INTRODUCTION TO LOWER EXTREMITY MALUNIONS
The management of malunited fractures of the lower extremity demands a profound understanding of biomechanics, joint kinematics, and advanced osteosynthesis techniques. Malunions disrupt the mechanical axis, alter load distribution across articular cartilage, and inevitably lead to early-onset osteoarthritis if left uncorrected. This comprehensive guide delineates the surgical strategies for addressing malunions of the patella, femoral condyles, and femoral shaft, providing orthopedic surgeons with evidence-based protocols for restoring anatomical alignment and functional integrity.
MALUNION OF THE PATELLA
Pathoanatomy and Clinical Presentation
The patella serves as a critical fulcrum for the extensor mechanism of the knee. A malunited fracture of the patella severely compromises this mechanical advantage. The clinical presentation of a patellar malunion is virtually indistinguishable from advanced chondromalacia patellae. Patients typically present with anterior knee pain, crepitus, recurrent effusions, and a subjective feeling of instability or "giving way" during activities that load the patellofemoral joint, such as descending stairs.
The degree of clinical disability is directly proportionate to two factors:
1. The severity of the step-off or irregularity on the articular surface of the patella.
2. The subsequent roughening and degradation of the contiguous articular cartilage of the femoral trochlea.
Surgical Rationale: Patellectomy
While acute patellar fractures are managed with open reduction and internal fixation (ORIF) to restore the articular surface, a malunion presents a different biological environment. The articular cartilage has often undergone irreversible damage due to abnormal contact pressures.
Clinical Pearl: Attempting an intra-articular osteotomy to correct a chronic patellar malunion is fraught with high failure rates due to pre-existing cartilage necrosis. Therefore, for even a relatively recent malunion with significant articular incongruity, a total or partial patellectomy remains the procedure of choice to alleviate pain and restore extensor function.
During patellectomy, meticulous repair of the extensor retinaculum and the quadriceps-to-patellar tendon continuity is paramount to prevent extensor lag and ensure dynamic stability of the knee.
MALUNION OF THE FEMORAL CONDYLES
Biomechanical Implications
Malunion of one or both femoral condyles profoundly distorts the articular surface of the knee. While tibial plateau malunions are problematic, femoral condyle malunions frequently produce a much more severe and rapid functional disability due to the complex, multi-axial rolling and gliding motion of the femoral condyles during knee flexion.
- Lateral Femoral Condyle Malunion: Typically results in a triad of external rotation, flexion contracture, and valgus deformity of the knee.
- Medial Femoral Condyle Malunion: Produces a corresponding triad of internal rotation, flexion contracture, and varus deformity.
Lateral Femoral Condyle: Surgical Technique
Correction of a lateral femoral condyle malunion requires an intra-articular osteotomy to restore the joint line.
Preoperative Preparation and Positioning:
The patient is placed supine on a radiolucent table. A tourniquet is applied to the proximal thigh. Fluoroscopy must be available to confirm multi-planar alignment.
Step-by-Step Surgical Approach:
* Incision: Approach the joint through a lateral incision beginning 10 cm proximal to the knee joint line and extending distally to a point 2.5 cm distal and slightly anterior to the head of the fibula.
* Superficial Dissection: Incise the iliotibial band in line with its fibers.
Surgical Warning: Strictly identify and protect the common peroneal nerve as it courses posterior to the biceps femoris tendon and wraps around the fibular neck.
* Deep Dissection: Incise the vastus lateralis muscle fascia and retract the muscle belly anteriorly to expose the lateral femoral condyle and the site of the old fracture.
* Arthrotomy: Open the joint capsule and synovial membrane. Direct visualization of the interior of the joint is mandatory to ensure perfect anatomic reduction of the articular surface.
* Osteotomy: Divide the bone as near to the plane of the original fracture as possible using a thin oscillating saw or sharp osteotomes. Maintain absolute protection of the posterior neurovascular structures.
