POSTOPERATIVE CARE PROTOCOLS
The successful management of acetabular fractures extends far beyond the operating theater. Achieving an anatomical reduction and stable internal fixation is only the first step; meticulous postoperative care is paramount to optimizing functional outcomes and mitigating the high risk of perioperative complications. The postoperative protocol must be tailored to the specific fracture pattern, the surgical approach utilized, the quality of bone stock, and the presence of concomitant polytrauma.
Immediate Postoperative Phase (Days 0–3)
In the immediate postoperative period, physiological stabilization and the prevention of early complications are the primary objectives.
- Wound Management: Closed suction drainage is routinely employed to prevent the formation of deep pelvic hematomas, which can serve as a nidus for infection or contribute to sciatic nerve compression. Drains are typically discontinued when output falls below 30 to 50 mL over a 24-hour period.
- Antibiotic Prophylaxis: Intravenous antibiotic therapy (typically a first-generation cephalosporin, or vancomycin in patients with penicillin allergies or high MRSA risk) is continued for 24 hours postoperatively. Prolonged prophylactic antibiotics beyond 24 hours have not been shown to decrease infection rates and may select for resistant organisms.
- Early Mobilization: Passive motion of the hip is initiated on the second or third postoperative day. Continuous passive motion (CPM) machines may be utilized to prevent intra-articular adhesions and promote cartilage nutrition through synovial fluid diffusion.
Clinical Pearl: Early passive range of motion (ROM) is critical for cartilage health. The cyclical loading and unloading of the joint surface facilitate the diffusion of nutrients into the avascular articular cartilage, which is especially vital following the mechanical insult of a fracture and subsequent surgical reduction.
Weight-Bearing and Rehabilitation Biomechanics
The biomechanics of the hip joint dictate a highly conservative approach to postoperative weight-bearing. The hip joint experiences forces up to three to four times body weight during normal ambulation due to the lever arm mechanics of the abductor musculature.
- Touch-Down Weight-Bearing (TDWB): Patients are restricted to touch-down (or toe-touch) ambulation with the assistance of crutches or a walker. This is progressed strictly as tolerated and is heavily dependent on the presence of other injuries in the polytraumatized patient.
- Duration of Restriction: This minimal weight-bearing status is rigorously maintained for approximately 8 weeks in patients with simple fracture patterns (e.g., isolated posterior wall or anterior column fractures) and extended to 12 weeks for most complex, multi-fragmentary, or both-column fractures.
- Abductor Rehabilitation: Rehabilitation of the abductor muscle group (gluteus medius and minimus) is absolutely essential, particularly after the Kocher-Langenbeck and other extensile exposures. These approaches require significant retraction or partial detachment of the abductors, leading to postoperative weakness and a potential Trendelenburg gait if not aggressively rehabilitated.
SURGICAL APPROACHES AND RADIOGRAPHIC EVALUATION
The choice of surgical approach directly influences both the reduction strategy and the postoperative complication profile. Modern acetabular surgery relies heavily on specific intervals to access complex intra-pelvic anatomy.
Anterior Column and Quadrilateral Surface Management
Fractures involving the anterior column and the quadrilateral surface often require an anterior approach. The ilioinguinal approach, frequently combined with the Stoppa interval (anterior intrapelvic approach), allows for direct visualization and stabilization of the quadrilateral plate, preventing medial subluxation of the femoral head.
