INTRODUCTION TO FOREFOOT KINEMATICS AND INTRINSIC IMBALANCE
The first ray of the foot is a complex biomechanical unit essential for normal gait, weight-bearing, and the windlass mechanism. Deformities of the hallux—ranging from fixed interphalangeal (IP) joint contractures to severe claw toe and hallux extensus—often stem from a profound disruption of the intrinsic muscle balance. The plantar plate, a robust fibrocartilaginous structure, serves as the primary static stabilizer of the metatarsophalangeal (MTP) and IP joints. When intrinsic muscle function is compromised (often iatrogenically via sesamoidectomy or aggressive capsulorrhaphy), the delicate equilibrium between the flexor and extensor mechanisms is lost.
This masterclass provides an exhaustive, evidence-based review of plantar plate release, the "hanging toe" procedure, and the management of complex forefoot deformities and complications, tailored for the practicing orthopedic consultant and advanced surgical fellow.
SURGICAL ANATOMY AND NEUROVASCULAR CONSIDERATIONS
A profound understanding of forefoot neuroanatomy is paramount to avoiding debilitating postoperative neuromas. The cutaneous innervation of the foot is highly variable, but specific zones are consistently at risk during first ray surgery.

As illustrated above, the cutaneous nerves of the foot include:
* Superficial Peroneal Nerve: Divides into a medial (intermediate) branch supplying the medial side of the hallux and the second/third dorsal web spaces, and a lateral branch to the third and fourth web spaces. The branch to the dorsomedial aspect of the hallux is the most vulnerable to injury during medial incisions.
* Deep Peroneal Nerve: Courses between the first and second metatarsals to innervate the skin of the first dorsal web space.
* Saphenous Nerve: Courses anterior to the medial malleolus, innervating the skin over the dorsomedial aspect of the hindfoot and midfoot.
* Sural Nerve: Passes posterior to the lateral malleolus, dividing near the calcaneocuboid joint to supply the lateral side of the fifth toe.
Surgical Warning: Neuroma and hematoma are largely avoidable with meticulous attention to anatomical detail. If a tourniquet is utilized, it must be released prior to closure to ensure absolute hemostasis. A postoperative neuroma in the foot can be a severely debilitating complication that eclipses the success of the primary osseous or soft-tissue correction.
PLANTAR PLATE RELEASE: SURGICAL TECHNIQUE
The plantar plate release is indicated for fixed flexion contractures of the IP joint or extension contractures of the MTP joint that do not passively correct.
Preoperative Preparation and Positioning
The patient is placed supine on the operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg to a neutral position, allowing direct visualization of the medial forefoot. A thigh or calf tourniquet is applied based on surgeon preference.
Step-by-Step Surgical Approach
- Incision and Dissection: Begin with a 3-cm medial incision centered at the midshaft of the proximal phalanx, extending distally to the level of the nail base. This specific placement is critical to avoid the sensory branches of the medial proper plantar digital nerve supplying the pulp of the hallux.
- Flexor Hallucis Longus (FHL) Exposure: Locate the sheath of the FHL. Incise it longitudinally for exactly 1 cm, centered directly over the interphalangeal joint.
- Capsular Release: Make a midline medial incision. Expose the metatarsal head by incising the capsule 2 to 3 mm plantar to the center of the skin incision. Elevate the capsule from the metatarsal head and the base of the proximal phalanx, working both dorsally and plantarward.
- Sesamoid Evaluation: Expose the tibial sesamoid. If the deformity is rigidly fixed in extension at the MTP joint, a wider resection of the soft tissue extending to the junction of the neck and shaft of the first metatarsal is mandated.
- Dynamic Assessment: Manually reduce the hallux into a valgus position. Release the capsule incrementally to evaluate tightness. Note: If all components of the deformity are not completely correctable passively at this stage, soft tissue correction alone will fail, and osseous intervention is required.
- Articular Surface Inspection: Examine the articular cartilage of the first metatarsal head. If there is significant eburnation, loss of cartilage, or unhealthy-appearing surfaces (presumably from chronic abnormal pressure), proceed directly to an MTP arthrodesis.
- Joint Fixation (If Cartilage is Viable): If the articular cartilage is reasonably normal and passive motion is unimpeded, fix the hallux in 10 degrees of valgus. Utilize a 0.062-inch Kirschner wire (K-wire), driving it obliquely across the joint from the medial base of the proximal phalanx to the lateral head-neck junction of the first metatarsal. Ensure the sesamoids are anatomically positioned beneath the metatarsal head.