* Reduction and Provisional Fixation: Grasp the mobilized condyle with a large pointed bone-holding forceps. Manipulate it into its anatomic position, restoring the articular contour. Drill two smooth Kirschner wires (K-wires) through the lateral fragment into the intact medial condyle. The wires should cross each other at an angle of approximately 30 degrees for rotational stability and must protrude slightly through the opposite medial cortex to ensure adequate purchase.
* Radiographic Verification: Obtain precise two-plane (AP and lateral) radiographs to verify the position of the K-wires, the restoration of the joint line, and the overall mechanical axis.
* Definitive Fixation: Once alignment is confirmed, over-drill and fix the fragment with large fragment AO cancellous lag screws (typically 6.5 mm or 7.3 mm).
Management of Posterior Condylar Malunions:
To expose a malunited fracture isolated to the posterior aspect of the lateral condyle, utilize the same lateral incision but carry the deep dissection further posteriorly.
* Expose the biceps femoris tendon and the peroneal nerve, retracting them laterally and posteriorly with a vessel loop.
* Incise the posterolateral capsule to expose the fragment.
* The posterior fragment is almost universally displaced proximally due to the pull of the gastrocnemius. It usually can be refractured and mobilized from proximal to distal.
* Reduce the fragment with a towel clip and secure it with two AO cancellous lag screws.
* Fixation Augmentation: If screw fixation alone is not sufficiently rigid due to poor bone quality or comminution, a lateral buttress plate must be added to prevent proximal migration.
Medial Femoral Condyle
Malunion of the medial femoral condyle is corrected using the identical biomechanical principles described for the lateral condyle, utilizing a standard medial parapatellar or subvastus approach.
Pediatric Consideration: When the distal femoral physis is involved in a child, the surgeon must anticipate that growth of the distal femur may be permanently disturbed. Parents must be counseled regarding the high likelihood of future limb-length discrepancy or angular deformity requiring epiphysiodesis or lengthening procedures.
Both Femoral Condyles (Bicondylar Malunion)
Malunion of fractures involving both condyles with marked displacement is a devastating complication. It should rarely be corrected by open reduction and intra-articular osteotomy of each individual condyle, unless the malunion is of very short duration (less than 6-8 weeks) and occurs in a young, highly compliant patient with excellent bone stock.
For chronic bicondylar malunions presenting primarily with extra-articular varus or valgus deformity, the mechanical axis should be realigned via a corrective closing or opening wedge osteotomy through the distal femoral metaphysis, avoiding the scarred joint capsule entirely.
When the contour of the articular joint is severely irregular, leading to profound functional impairment and intractable pain, joint-sacrificing or joint-replacing procedures are indicated.

Fig. 55-16 Malunited comminuted fracture of both condyles of femur 1 year after injury. Knee motion was markedly limited and painful.
In young laborers or patients with active infection history, a compression arthrodesis is a highly durable salvage option.
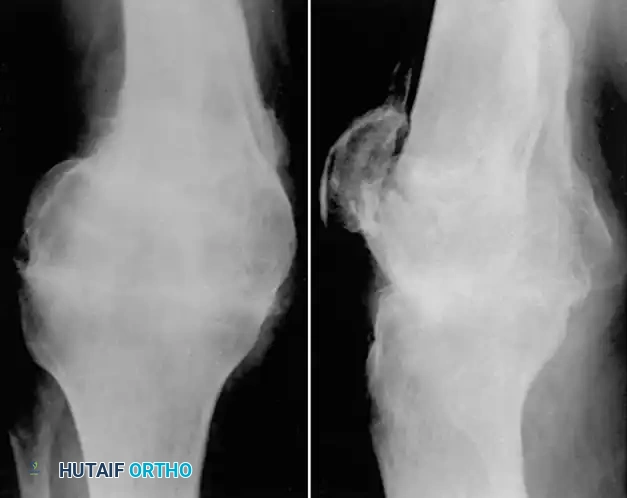
Fig. 55-17 Same patient as in Figure 55-16, 3.5 months after compression arthrodesis. Knee is painless and stable for heavy labor.
