allograft reconstruction is indicated. Achilles tendon allograft with a calcaneal bone block is a preferred option. The bone block is fixed to the ischial tuberosity using cancellous screws, and the tendinous portion of the allograft is woven into the native hamstring stump using a Pulvertaft weave or side-to-side anastomosis, supplemented with heavy non-absorbable sutures.
Complications and Management
Surgical repair of proximal hamstring avulsions carries a unique set of potential complications, primarily related to the complex regional anatomy and the high mechanical forces subjected to the repair during rehabilitation.
Common Surgical Complications
| Complication | Incidence Range | Management and Salvage Strategy |
|---|---|---|
| Sciatic Neuropraxia | 2% - 5% | Observation, gabapentinoids. Usually resolves within 3-6 months. |
| Sciatic Nerve Tethering | Unknown (Higher in chronic) | Surgical exploration, neurolysis, and potential wrapping with nerve conduit. |
| Infection | 1% - 3% | Prompt irrigation and debridement, targeted intravenous antibiotics. |
| Deep Vein Thrombosis | 1% - 2% | Chemical prophylaxis post-operatively, therapeutic anticoagulation if DVT confirmed. |
| Re-rupture | 2% - 6% | Revision repair vs allograft reconstruction based on tissue quality. |
| Ischial Apophysitis Pain | 5% - 10% | Activity modification, NSAIDs, localized corticosteroid injection (avoiding tendon). |
Sciatic nerve injury remains the most devastating potential complication. Neuropraxia may occur due to aggressive retraction during surgery or tension placed on the nerve during the reduction of a chronically retracted tendon. Postoperative sciatic nerve symptoms must be evaluated promptly. If an iatrogenic structural injury to the nerve is suspected, early re-exploration is mandatory.
Re-rupture is typically the result of non-compliance with postoperative rehabilitation protocols, specifically premature eccentric loading or forced hip flexion with an extended knee. Revision surgery is technically demanding due to compromised tissue quality and often necessitates allograft augmentation.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation following proximal hamstring repair is a delicate balance between protecting the surgical repair and preventing debilitating arthrofibrosis and muscle atrophy. A structured, phased protocol is essential for optimal outcomes.
Phase One Protection Phase
The initial 4 to 6 weeks post-surgery focus entirely on protecting the repair. The patient is placed in a hinged knee brace locked at 40 to 60 degrees of flexion, or a custom hip-knee-ankle orthosis that restricts hip flexion and maintains knee flexion. Weight-bearing is strictly restricted to toe-touch or non-weight-bearing with crutches. Passive range of motion of the knee is permitted within safe, pain-free limits, strictly avoiding simultaneous hip flexion and knee extension.
Phase Two Early Range of Motion
From weeks 6 to 12, the focus shifts to restoring normal range of motion. The brace is gradually unlocked to allow progressive knee extension, typically unlocking 10 to 15 degrees per week. Weight-bearing is progressed to full as tolerated once the brace is discontinued. Active knee flexion and gentle isometric hamstring contractions are initiated. The patient may begin stationary cycling with low resistance.
Phase Three Strengthening Phase
Beginning around week 12, provided the patient has achieved full, pain-free range of motion, strengthening exercises are introduced. The initial focus is on concentric hamstring strengthening and gluteal activation. As the patient progresses, eccentric strengthening—which is critical for preventing reinjury—is carefully integrated. Exercises such as Nordic hamstring curls are introduced late in this phase and advanced based on patient tolerance and strength symmetry.
Phase Four Return to Sport
Return to sport is typically permitted between 5 and 9 months postoperatively. Criteria for return to unrestricted athletic activity include a lack of pain with functional movements, full range of motion, and isokinetic hamstring strength testing demonstrating at least 85% to 90% symmetry compared to the contralateral uninjured limb. The athlete must successfully complete a sport-specific functional progression, including sprinting, cutting, and deceleration drills, without apprehension or compensatory mechanics.
Summary of Key Literature and Guidelines
The academic literature strongly supports the surgical repair of acute, complete proximal hamstring avulsions in active patients. Systematic reviews by Harris et al. and Cohen & Bradley have consistently demonstrated that acute repair (performed within 4 weeks of injury) yields significantly better clinical outcomes, higher rates of return to pre-injury levels of sport, and lower complication rates compared to delayed or chronic repairs.
Lempainen et al. evaluated the long-term outcomes of surgical repair and found that patients maintained excellent subjective and objective functional scores at a minimum of five years postoperatively, with very low rates of re-rupture. The literature also emphasizes the critical nature of the sciatic nerve during these procedures; Wood et al. highlighted that delayed surgical intervention exponentially increases the difficulty of neurolysis and the subsequent risk of postoperative sciatic neuropathy.
Current orthopedic guidelines recommend a high index of suspicion for complete avulsions in athletes presenting with posterior thigh pain and weakness following an eccentric loading event. Early MRI evaluation is critical to delineate the injury pattern, and prompt surgical referral is advocated for multi-tendon avulsions with retraction to optimize biological healing and functional recovery.
Clinical & Radiographic Imaging