Mastering the Proximal First Metatarsal Osteotomy: Principles and Techniques
Key Takeaway
Proximal first metatarsal osteotomy is a powerful surgical intervention indicated for severe hallux valgus deformities characterized by an intermetatarsal angle exceeding 10 degrees and a hallux valgus angle greater than 35 degrees. By correcting the metatarsus primus varus near its apex, surgeons achieve substantial distal correction. This comprehensive guide details the biomechanical rationale, step-by-step surgical techniques, stabilization protocols, and postoperative management required to optimize patient outcomes and prevent complications like transfer metatarsalgia.
INTRODUCTION TO PROXIMAL FIRST METATARSAL OSTEOTOMY
Hallux valgus is a complex, three-dimensional deformity characterized by lateral deviation of the great toe and medial deviation of the first metatarsal (metatarsus primus varus). When primary or secondary varus of the first metatarsal significantly contributes to the hallux valgus complex, surgical correction near the origin of the deformity—the proximal metatarsal—is biomechanically sound and clinically highly effective.
A proximal first metatarsal osteotomy, combined with a distal soft tissue procedure at the first metatarsophalangeal (MTP) joint, allows for profound correction of the intermetatarsal angle (IMA). Because the osteotomy is performed at the base of the metatarsal, even a few degrees of angular shift translates into a marked geometric improvement at the distal articular end. This effectively narrows the forefoot, restores the mechanical axis of the first ray, and dramatically reduces the chance of recurrent pressure symptoms over the medial eminence (bunion).
INDICATIONS AND PATIENT SELECTION
Patient selection is paramount. The proximal osteotomy is a technically demanding procedure reserved for moderate to severe deformities where distal procedures alone would fail to adequately reduce the intermetatarsal angle.
Clinical and Radiographic Criteria
A patient may benefit from a proximal metatarsal osteotomy and a concomitant distal soft tissue procedure if they meet the following criteria:
* Hallux Valgus Angle (HVA): Greater than 35 degrees.
* Intermetatarsal Angle (IMA): Greater than 10 degrees (or a 1st-to-5th intermetatarsal angle of ≥ 30 degrees combined with an HVA of ≥ 35 degrees).
* Joint Viability: Absence of significant degenerative arthritis (hallux rigidus) in the first MTP joint.
* First Ray Mobility: Absence of gross hypermobility at the first tarsometatarsal (TMT) joint, which might otherwise necessitate a Lapidus arthrodesis.
Clinical Pearl: Deformities with intermetatarsal angles of 13 degrees or less and hallux valgus angles of 30 degrees or less can typically be corrected by less technically demanding distal procedures (e.g., distal chevron osteotomy). Reserve the proximal osteotomy for severe metatarsus primus varus.
BIOMECHANICAL RATIONALE: ADVANTAGES AND DISADVANTAGES
Understanding the biomechanics of the first ray is critical for executing a successful proximal osteotomy. The goal is to translate the metatarsal head laterally, reduce the sesamoid complex, and maintain or slightly plantarflex the first ray to ensure appropriate load-bearing.
Advantages of the Proximal Approach
- Favorable Healing Environment: The base of the first metatarsal is rich in cancellous bone. The broad contact surfaces of the osteotomy fragments promote early clinical stability (within 3 to 5 weeks) and robust radiographic union (within 6 to 8 weeks).
- Magnified Distal Correction: Due to the center of rotation of angulation (CORA), small angular changes at the proximal osteotomy produce excellent, large-magnitude correction at the distal end of the metatarsal where the patient's symptoms are located.
- Preservation of Metatarsal Length: The metatarsal is shortened minimally, if at all. The width of the saw blade cut is more than compensated for by the geometric "straightening" of the bone.
- Correction of Severe Deformity: Large angles between the first and second metatarsals can be reliably corrected.
- Prevention of Transfer Lesions: By intentionally tilting the distal fragment slightly plantarward during fixation, the surgeon increases the load-bearing capacity of the first ray, thereby decreasing the load on the lesser metatarsals and preventing transfer metatarsalgia.
- Cosmesis and Footwear: Significant narrowing of the forefoot improves the variety of footwear the patient can tolerate and yields an excellent cosmetic result.
Disadvantages and Surgical Risks
- Soft Tissue Disruption: Traditional open proximal osteotomies require extensive soft tissue dissection.
- Instability and Displacement: The distal fragment has a strong tendency to displace dorsally or migrate medially back to its original position due to the pull of the tibialis anterior and ground reaction forces. Secure internal fixation is absolute.