MALUNION OF THE FEMORAL SHAFT
Epidemiology and Clinical Evaluation
Historically common, malunions of the femoral shaft have become significantly less frequent with the universal adoption of interlocking intramedullary (IM) nailing for acute fractures. Today, diaphyseal malunions are typically seen following nonoperative treatment (traction/casting in developing regions), premature weight-bearing, or failure of initial fixation.
A femoral malunion becomes clinically significant and warrants surgical intervention if it results in:
1. Shortening: Greater than 2.5 cm.
2. Angulation: Greater than 10 degrees in the coronal (varus/valgus) or sagittal (procurvatum/recurvatum) planes.
3. Rotation: Internal or external rotation severe enough that the knee cannot be aligned with the forward vector of motion during the stance phase of gait.
The Impact of Rotational Deformity:
While many authors define rotational malunion as 10 degrees or more of axial malalignment, minor rotational deviations are often asymptomatic due to compensatory mechanisms in the hip and foot. However, Winquist et al. demonstrated that rotational malunions greater than 15 to 20 degrees are highly symptomatic, causing severe gait disturbances, patellofemoral pain, and secondary lumbar spine stress. Braten et al. corroborated this, noting that symptoms increased to 38% in patients with rotational deformities exceeding 15 degrees.
Preoperative Planning
Detailed preoperative planning, as championed by Mast, Teitze, and Gowda, is the cornerstone of successful deformity correction.
