Pathophysiology and Classifications of Osteoarthritis
Osteoarthritis (OA) is the clinical endpoint of a complex cascade of mechanical and biological events that destabilize the normal homeostatic processes of degradation and synthesis within the articular joint. This destabilization affects articular cartilage chondrocytes, the extracellular matrix, and the subchondral bone. At the cellular level, these changes are characterized by an initial increase in water content, a subsequent decrease in proteoglycan concentration, and an altered collagen matrix architecture. This biochemical degradation is mediated by matrix metalloproteinases (MMPs) and pro-inflammatory cytokines (e.g., IL-1β, TNF-α), ultimately leading to the irreversible deterioration of articular cartilage.
Osteoarthritis is broadly classified into primary and secondary types:
* Primary Osteoarthritis: Generally presents as a polyarticular degenerative arthritis of idiopathic origin. It may be active simultaneously in several joints and rarely manifests before the age of 35. Progression is typically insidious, slow, and relentless. It is highly correlated with obesity, particularly in weight-bearing joints, and is prevalent in patients over 50 years of age. Occupational hazards requiring heavy lifting and elite sporting activities have been strongly associated with primary OA of the hip, though the correlation with knee OA remains multifactorial.
* Secondary Osteoarthritis: Usually monoarticular, arising as a direct reaction of the joint to a pre-existing condition that has produced articular incongruity. Common etiologies include mechanical derangement, pyogenic infection, congenital anomalies (e.g., developmental dysplasia of the hip), physeal separation, chronic ligamentous instability, and intra-articular fractures.
Clinical Pearl: The prognosis is generally more favorable for primary polyarticular degenerative arthritis than for secondary osteoarthritis, as the latter often presents with severe, localized mechanical deficits that accelerate joint destruction.
Osteoarthritis of the Upper Extremity: The Elbow
While the elbow is a non-weight-bearing joint, it is highly susceptible to degenerative changes secondary to trauma, repetitive microtrauma, or inflammatory arthropathies such as rheumatoid arthritis (RA).
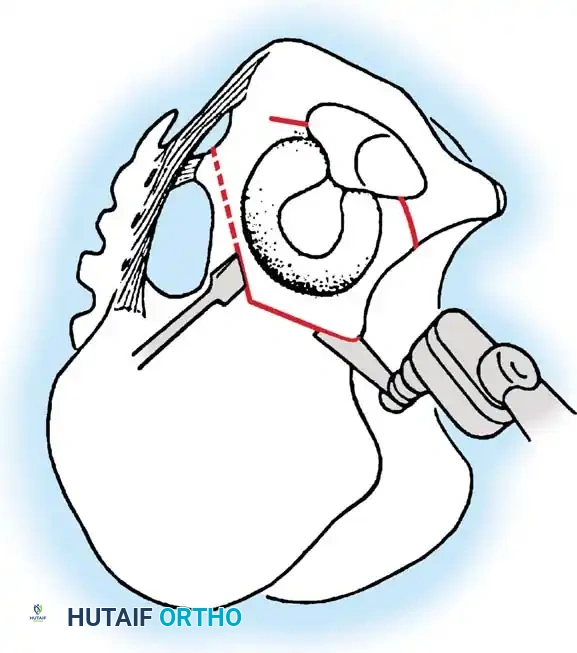
Synovectomy and Radial Head Excision
In cases of advanced synovial hypertrophy and radiocapitellar degeneration, synovectomy combined with radial head excision can provide significant pain relief and improve the arc of motion.
Surgical Technique:
1. Positioning: The patient is placed in the lateral decubitus or supine position with the arm draped over a chest roll. A sterile tourniquet is applied.