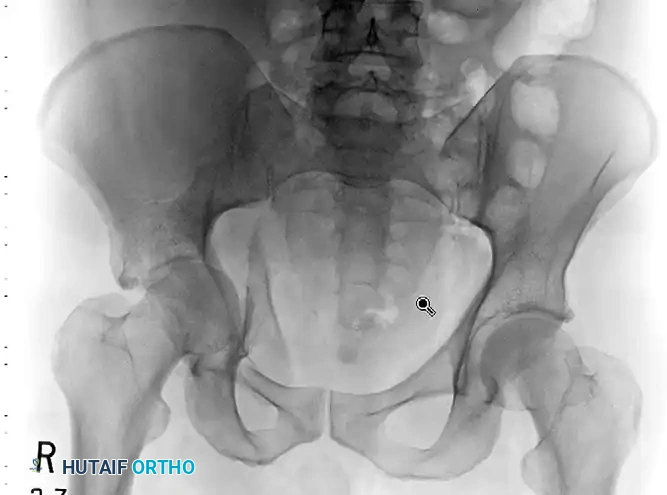


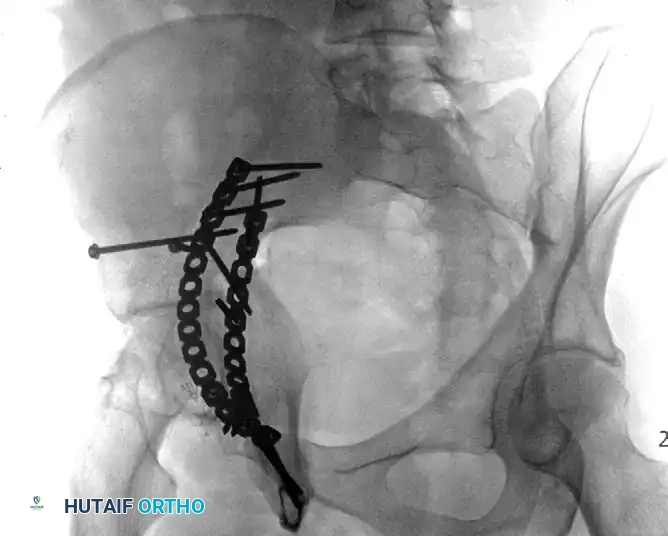
FIGURE 56-33: Anterior column fracture with quadrilateral surface comminution treated through an ilioinguinal approach with the Stoppa interval utilized to stabilize the quadrilateral surface.
Both-Column Fractures and Indirect Reduction
Both-column fractures represent complete dissociation of the articular surface from the axial skeleton. These complex injuries often require extensive exposures or combined approaches. However, when treated through an ilioinguinal approach, indirect reduction techniques are frequently employed to restore the acetabular dome, with fixation placed on the internal surfaces of the pelvis to buttress the columns.
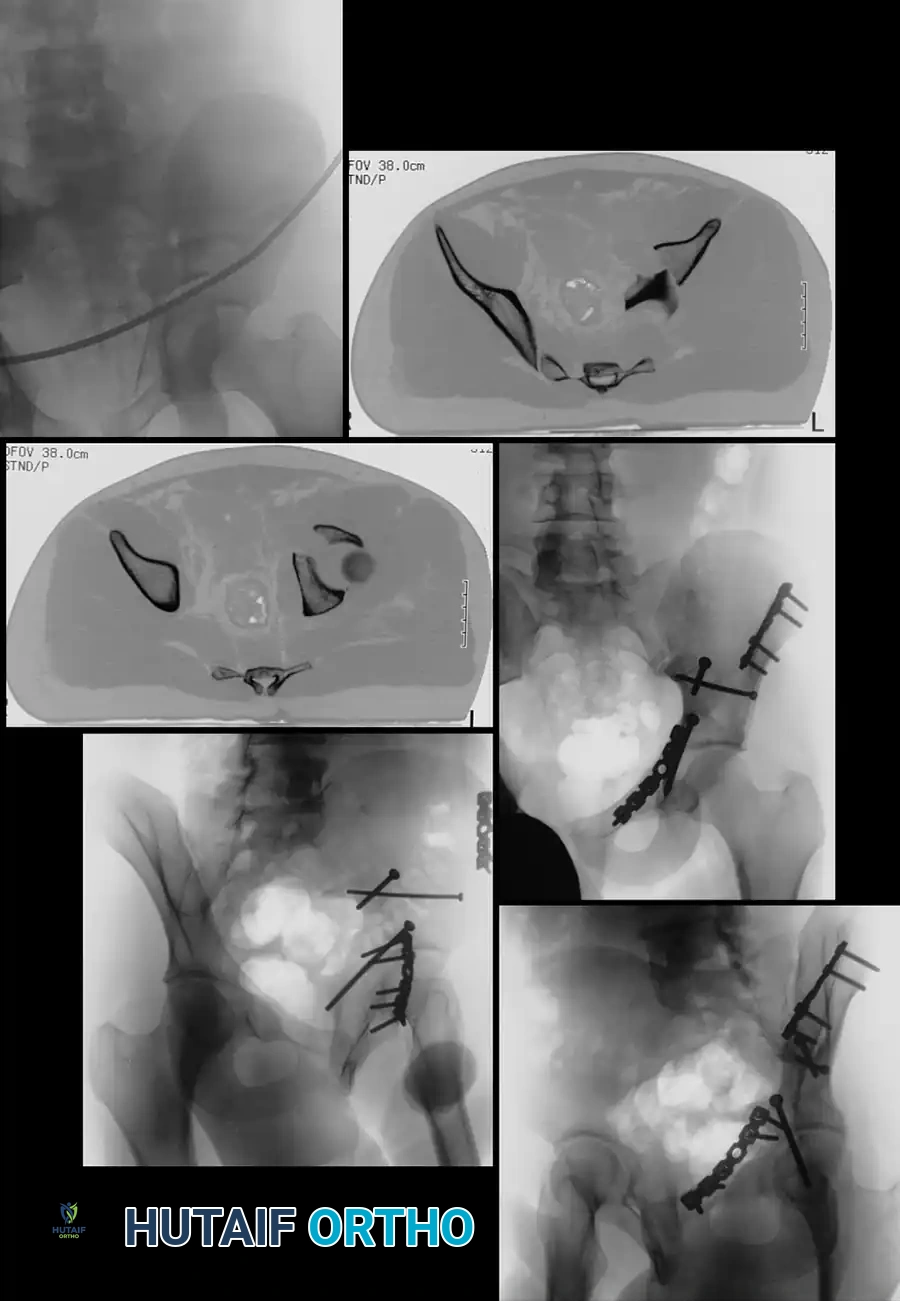
FIGURE 56-34: Both-column acetabular fracture treated through an ilioinguinal approach with indirect reduction of the acetabulum and fixation placed on the internal surfaces of the pelvis.
The Critical Role of Postoperative Computed Tomography (CT)
Historically, reduction quality was assessed using the three standard Judet radiographic views (AP pelvis, obturator oblique, and iliac oblique). However, plain radiographs lack the sensitivity required to detect small, clinically significant incongruencies.
- Radiographic Deception: Moed et al. demonstrated that while anatomical reductions were seemingly obtained in 97% of posterior wall fractures based on plain radiographs, 16% of these cases had an intra-articular incongruity or gap of 2 mm or more when evaluated by postoperative CT.