* Imaging: Obtain full-length, weight-bearing, standing radiographs of both the involved and uninvolved lower extremities. Computed Tomography (CT) scanograms are invaluable for precisely quantifying rotational discrepancies.
* Patient Optimization: Assess the patient’s overall medical condition, functional demands, and soft tissue envelope. Extensive scarring, compromised vascularity, or latent infection drastically alter the surgical approach.
Surgical Techniques for Diaphyseal Malunions
Femoral osteotomies in adults, particularly those involving acute lengthening, carry substantial risks, including deep infection, nerve palsies (especially the sciatic and femoral nerves), hardware failure, and nonunion.
Intramedullary Nailing
For aseptic malunions located from the lesser trochanter to within 5 cm of the intercondylar notch, osteotomy followed by fixation with a locked intramedullary nail is the gold standard. This technique offers superior biomechanical stability (load-sharing) and allows for early mobilization.
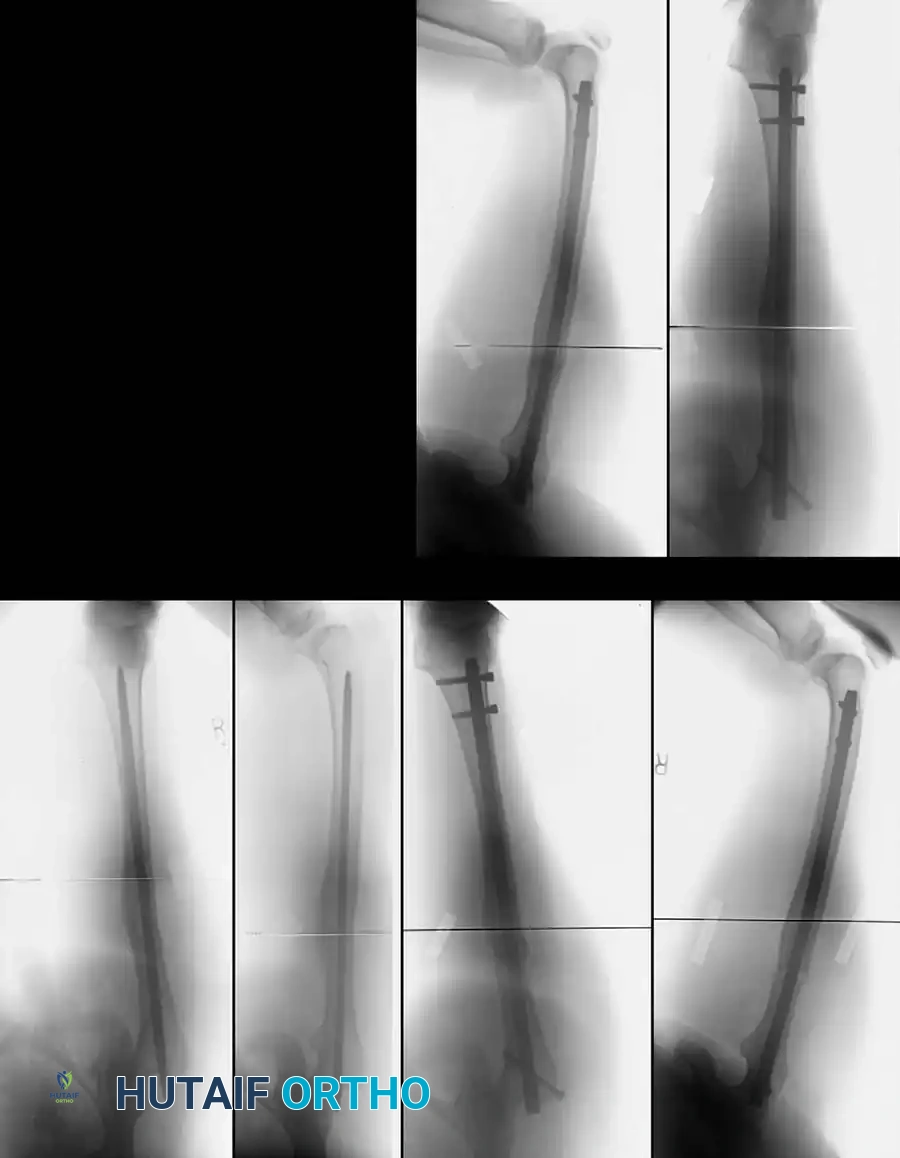
Fig. 55-18 A, Rotational malunion of femur after unlocked intramedullary nailing. B, Correction of malunion with proximal femoral derotational osteotomy and locked nailing. C, Healed osteotomy.
Technique:
1. Place the patient supine or lateral on a fracture table.
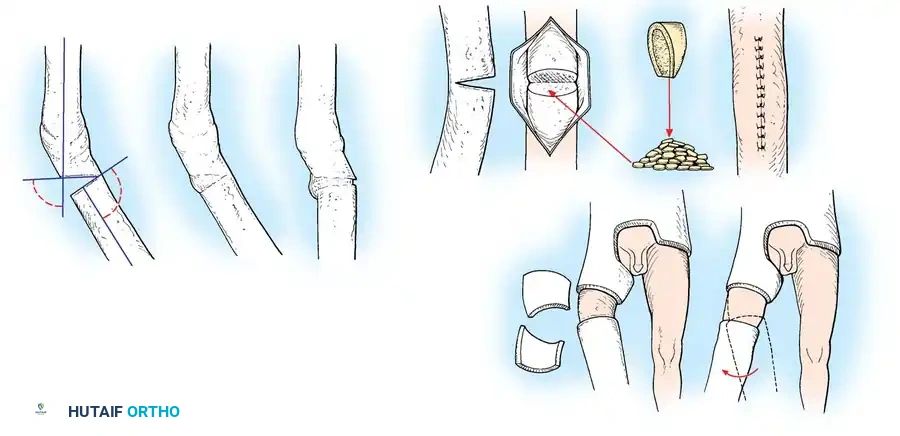
2. Expose the malunion site. The bone is divided through the plane of the malunion using a reciprocating saw. Alternatively, to minimize thermal necrosis, the plane can be outlined with multiple drill holes and completed with a sharp osteotome.