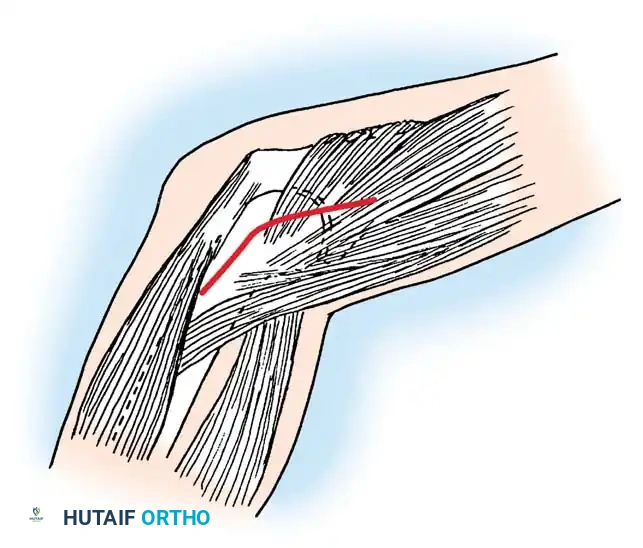
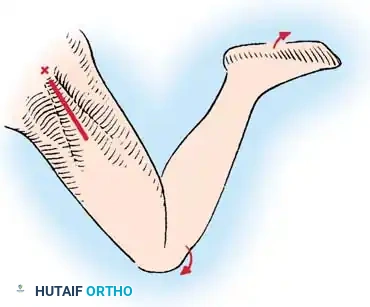
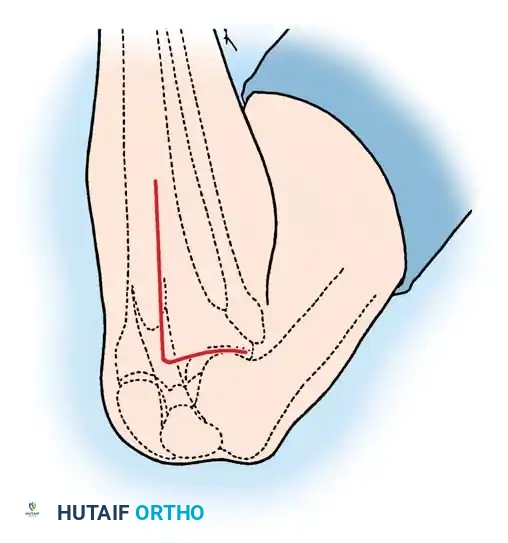
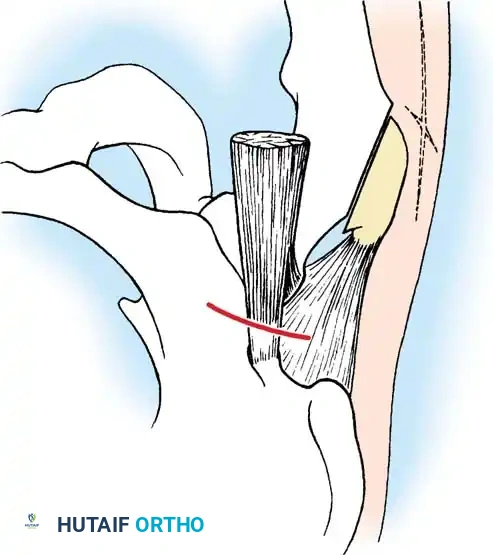
2. Approach: A lateral (Kocher) incision is utilized, extending from the lateral epicondyle distally toward the ulna.
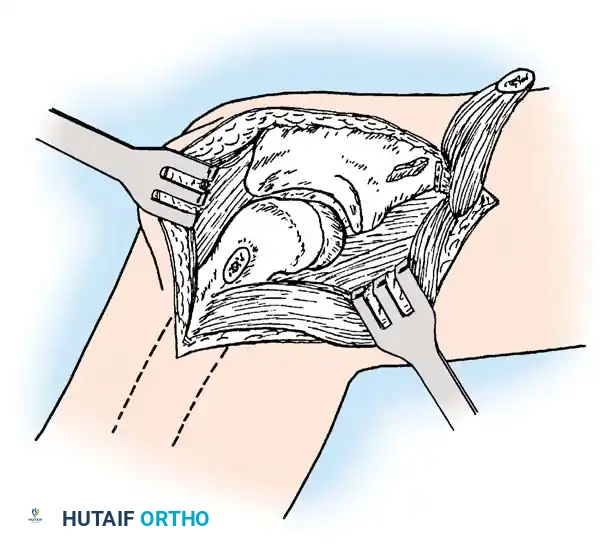
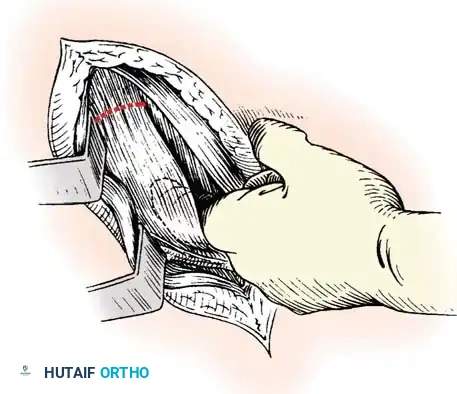
3. Exposure: The joint is exposed by freeing and reflecting the common origin of the extensor muscles. The anconeus and extensor carpi ulnaris are separated to access the capsule.