- Standard of Care: CT is vastly superior in identifying postoperative gaps, step-offs, and retained intra-articular hardware. Consequently, postoperative CT is now strongly recommended as the gold standard for the definitive assessment of operative reduction in acetabular trauma.
CLINICAL OUTCOMES AND SURVIVORSHIP
The ultimate goal of acetabular fracture surgery is the preservation of the native hip joint and the avoidance of total hip arthroplasty (THA).
Mortality Rates
Acetabular fractures are high-energy injuries often associated with significant polytrauma.
* Reported overall mortality rates range from 0% to 2.5%.
* In Letournel’s foundational series, mortality in patients older than 60 years was notably higher at 5.7%, reflecting the decreased physiological reserve in the geriatric population.
* Modern data from the National Trauma Data Bank (involving 8,736 patients) indicates an overall in-hospital mortality of 1.5%, while comprehensive meta-analyses suggest a rate closer to 3%.
Posttraumatic Arthritis (PTA)
Posttraumatic osteoarthritis is the most common long-term complication, directly correlating with the quality of the articular reduction and the initial energy of the injury.
Letournel’s landmark series of 940 patients remains the benchmark. Of the 569 patients who underwent open reduction and internal fixation (ORIF) within 21 days of injury, 17% developed posttraumatic arthritis at a minimum 1-year follow-up.