- Transfer Metatarsalgia Risk: If the distal fragment displaces dorsally or migrates, the second ray will become overloaded, leading to intractable plantar keratosis and pain.
- Incision Burden: Three separate incisions are often required if a traditional dorsal basilar osteotomy is performed alongside a distal soft tissue release.
- Anesthetic Challenges: The procedure is more difficult to perform under simple regional block anesthesia compared to distal osteotomies.
- Prolonged Convalescence: Immediate postoperative recovery is usually characterized by more pain, swelling, and immobility than a distally placed osteotomy. Cast immobilization or strict adherence to rigid postoperative footwear is frequently needed.
OVERVIEW OF PROXIMAL OSTEOTOMY TECHNIQUES
Currently, the most frequently utilized open proximal metatarsal osteotomies include the crescentic, chevron, Ludloff, and scarf osteotomies.
Surgical Warning: The specific technique or geometry of the proximal osteotomy is not as important as meticulous attention to surgical detail. Any proximal osteotomy that allows the first metatarsal to deviate laterally and remain rigidly stable in that position—with absolutely no dorsal tilt to the distal fragment—will accomplish the goal of narrowing the IMA.
Overcorrection of the IMA is possible but should be avoided through careful intraoperative fluoroscopic assessment. Furthermore, if the hallucal sesamoids are not anatomically reduced into their respective facets on the plantar aspect of the metatarsal head, recurrent metatarsus primus varus and hallux valgus will inevitably occur regardless of the degree of bony correction achieved proximally.
MINIMALLY INVASIVE AND PERCUTANEOUS TECHNIQUES
While traditional open proximal osteotomies are highly effective, advancements in minimally invasive surgery (MIS) have introduced percutaneous techniques that achieve powerful correction with intramedullary stabilization extending to the proximal metatarsal base. The percutaneous distal metatarsal osteotomy (e.g., Magnan technique) utilizes a distal-to-proximal intramedullary Kirschner wire (K-wire) to achieve the biomechanical stability traditionally reserved for proximal basilar osteotomies.
Step-by-Step Percutaneous Technique with Proximal Stabilization
The following technique details a percutaneous approach where the osteotomy is performed distally, but stabilization relies entirely on anchoring the fixation deep into the proximal metatarsal base.
1. Osteotomy Execution
A percutaneous transverse or slightly oblique osteotomy is performed at the metatarsal neck using a specialized Shannon burr under fluoroscopic guidance. The distal fragment is translated laterally to correct the IMA. Slight overcorrection is advisable in this specific technique to allow for the early removal of the K-wire without loss of alignment.
2. Intramedullary Stabilization
Rigid stabilization is the most critical step. The fixation must bridge the osteotomy and anchor securely into the proximal metaphysis.
- Use a mallet to drive a stout Kirschner wire (typically 2.0 mm) from distal to proximal, entering the medial aspect of the distal fragment and passing into the medullary canal of the first metatarsal.
- To ensure absolute biomechanical stability, drive the wire as far as the base of the first metatarsal, engaging the dense cancellous bone proximally.

FIGURE 81-36 Percutaneous distal metatarsal osteotomy. The Kirschner wire is driven firmly as far as the base of the first metatarsal to improve stabilization.
Clinical Pearl: In this specific percutaneous technique, no formal open soft tissue procedures—including lateral release—are performed. The lateral translation of the capital fragment effectively decompresses the joint and realigns the soft tissue envelope.
3. Final Adjustments and Fluoroscopic Verification
Once the wire is seated proximally, the alignment and hardware placement must be rigorously verified.
- Carefully remove any grooved instruments or tissue protectors used during wire insertion.
- Obtain a true lateral fluoroscopic image to check the trajectory and final position of the K-wire. Ensure the wire has not breached the dorsal or plantar cortices and is firmly seated in the proximal base without causing dorsal elevation of the capital fragment.

FIGURE 81-37 Percutaneous distal metatarsal osteotomy. Lateral fluoroscopic view shows the position of the Kirschner wire.
4. Soft Tissue Management
Because the capital fragment has been translated laterally, the medial skin and soft tissues may become tethered or invaginated around the K-wire insertion site.
- Using a small hemostat or tenotomy scissors, gently release the soft tissue at the level of the skin incision to prevent skin necrosis and alleviate tension.