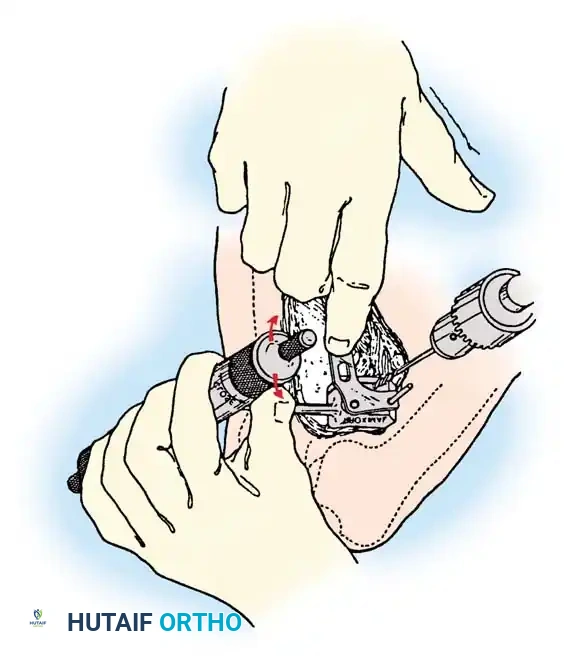
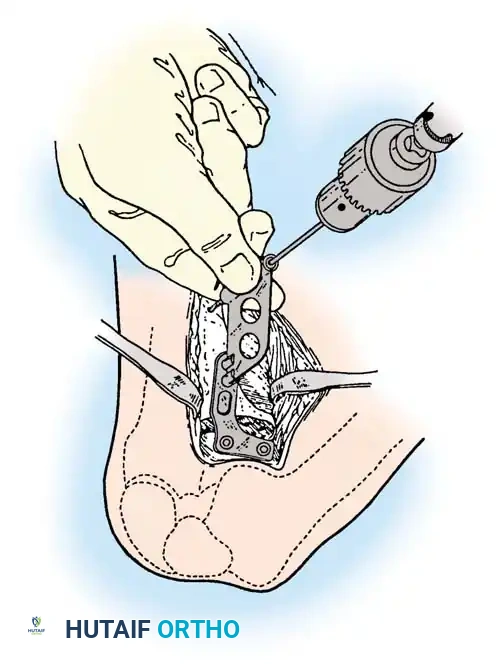
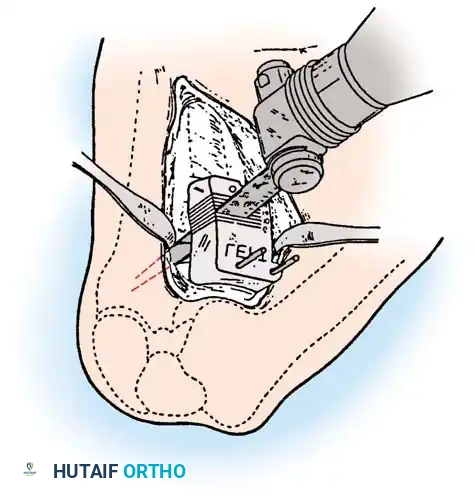
4. Excision: The radial head is identified, and a microsaw or osteotome is used to excise it at the level of the annular ligament, ensuring no impingement occurs during pronation and supination.