* Impact of Reduction Quality: Following a perfect anatomical reduction (418 fractures), the rate of PTA was 10.2%. Conversely, after an imperfect reduction (151 fractures), the PTA rate skyrocketed to 35.7%.
* Fracture Pattern Influence: Both-column and transverse posterior wall fractures historically yield worse results, primarily due to the sheer difficulty of obtaining a perfect reduction. Interestingly, even when posterior wall fractures were reduced nearly perfectly (98% of the time), they still resulted in PTA in 17% of cases, likely due to the initial impaction injury to the articular cartilage (chondrocyte apoptosis) at the time of dislocation.
* Modern Meta-Analyses: Recent literature involving 1,211 patients found an overall osteoarthritis incidence of 27%. This was stratified into a 13% incidence with satisfactory reduction (≤ 2 mm step-off) and a 43% incidence with unsatisfactory reduction.
* Longitudinal Trends: A 16-year prospective epidemiologic study (351 patients) reported a decline in the rate of osteoarthritis from 31% to 14% over the study span, reflecting advancements in surgical techniques, imaging, and instrumentation.
Surgical Warning: Cartilage damage occurs at the moment of impact. Even with a radiographically "perfect" reduction, the initial mechanical trauma causes irreversible chondrocyte death. Surgeons must counsel patients preoperatively that ORIF minimizes, but does not eliminate, the risk of future posttraumatic arthritis.
COMPLICATIONS AND MANAGEMENT STRATEGIES
Osteonecrosis (Avascular Necrosis)
Osteonecrosis of the femoral head or the acetabular fracture fragments is a devastating complication that frequently necessitates conversion to THA. It is radiographically apparent within 2 years of injury in the vast majority of affected patients.
- Incidence: A modern meta-analysis of 2,010 patients reported an overall osteonecrosis incidence of 5.6%.
- The Role of Dislocation: The risk is heavily stratified by the presence of an initial posterior hip dislocation. The incidence rises to 9% in patients with a posterior dislocation, compared to 5% in those without. Letournel reported a 7.5% rate after posterior dislocation versus 1.6% for other fractures.
- Iatrogenic Causes: Osteonecrosis of the posterior wall fragments can be exacerbated by excessive surgical exposure. The primary vascular supply to these osteochondral fragments is the injured posterior capsule of the hip. Aggressive stripping of the capsule during a Kocher-Langenbeck approach devascularizes these fragments, leading to structural collapse.
Surgical Site Infection
Deep surgical site infections occur in 1% to 5% of patients and can rapidly destroy the articular cartilage, leading to catastrophic joint failure.
- Approach-Specific Risks: The presence of a suprapubic catheter significantly increases infection risk when utilizing the ilioinguinal approach.
- Morel-Lavallée Lesions: Closed internal degloving injuries (Morel-Lavallée lesions) over the greater trochanter are highly associated with infection when utilizing Kocher-Langenbeck or extensile approaches. These lesions must be meticulously debrided and managed prior to or during definitive fixation.
- Obesity: Elevated Body Mass Index (BMI) is a profound risk factor. Studies demonstrate that patients with a BMI > 40 have a five-fold increased risk of infection and a significantly higher rate of overall wound healing complications (46% vs. 12% for BMI < 40).
Sciatic Nerve Palsy
The sciatic nerve is intimately related to the posterior column of the acetabulum and is at high risk during both the initial trauma and surgical intervention.
- Traumatic vs. Iatrogenic: Sciatic nerve palsies resulting from the initial injury occur in 10% to 15% of patients. Iatrogenic (surgically induced) injury occurs in 2% to 6% of patients, most frequently associated with posterior fracture patterns treated via the Kocher-Langenbeck or extensile exposures due to prolonged retractor placement.
- Anatomical Vulnerability: The peroneal division of the sciatic nerve is tethered at the fibular head and has less connective tissue supporting its fascicles compared to the tibial division. Consequently, the peroneal component is more frequently injured and has a significantly worse prognosis for recovery. Complete peroneal palsies carry the poorest functional outlook, whereas the tibial component has a greater propensity for recovery.