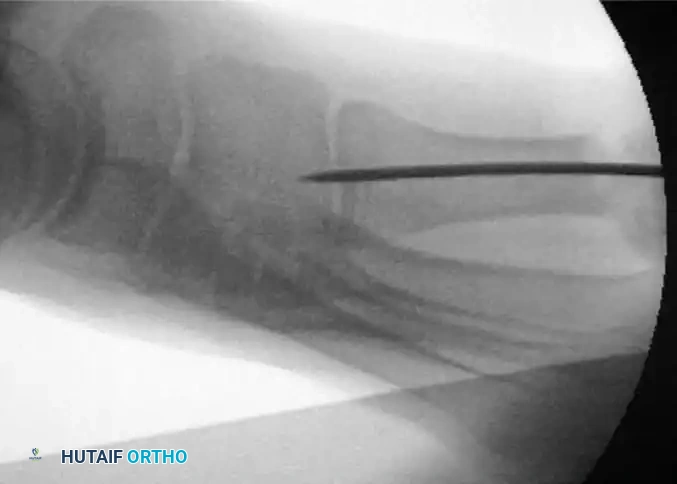
FIGURE 81-38A Percutaneous distal metatarsal osteotomy. The soft tissue is released at the level of the skin incision.
5. Wire Modification and Closure
The protruding K-wire must be managed to prevent migration and to assist in postoperative dressing application.
- Bend the Kirschner wire approximately 90 degrees outside the skin before cutting it. This bent tip prevents proximal migration of the wire into the foot and serves as a crucial anchor point for the postoperative taping protocol.
- Close the small percutaneous incision with a single non-absorbable suture.

FIGURE 81-38B Percutaneous distal metatarsal osteotomy. The tip of the Kirschner wire is bent before cutting.
POSTOPERATIVE CARE AND REHABILITATION
The success of a metatarsal osteotomy relies as much on meticulous postoperative care as it does on intraoperative execution. The rehabilitation protocol is designed to protect the osteotomy, prevent dorsal malunion, and restore first MTP joint kinematics.
Taping and Padding Protocol
- Duration: The hallux is taped in the corrected position for a minimum of 6 weeks.
- Frequency: The tape must be replaced every week by the surgical team to ensure tension is maintained as swelling subsides.
- Hyper-correction: The taping should maintain a slight hyper-correction of the hallux (slight varus) to counter the natural soft-tissue tendency toward recurrence of the valgus deformity.
- Plantar Padding: A plantar kidney-shaped pad is strictly utilized. The concavity of the pad should surround the plantar aspect of the first metatarsal head. This serves a dual purpose: it reduces local weight-bearing pressure beneath the capital fragment and physically prevents dorsiflexion (elevation) of the fragment during the healing phase.
Weight-Bearing and Mobilization
- Immediate Post-Op: Patients are generally allowed to walk on the day after surgery, provided they strictly use a postoperative shoe with a flat, rigid sole. The rigid sole prevents bending moments across the osteotomy site.
- Transition: At 6 weeks, clinical and radiographic union is assessed. If bridging callus is present and the osteotomy is stable, the K-wire (if used) is removed, and the tape is discontinued.
- Range of Motion (ROM): After tape removal at 6 weeks, patients are strongly encouraged to begin active and passive ROM exercises of the first MTP joint. Particular care and physical therapy should be directed toward obtaining full dorsiflexion within 4 to 6 weeks following immobilization removal, as stiffness is a common complication.
COMPLICATIONS AND PITFALLS
Surgeons performing proximal metatarsal osteotomies must be vigilant regarding several severe complications:
- Dorsal Malunion: The most devastating complication. Even a few millimeters of dorsal elevation at the proximal osteotomy site will completely unload the first ray during the terminal stance phase of gait, leading to severe, intractable transfer metatarsalgia beneath the second and third metatarsal heads.
- Nonunion/Delayed Union: While the proximal metaphysis has excellent healing potential, thermal necrosis from aggressive saw use or inadequate rigid fixation can lead to nonunion.
- Hallux Varus: Overcorrection of the IMA, excessive lateral release, or over-tightening of the medial capsule can result in an iatrogenic hallux varus, which is often more symptomatic for the patient than the original deformity.
- Avascular Necrosis (AVN): Extensive stripping of the lateral capsular structures combined with a proximal osteotomy can disrupt the blood supply to the metatarsal head, though this is less common with basilar osteotomies than with distal chevron osteotomies.
By adhering to strict biomechanical principles, ensuring rigid internal fixation, and executing a flawless postoperative protocol, the proximal first metatarsal osteotomy remains one of the most powerful tools in the orthopedic surgeon's armamentarium for the correction of severe hallux valgus.
===END===
You Might Also Like

