PEDIATRIC PELVIC FRACTURES: PATHOLOGY AND BIOMECHANICS
Fractures of the pelvis in children are relatively unusual, representing a distinct clinical entity compared to adult pelvic trauma. Because of the immense remodeling potential of the immature skeleton, open reduction and internal fixation (ORIF) are rarely necessary. Generally, the long-term functional and radiographic results of conservative treatment are highly satisfactory. However, the mechanism of injury—typically high-energy trauma such as a child being struck by a moving vehicle—dictates that soft-tissue and multisystem injuries occurring in conjunction with pelvic fractures are often severe and require immediate, life-saving emergency treatment.
The Pediatric vs. Adult Pelvis: Biomechanical Differences
The pediatric pelvis possesses unique biomechanical and anatomical characteristics that directly influence fracture patterns and management algorithms. These differences include:
- Osseous Malleability: The pediatric pelvic bone is highly malleable due to its lower mineral content and higher porosity. The cartilaginous structures possess a profound ability to absorb energy before failing.
- Joint Elasticity: The symphysis pubis and sacroiliac (SI) joints exhibit significantly greater elasticity. This allows for substantial displacement and deformation, frequently resulting in a fracture in only one area of the ring, contrasting with the traditional "double break" (e.g., Malgaigne fracture) obligatory in rigid adult pelves.
- Apophyseal Vulnerability: The cartilage at the apophyses is inherently weaker than the adjacent bone or the attaching musculotendinous units. Consequently, avulsion fractures occur with much higher frequency in children and adolescents than in adults.
- Triradiate Cartilage: Fractures extending into the triradiate cartilage can cause premature closure and growth arrest. This complication inevitably results in leg-length inequality and secondary acetabular dysplasia.
Clinical Pearl: In children and adolescents, isolated pubic rami and iliac wing fractures occur predominantly in immature hips (open triradiate cartilage). Conversely, acetabular fractures and pubic or sacroiliac diastasis occur more frequently in mature hips (closed triradiate cartilage).
CLINICAL EVALUATION AND ASSOCIATED INJURIES
Because pediatric pelvic fractures are markers of massive energy transfer, the initial evaluation must strictly adhere to Advanced Trauma Life Support (ATLS) protocols. Mortality in children with pelvic fractures is high (ranging from 9% to 18%), but as noted by Demetriades et al. and Silber and Flynn, the death rate from the pelvic fracture alone is exceptionally low (0% to 2.3%). Mortality is almost exclusively driven by associated injuries.
Multisystem Trauma Correlation
Associated injuries frequently include skull, cervical, facial, and long bone fractures; subdural hematomas and cerebral contusions; lung contusions, hemothorax, and ruptured diaphragms; and lacerations of the spleen, liver, and kidneys.
Bond et al. established a critical correlation between the location/number of pelvic fractures and the probability of intra-abdominal injury:
* 1% probability for isolated pubic fractures.
* 15% probability for iliac or sacral fractures.
* 60% probability for multiple fractures of the pelvic ring.
Local adjacent injuries include damage to major blood vessels, retroperitoneal hemorrhage, rectal tears, and rupture of the urethra or bladder.
Pathognomonic Physical Signs
During the secondary survey, three classic physical signs indicate significant pelvic trauma:
* Destot Sign: A large superficial hematoma forming beneath the inguinal ligament or within the scrotum/labia.
* Roux Sign: A measurable decrease in the distance from the greater trochanter to the pubic spine on the affected side, indicative of a lateral compression fracture.
* Earle Sign: A palpable bony prominence, large hematoma, or severe tenderness on digital rectal examination.
Provocative maneuvers, such as posterior pressure on the iliac crests (opening the ring) or lateral-to-medial compression, will elicit pain and crepitation in unstable injuries.
CLASSIFICATION SYSTEMS
Numerous classification systems exist, but the most clinically relevant for pediatric patients focus on stability and the integrity of the pelvic ring.