- Neuromonitoring Controversy: The use of intraoperative somatosensory evoked potentials (SSEPs) and spontaneous electromyography (sEMG) to monitor the sciatic nerve is highly debated. While some advocate its use to prevent iatrogenic stretch injuries, experienced pelvic surgeons report similar iatrogenic injury rates without monitoring. A poll of Orthopaedic Trauma Association (OTA) members revealed that only 15% routinely utilize nerve monitoring during acetabular surgery.
- Prognosis: Functional recovery is observed in approximately 65% of patients, with neurological improvement continuing for up to 3 years post-injury.
Heterotopic Ossification (HO)
Heterotopic ossification—the formation of mature lamellar bone in non-osseous soft tissues—is a frequent complication following surgical trauma to the hip abductors.
- Incidence by Approach: HO occurs most frequently after extensile approaches (e.g., extended iliofemoral), with moderate-to-severe HO (Brooker grades III and IV) occurring in 14% to 50% of patients without prophylaxis. Following the Kocher-Langenbeck approach, the rate is approximately 25%. It is exceedingly rare after the ilioinguinal approach unless the external surface of the ilium is aggressively stripped.
- Prophylactic Regimens:
- Indomethacin: A non-steroidal anti-inflammatory drug (NSAID) that inhibits prostaglandin synthesis. The standard protocol is 25 mg orally three times daily for 4 to 6 weeks. While generally effective, some prospective series have questioned its absolute efficacy, and it carries risks of gastrointestinal bleeding and potential fracture nonunion.
- Radiation Therapy (XRT): A single low-dose fraction of 700 cGy administered within 72 hours postoperatively is highly effective at preventing the differentiation of mesenchymal stem cells into osteoblasts. XRT is frequently utilized when indomethacin is contraindicated or in high-risk extensile exposures. Routine use in very young patients is generally avoided due to theoretical oncogenic risks.
- Surgical Technique: Meticulous debridement of devitalized gluteus minimus muscle tissue is strongly advocated to remove the necrotic nidus that stimulates osteoinduction.

FIGURE 56-35: Brooker grade IV heterotopic ossification occurred despite postoperative irradiation, demonstrating complete bony ankylosis of the hip joint.
Thromboembolic Complications
Pelvic trauma induces a profound hypercoagulable state (Virchow's triad: endothelial injury, venous stasis, and hypercoagulability). Thromboembolic events can be fatal.
- Incidence: The reported risk of pulmonary embolism (PE) ranges from 2% to 6%. Deep vein thrombosis (DVT) rates vary wildly from 8% to 61%, heavily dependent on the screening modality utilized.
- Screening Modalities:
- Duplex Ultrasound: Often underestimates the presence of significant clots because it cannot reliably detect intrapelvic vein thrombosis (e.g., internal iliac veins) compared to invasive venography.
- Magnetic Resonance Venography (MRV): Highly sensitive, detecting asymptomatic DVT in 34% of patients (49% of which are above the inguinal ligament). However, both MRV and contrast-enhanced CT have high false-positive rates. Positive findings on screening MRV/CT should ideally be correlated with selective venography before committing to aggressive interventions like inferior vena cava (IVC) filters.
- Prophylaxis Protocols:
- Preoperative: Subcutaneous low-molecular-weight heparin (LMWH, e.g., enoxaparin) or unfractionated heparin, combined with intermittent pneumatic compression boots, is initiated while the patient awaits surgery.
- Screening: A preoperative screening duplex Doppler scan is mandatory for any patient whose injury is more than 4 days old or who has not received adequate early prophylaxis.
- IVC Filters: Greenfield vena cava filters are indicated for patients with documented preoperative proximal DVTs, or in high-risk groups where anticoagulation is strictly contraindicated (e.g., severe traumatic brain injury). High-risk factors include age > 60 years, morbid obesity, active malignancy, or a prior history of VTE.
- Postoperative: Chemical anticoagulation with LMWH (enoxaparin) followed by a transition to oral agents (such as warfarin or direct oral anticoagulants) is continued for 6 to 12 weeks postoperatively, provided there are no medical contraindications.