3. Ream the medullary canal sequentially.
4. Insert the interlocking nail, ensuring rotational correction is held perfectly before deploying the distal locking screws.
5. Autogenous iliac crest bone grafting is highly recommended to stimulate osteogenesis at the osteotomy site.
Clinical example demonstrating restoration of the mechanical axis using a statically locked intramedullary nail following diaphyseal osteotomy.
Plate Osteosynthesis and External Fixation
For patients with distorted medullary canals, extremely distal/proximal fractures, or those who do not fulfill the criteria for IM nailing, open reduction and internal fixation with broad dynamic compression plates (DCP) or locking compression plates (LCP) is indicated.

Fig. 55-19 A, Distal femoral fracture with 30-degree varus malunion. B, External fixation was used to correct deformity before plating. C, After osteotomy and plating.
Müller, Strosche, and Scheuer reported high union rates using plate osteosynthesis combined with autogenous bone grafting for angular and rotational deformities. Chiodo et al. successfully utilized oblique osteotomies combined with closing wedges to correct multi-planar deformities (coronal, transverse, and sagittal), stabilizing them with 4.5-mm plates.
Radiographic progression of a complex diaphyseal malunion managed with robust plate osteosynthesis and structural bone grafting.
If the malunion is of short duration and features overlapping fragments without consolidation, it can sometimes be mobilized manually. Graduated distraction with an external fixation assembly (such as an Ilizarov or Taylor Spatial Frame) can slowly correct shortening and angulation, mitigating the risk of acute sciatic nerve stretch palsy.
Subtrochanteric Malunions
Malunions in the proximal third of the femur, particularly the subtrochanteric region, are subjected to massive deforming forces (flexion, abduction, and external rotation from the iliopsoas and gluteal musculature).

Fig. 55-20 A and B, Malunion of subtrochanteric fracture with severe internal rotational deformity. C and D, Corrective osteotomy, implant removal, and fixation with proximal interlocking Grosse-Kempf medullary nail.
These require robust fixation using a cephalo-medullary interlocking nail (reconstruction nail), a 95-degree blade plate, or a dynamic condylar screw system inverted for proximal use.
Advanced Lengthening Osteotomies
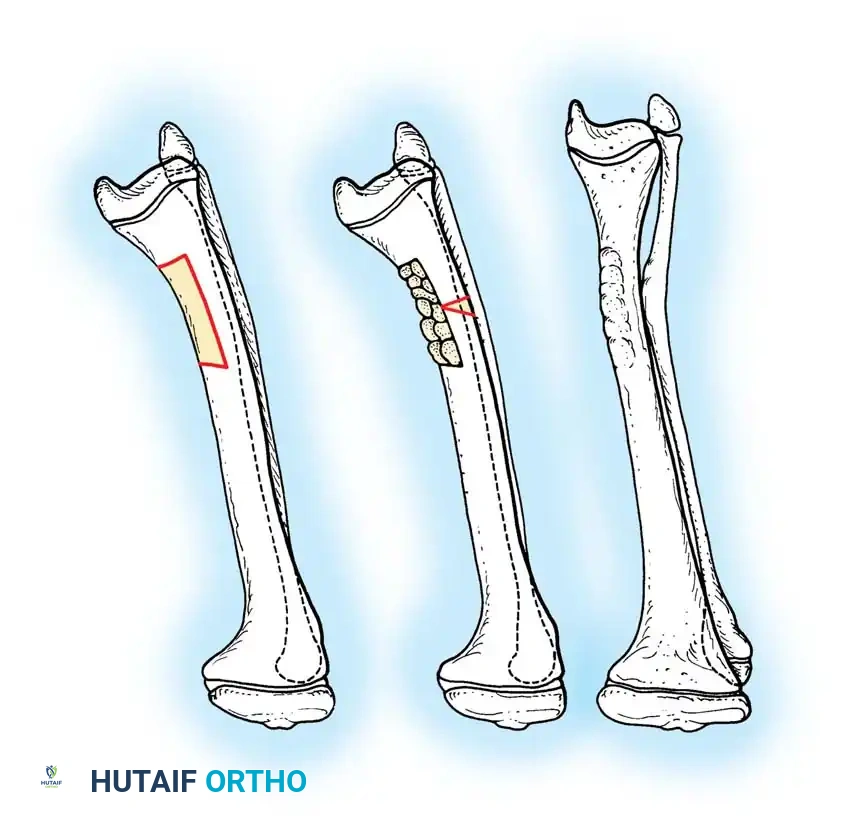
When significant shortening accompanies the malunion, one-stage femoral lengthening can be performed, though it is technically demanding. Kempf, Grosse, and Abalo popularized the Z-step osteotomy stabilized with a dynamically locked intramedullary nail.