Torode and Zieg Classification
Torode and Zieg proposed a highly utilized four-part classification system for pediatric pelvic fractures:
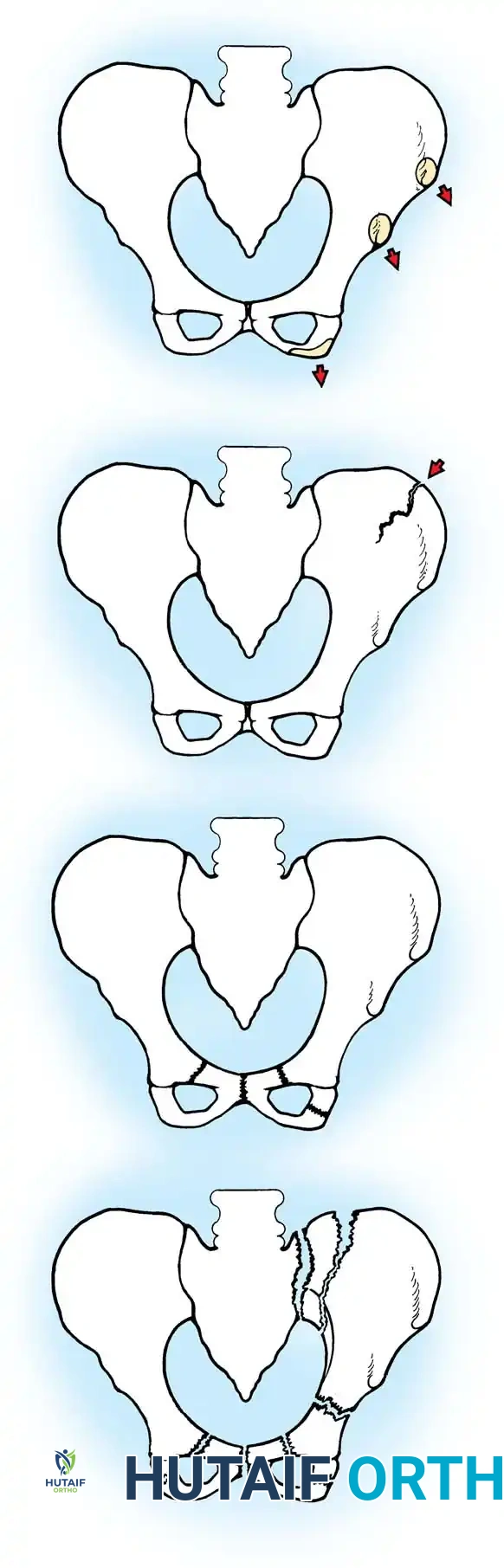
- Type I: Avulsion fractures of the bony elements of the pelvis (e.g., ASIS, AIIS, ischial tuberosity).
- Type II: Iliac wing fractures.
- Type III: Simple ring fractures, including isolated fractures involving the pubic rami or disruptions of the pubic symphysis without posterior instability.
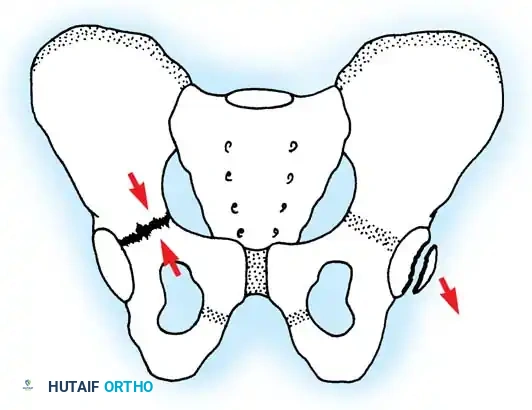
- Type IV: Ring disruption fractures creating an unstable segment. This includes bilateral pubic rami (straddle) fractures, fractures involving the anterior ring with a concomitant fracture through the posterior elements or SI joint, and fractures involving the acetabulum.
Surgical Warning: Torode and Zieg reported that 40% of patients with Type IV injuries required an emergent laparotomy due to severe associated visceral injuries.
Single vs. Double Breaks
Due to the elasticity of the pediatric pelvis, a single break in the ring is common and often stable.
Single break in the pelvic ring, demonstrating two ipsilateral rami fractures without posterior disruption.
SPECIFIC FRACTURE PATTERNS AND MANAGEMENT
Avulsion Fractures
Avulsion fractures occur most commonly in adolescent athletes due to sudden, violent muscle contraction against a fixed resistance.
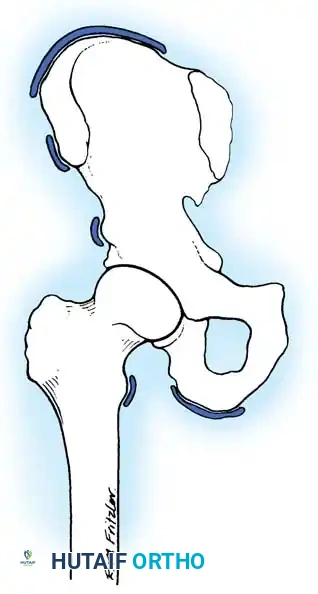
Common sites include:
* Anterior Superior Iliac Spine (ASIS): Sartorius muscle avulsion.