5. Synovectomy: A thorough anterior and posterior synovectomy is performed, meticulously protecting the lateral ulnar collateral ligament (LUCL) to prevent iatrogenic posterolateral rotatory instability.
Postoperative Protocol:
* Remove the tourniquet, elevate the arm, and apply compression for several minutes to achieve hemostasis.
* Close the capsule over a closed-suction drain.
* Close the remainder of the wound in a routine layered fashion.
* Apply a bulky compression dressing followed by a posterior plaster long-arm splint.
* Rehabilitation: Because pain is usually mild, active-assisted motion of the elbow is initiated approximately 4 days postoperatively. As strength improves, exercises progress to active motion. Pain typically decreases over 3 months, with motion continuing to improve for up to 6 months.
Total Elbow Arthroplasty (TEA)
The most common diagnosis for which total elbow arthroplasty is performed is rheumatoid arthritis, yielding satisfactory results in approximately 90% of patients.
Outcomes and Evidence:
* Ewald et al. reported on 202 capitellocondylar prostheses with a 2- to 15-year follow-up. Pain relief and functional improvement were excellent (average score improved from 26 to 91 on a 100-point scale). Reoperation for loosening, dislocation, or infection occurred in only 5%.
* Inglis and Figgie reported 77% good or excellent results in 137 semiconstrained total elbow replacements for RA.
* Gill and Morrey demonstrated a 92.4% survival rate at 10 to 15 years using the Mayo modified Coonrad semiconstrained prosthesis.

Surgical Warning: When performing TEA, meticulous handling of the ulnar nerve is mandatory. Routine ulnar nerve transposition is often performed to prevent postoperative neuropathy, especially in patients with pre-existing flexion contractures.
Osteoarthritis of the Foot and Ankle
Polyarticular osteoarthritis of the foot and ankle can cause debilitating symptoms that justify the fusion of one or more joints. More frequently, operative intervention is indicated for monoarticular arthritis of static or traumatic origin. Conditions such as hallux valgus, hallux rigidus, pes planus, or malunions of the foot and ankle bones often require corrective osteotomies or localized arthrodesis to restore plantigrade biomechanics and alleviate pain.
Osteoarthritis of the Knee: Comprehensive Management
Osteoarthritis of the knee presents with symptoms ranging from mild, activity-related aching to severe, disabling rest pain. The choice of procedure depends heavily on the patient’s age, activity expectations, disease severity, and the number of compartments involved.
Nonoperative Management
Initial management must be nonoperative and multidisciplinary:
* Physical therapy (quadriceps and hamstring strengthening).
* Unloader bracing and orthoses.
* Ambulatory aids.
* Pharmacologic intervention: NSAIDs, acetaminophen.
* Intra-articular injections: Corticosteroids or hyaluronic acid (viscosupplementation).
* Weight loss: Obesity is a primary risk factor; weight reduction significantly slows disease progression.
Arthroscopic Debridement and Lavage
Surgical debridement of the osteoarthritic knee generally includes limited synovectomy, excision of impinging osteophytes, removal of loose bodies, chondroplasty, and resection of unstable meniscal tears. Historically, open debridement (as postulated by Magnuson) was utilized, but it required extensive rehabilitation. Today, arthroscopic techniques are the gold standard for joint preservation in early OA.
The Evidence and The "Placebo" Debate:
* Hubbard reported that 60% of patients undergoing arthroscopic debridement were pain-free at 5 years, compared to only 12% in a lavage-only group.
* Moseley et al. (2002) published a landmark placebo-controlled, randomized study of 180 patients, concluding there was no significant difference in outcomes between arthroscopic debridement, lavage, and sham surgery.
* Dervin et al. prospectively evaluated 126 arthroscopic debridement procedures and found that 44% had significant pain relief at 2 years.
Prognostic Factors for Arthroscopic Debridement:
Patient selection is paramount. Age should not be the sole criterion.