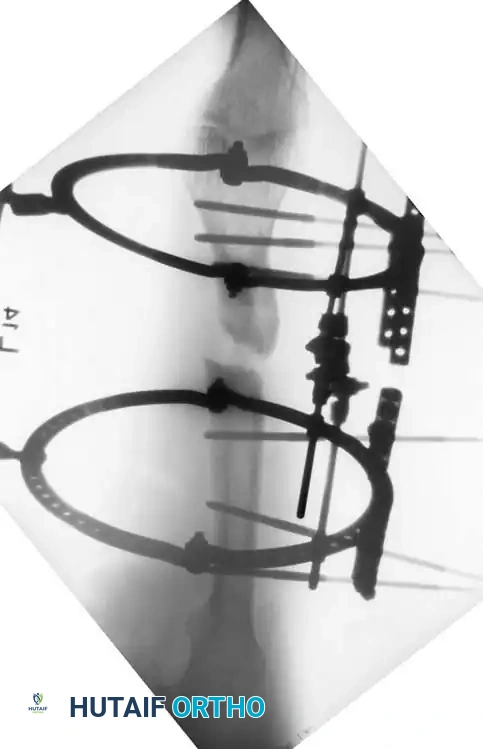
Fig. 55-21 One-stage femoral lengthening: reaming, Z-shaped osteotomy, lengthening, static locked medullary nailing, transverse screws, and bone grafts.
Surgical Warning: Acute lengthening of the femur beyond 3-4 cm carries a high risk of femoral or sciatic nerve neurapraxia. Kempf et al. recommended keeping the patient on strict bed rest with the hip flexed 30 degrees and the knee flexed 90 degrees for 48 hours postoperatively to relax the neurovascular tension.
Murray, Kambouroglou, and Kenwright reported excellent results with one-stage lengthening (averaging 4 cm) using diaphyseal osteotomies stabilized by IM nails or plates, provided the soft tissue envelope was pristine. They emphasized that extensive scarring or previous infection are absolute contraindications for acute one-stage lengthening, favoring gradual distraction osteogenesis in such scenarios.

Complex multi-planar correction utilizing advanced osteosynthesis techniques to restore length and rotation simultaneously.
Postoperative Protocol
The postoperative rehabilitation protocol is dictated by the stability of the fixation achieved.
* Intramedullary Nailing: If rigid interlocking fixation is achieved, patients may begin immediate active and passive range of motion (ROM) of the hip and knee. Touch-down weight-bearing (TDWB) is permitted, advancing to full weight-bearing as radiographic callus appears (typically 6-8 weeks).
* Plate Fixation / Intra-articular Osteotomies: For condylar osteotomies or plate fixation, the limb is often placed in a hinged knee brace. Weight-bearing is strictly restricted for 8 to 12 weeks until definitive radiographic union is confirmed. Early continuous passive motion (CPM) is critical to prevent intra-articular adhesions and arthrofibrosis.
* DVT Prophylaxis: Given the extensive nature of these reconstructive procedures, chemical thromboprophylaxis is mandatory for a minimum of 28 days postoperatively, alongside mechanical compression devices.