* Anterior Inferior Iliac Spine (AIIS): Rectus femoris muscle avulsion.
* Ischial Tuberosity: Hamstring muscle avulsion.
* Iliac Crest: Abdominal musculature avulsion.
Management: Operative treatment is rarely indicated. Conservative management consisting of rest, protected weight-bearing with crutches for 3 to 4 weeks, and a gradual return to sports yields excellent results regardless of displacement.
Complications: Displaced ischial tuberosity fractures may occasionally result in excessive callus formation or myositis ossificans, which can mimic Ewing sarcoma or osteomyelitis. If symptomatic nonunion or massive callus restricts athletic activity, delayed surgical excision of the fragment (rather than reattachment) is the preferred intervention.
Acetabular and Triradiate Cartilage Injuries
Fractures involving the acetabulum and the triradiate cartilage require meticulous evaluation, often necessitating fine-cut Computed Tomography (CT) scans to assess joint congruity and physeal involvement.
Small acetabular rim fracture (right) and triradiate cartilage compression fracture (left).
Management:
* Undisplaced/Stable: Managed with non-weight-bearing and close radiographic follow-up.
* Displaced (>2mm step-off): Requires ORIF to restore joint congruity and minimize the risk of post-traumatic arthritis.
* Triradiate Cartilage: Compression injuries (Salter-Harris V equivalents) are notorious for causing premature physeal closure. Parents must be counseled regarding the high risk of secondary acetabular dysplasia and leg-length discrepancy, requiring long-term follow-up until skeletal maturity.
Spinal-Pelvic Junction Injuries
High-energy trauma can also result in complex injuries at the lumbosacral junction. Because of the elasticity of a child’s spine, forces are transmitted over many segments.
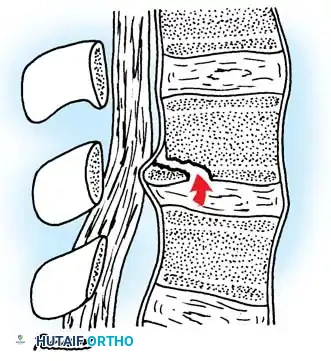
Posterior physeal injury that can mimic a ruptured disc. Avulsion of the ring apophysis produces a displaced fragment that compresses the nerve root.
In cases of burst fractures or fracture-dislocations with neurological deficits, operative decompression and stabilization are mandatory. Furthermore, pediatric Chance fractures (flexion-distraction injuries) caused by lap seat belts are highly associated with intra-abdominal hollow viscus injuries, especially when a "seat belt sign" (abdominal ecchymosis) is present.
OPERATIVE MANAGEMENT: INDICATIONS AND TECHNIQUES
While most pediatric pelvic fractures are treated conservatively with bed rest and supportive care, specific indications necessitate surgical intervention. Surgery is generally reserved for patients with a mature pelvis, severe hemodynamic instability, or unacceptable displacement.
Indications for Surgery
- Hemodynamic Instability: Severe diastasis of the pubic symphysis or open-book pelvic fractures causing life-threatening retroperitoneal hemorrhage.
- Unstable Pelvic Ring (Type IV): Vertical shear injuries or highly displaced Malgaigne fractures.
- Acetabular Incongruity: Intra-articular displacement >2mm.
- Open Pelvic Fractures: Requiring immediate debridement and stabilization.
Operative Technique: Application of Pelvic External Fixator
External fixation is the workhorse for acute, hemodynamically unstable "open-book" (anteroposterior compression) fractures in children. It rapidly reduces pelvic volume, promoting tamponade of retroperitoneal venous bleeding.

Radiographic sequence demonstrating the application of a pelvic external fixator to close a severe diastasis of the symphysis pubis.
Step-by-Step Procedure:
1. Positioning: Supine on a radiolucent trauma table. Ensure the abdomen and pelvis are prepped widely to allow for concurrent laparotomy if required by general surgery.
2. Incision and Approach: Make a 1-2 cm incision over the anterior inferior iliac spine (AIIS) or the iliac crest, depending on the chosen pin trajectory. The supra-acetabular (AIIS) corridor is biomechanically superior and preferred in older children.
3. Pin Insertion (Supra-acetabular):
* Bluntly dissect down to the bone between the sartorius and rectus femoris.