Interphalangeal Joint Contracture Release
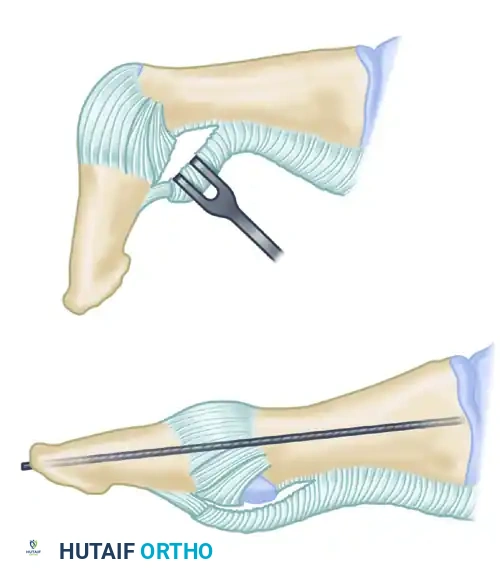
To address the IP joint contracture:
1. Utilize a dorsal inverted-L incision. The transverse limb crosses the dorsum of the IP joint, while the proximal limb extends 2 to 3 cm proximally along the dorsolateral border of the proximal phalanx.
2. Using a small-bladed scalpel (e.g., #15 blade), carefully remove 2 to 3 mm of the FHL tendon insertion onto the base of the distal phalanx. Because this insertion is broad and tenacious, this fractional release will not disrupt the overall tendon attachment.
3. Gently flex and extend the joint to identify the plantar plate insertion on the neck of the proximal phalanx. Completely incise the plantar plate from the neck, allowing it to slide distally and expose the IP joint.
4. If passive correction to neutral is still not achieved, release the accessory portions of the collateral ligaments that insert into the plantar plate.
5. Postoperative Fixation: Hold the IP joint in a neutral position with one or two 0.062-inch K-wires for 4 to 6 weeks. Leave the wires protruding 2 to 3 mm from the skin, capped or covered with a plastic strip to prevent pin-tract infections.
THE "HANGING TOE" PROCEDURE
The "hanging toe" procedure is a salvage technique involving the resection of all intrinsic muscle attachments to the base of the proximal phalanx, typically performed when the proximal third of the phalanx is excised (resection arthroplasty).
Technical Execution
- Pin Fixation: The procedure mandates the insertion of two longitudinal, parallel K-wires to maintain the hallux in 5 to 10 degrees of valgus for 6 weeks.
- Extensor Hallucis Longus (EHL) Tensioning: Before driving the K-wires retrograde through the phalanges and antegrade into the metatarsal head, the tension on the EHL tendon must be critically evaluated. Hold the foot and ankle in neutral dorsiflexion. If the EHL is causing an extensor posture of the hallux, it must be lengthened (Z-plasty) by no more than 1 cm prior to fixation.
- Managing Dorsal Calluses: If a fixed flexion contracture of the IP joint has resulted in symptomatic dorsal calluses, two options exist:
- Arthrodesis of the IP joint concurrent with the MTP resection arthroplasty.
- Plantar plate release at the IP joint with neutral pin fixation.
CLAW TOE AND INTRINSIC IMBALANCED HALLUX
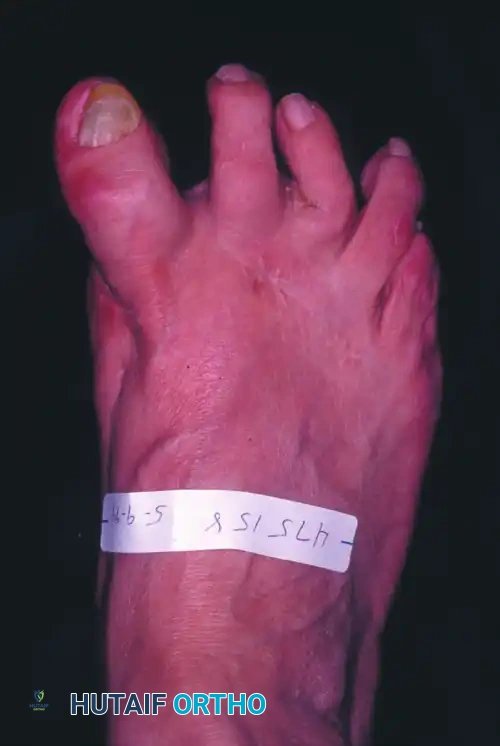
Claw toe of the hallux is a complex multi-joint deformity characterized by hyperextension of the MTP joint and flexion of the IP joint, with or without fixed contractures.
Pathomechanics
Hallux extensus frequently accompanies this deformity. The patient is unable to place the pulp of the great toe on the floor during the stance phase of gait.
Clinical Pearl: The crucial biomechanical loss in a clawed hallux is the intrinsic muscle flexion moment at the MTP joint. This intrinsic-minus state allows the unopposed EHL and Extensor Hallucis Brevis (EHB) to hyperextend the MTP joint. Consequently, the EHL loses its excursion (slackness) and fails to extend the IP joint, leading to a secondary flexion deformity.
This loss of intrinsic control is most frequently iatrogenic—typically secondary to bilateral sesamoidectomy, or a fibular sesamoidectomy combined with aggressive medial capsular imbrication leading to dorsomedial subluxation of the tibial sesamoid.