* Under fluoroscopic guidance (Obturator Outlet and Iliac Inlet views), place a drill guide.
* Insert 4.5 mm or 5.0 mm Schanz pins (depending on patient size) directed from the AIIS toward the posterior superior iliac spine (PSIS), staying strictly within the dense bone corridor above the sciatic notch.
4. Frame Assembly: Connect the pins with a carbon fiber rod system.
5. Reduction: Apply internal rotation compression forces to the pins to close the symphyseal diastasis. Confirm reduction fluoroscopically.
6. Final Tightening: Lock the frame. Ensure the abdomen is not compressed by the bar to avoid abdominal compartment syndrome.
Operative Technique: Open Reduction and Internal Fixation (ORIF)
In older adolescents with closed triradiate cartilages and unstable Type IV ring disruptions, ORIF is indicated to prevent long-term deformity, sitting imbalance, and chronic pain.
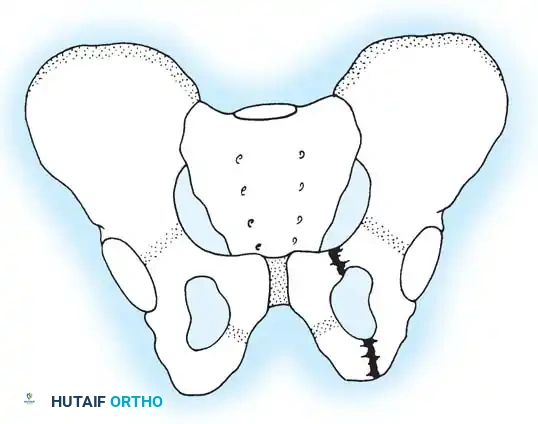
Anterior Ring Stabilization (Symphysis Pubis Plating):
1. Approach: A Pfannenstiel incision is utilized. The rectus abdominis is split linearly along the linea alba, exposing the retropubic space (Space of Retzius).
2. Reduction: A pelvic reduction forceps (Weber clamp) is placed on the superior pubic rami to anatomically reduce the symphysis.
3. Fixation: A multi-hole symphyseal plate (often a 3.5mm reconstruction plate) is contoured and secured with bicortical screws. In children, care must be taken not to strip the periosteum excessively to preserve the osteogenic potential.
Posterior Ring Stabilization (Percutaneous SI Screws):
1. Positioning: Supine or prone, depending on concurrent injuries.
2. Imaging: Perfect true lateral, inlet, and outlet fluoroscopic views of the sacrum are mandatory.
3. Guidewire Placement: A guidewire is advanced from the lateral ilium, across the SI joint, and into the center of the S1 vertebral body. In pediatric patients, the sacral ala can be dysmorphic; extreme caution is required to avoid the L5 nerve root anteriorly and the sacral foramina inferiorly.
4. Screw Insertion: A cannulated, partially threaded 6.5mm or 7.3mm screw is inserted over the wire to provide compression across the SI joint.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of pediatric pelvic fractures is dictated by the stability of the fixation and the presence of concomitant injuries.
- Weight-Bearing: For stable, conservatively managed fractures (Types I-III), patients are typically kept on bed rest for 1 to 3 weeks until acute pain subsides, followed by toe-touch weight-bearing with crutches. Full weight-bearing is usually achieved by 6 weeks.
- Operatively Managed Fractures: Patients with external fixators or ORIF are restricted to non-weight-bearing or toe-touch weight-bearing on the affected side for 6 to 8 weeks.
- External Fixator Care: Pin site care is performed daily using chlorhexidine or saline to prevent superficial infections. The fixator is typically removed in the clinic or under light sedation at 6 weeks once clinical and radiographic union is evident.
- Long-Term Monitoring: Any child who sustains a fracture involving the triradiate cartilage must be followed clinically and radiographically every 6 months until skeletal maturity. If premature closure occurs leading to acetabular dysplasia, reconstructive pelvic osteotomies (e.g., Salter, Pemberton, or Triple osteotomy) may be required in the future.
CONCLUSION
Pediatric pelvic fractures remain a formidable challenge, primarily due to the severity of associated multisystem trauma. While the inherent elasticity and remodeling capacity of the pediatric pelvis allow the vast majority of these injuries to be managed non-operatively, the orthopedic surgeon must remain vigilant. Accurate classification, recognition of triradiate cartilage involvement, and aggressive surgical stabilization of hemodynamically unstable or severely displaced mature pelvic fractures are critical to ensuring optimal long-term functional outcomes and preventing lifelong disability.