Surgical Management of Claw Toe
To preserve MTP joint motion while correcting the deformity, a triad of procedures is the treatment of choice:
1. Arthrodesis of the IP Joint: Simple arthrodesis alone will not correct the MTP hyperextension.
2. EHL Transfer: Transfer the EHL tendon into the neck of the first metatarsal (Jones transfer) to elevate the metatarsal head and remove the deforming extensor force.
3. Dorsal Capsulotomy: Perform a dorsal capsulotomy of the MTP joint. This effectively lengthens the EHB tendon as it heals with scar tissue in continuity.
A K-wire must be inserted to hold the MTP joint in neutral for 4 weeks. If preoperative radiographs reveal degenerative articular changes at the MTP joint, joint-sparing procedures are contraindicated, and a primary first MTP arthrodesis should be performed.
LIMITATION OF MTP JOINT MOTION AND HALLUX EXTENSUS
Capsulorrhaphy Biomechanics
An essential component of any soft-tissue hallux valgus correction is the imbrication ("reefing") of the medial capsule. Whether performed coronally or sagittally, the outcome is soft-tissue plication around a mobile joint. To maintain valgus correction, the capsulorrhaphy must be snug, which inherently decreases MTP joint motion.
Patient Counseling: Prior to any bunion surgery, patients must be explicitly informed that some loss of MTP motion is expected. However, this limitation is seldom clinically significant and should not decrease overall function. Postoperative wrapping of the hallux in neutral or 5 degrees of flexion is highly beneficial.
Isolated Hallux Extensus
Hallux extensus occurring as an isolated deformity (without hallux varus or clawing) is exceedingly rare. The primary etiology is iatrogenic laceration of the FHL tendon during sesamoidectomy or a Keller resection arthroplasty. Surgeons must meticulously verify FHL integrity via direct inspection and passive excursion testing after any sesamoid excision.
COMPLICATIONS IN FOREFOOT SURGERY
Stress Fractures of the Lesser Metatarsals
Stress fractures of the second, third, or rarely fourth metatarsals occur most frequently in postmenopausal women following first ray surgery. Attempting to unload the first ray (due to pain, shortening, or elevation) transfers pathological forces to the lesser metatarsals.
Treatment involves protected weight-bearing in a rigid wooden-soled shoe or controlled ankle motion (CAM) boot for 3 to 4 weeks.
Pitfall: If a stress fracture of the second or third metatarsal heals with apex-plantar angulation, the metatarsal head is driven plantarward, producing intractable, painful calluses. Prophylactic protection in osteoporotic patients is mandatory even before radiographic evidence of callus formation appears.
Complications of Resection Arthroplasty (Keller Procedure)
While largely replaced by modern osteotomies and arthrodesis, the Keller procedure retains utility in low-demand, elderly patients with severe rheumatoid destruction or osteoarthritis. However, complications are frequent:
- Cock-Up Hallux: Excision of the base of the proximal phalanx detaches the intrinsic flexors. Without intrinsic flexion, an extension contracture develops at the MTP joint, with concomitant IP flexion. A painful dorsal IP callus ensues, best treated by IP arthrodesis. If the cock-up deformity is severe and >33% of the proximal phalanx was excised, an interposition corticocancellous bone graft may be required to restore length and stability, though nonunion rates are high.
- Metatarsalgia: The Keller procedure drastically unloads the medial column due to extreme varus of the first metatarsal and loss of the windlass mechanism. This results in transfer metatarsalgia and painful callosities beneath the lesser metatarsal heads. Realigning the first ray closer to the second metatarsal reduces this load. Patients must be warned preoperatively that existing lesser metatarsalgia may worsen post-Keller.
Complications After Arthrodesis of the First MTP Joint
First MTP arthrodesis is the gold standard for severe hallux rigidus and salvage of failed forefoot procedures. The primary complications are nonunion (occurring in <10% of cases, often asymptomatic), malunion, and adjacent joint (IP) arthritis.
The Critical Importance of Positioning:
Accurate intraoperative positioning is the single most important factor in a successful MTP arthrodesis. The hallux must be positioned to accommodate shoe wear and normal gait roll-off.
* Dorsiflexion: 15 degrees relative to the plantar surface of the foot (the floor), which equates to 25 to 30 degrees of dorsiflexion relative to the anatomical inclination angle of the first metatarsal.
* Valgus: 15 degrees of valgus is strictly recommended. This aligns the hallux with the lesser toes, prevents impingement against the second toe, and significantly reduces the risk of degenerative changes in the IP joint and subsequent callus formation.
* Rotation: Neutral rotation; the plane of the hallux nail must perfectly match the plane of the lesser toes.
In the context of a rheumatoid forefoot reconstruction, the lesser MTP joints must be fully reconstructed and stabilized before the final positioning and fixation of the hallux arthrodesis.