* Good Prognosis: Short duration of symptoms, mechanical symptoms (catching/locking), normal alignment, medial joint line tenderness, unstable meniscal flap tear identified at arthroscopy.
* Poor Prognosis: Long duration of symptoms, insidious onset, severe bicompartmental or tricompartmental disease, malalignment (varus > 10 degrees, valgus > 15 degrees), pending litigation or workers' compensation claims.
Surgical Pearl: During arthroscopy, avoid aggressive resection of meniscal tissue and stable articular cartilage. Over-resection eliminates the crucial hoop stresses of the meniscus, rapidly accelerating the progression of osteoarthritis.
Marrow Stimulation and Chondroplasty
To address full-thickness chondral defects, marrow stimulation techniques aim to breach the subchondral bone plate, allowing multipotent mesenchymal stem cells from the bone marrow to form a fibrocartilage clot.
* Pridie Drilling: Introduced the concept of drilling exposed bony lesions to vascular marrow.
* Abrasion Chondroplasty: Promoted by Johnson, this involves using an arthroscopic burr to remove 1 to 2 mm of sclerotic subchondral bone. It is contraindicated in patients with inflammatory arthritis, significant stiffness, or those unable to comply with strict non-weight-bearing protocols for 2 months postoperatively.
* Microfracture: Currently the preferred marrow stimulation technique, utilizing arthroscopic awls to create precise perforations without the thermal necrosis associated with drilling.
Osteochondral and Autologous Chondrocyte Transplantation
For younger, active patients with focal, deep cartilage defects, advanced restoration techniques are indicated.
* Osteochondral Allografting: Meyers et al. reported satisfactory results in 77.5% of knees at 2 to 10 years. Jamali et al. described fresh osteochondral allografting as an excellent salvage procedure for severe patellofemoral degeneration.
* Autologous Chondrocyte Implantation (ACI): Brittberg et al. pioneered this two-stage procedure. Healthy chondrocytes are harvested, cultured, and re-implanted under a periosteal patch (or collagen membrane). Results are highly favorable for femoral condyle defects but less predictable for patellar lesions.
Corrective Osteotomy of the Knee
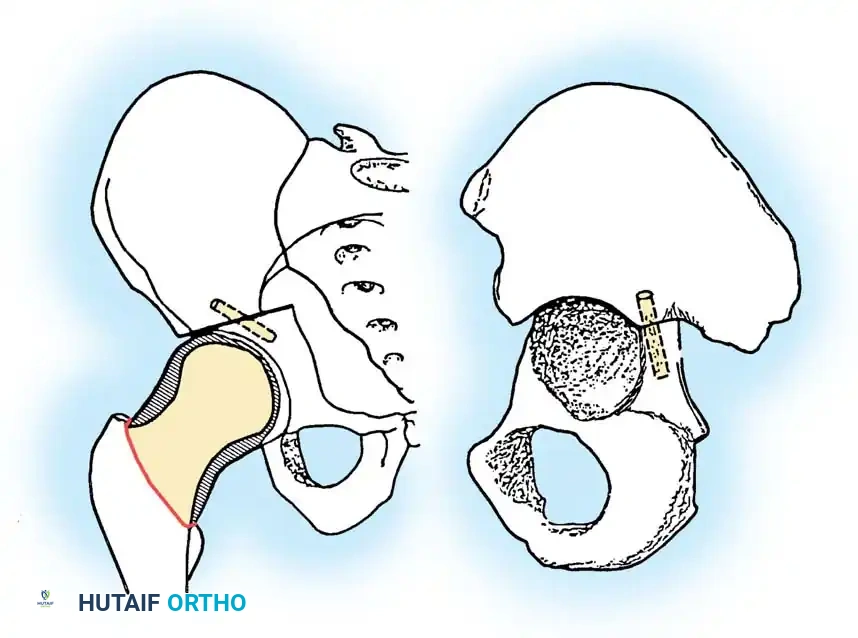
When osteoarthritis is unicompartmental and associated with mechanical malalignment (varus or valgus), corrective osteotomy is a powerful joint-preserving procedure. By realigning the mechanical axis, load is transferred from the diseased compartment to the relatively healthy compartment.
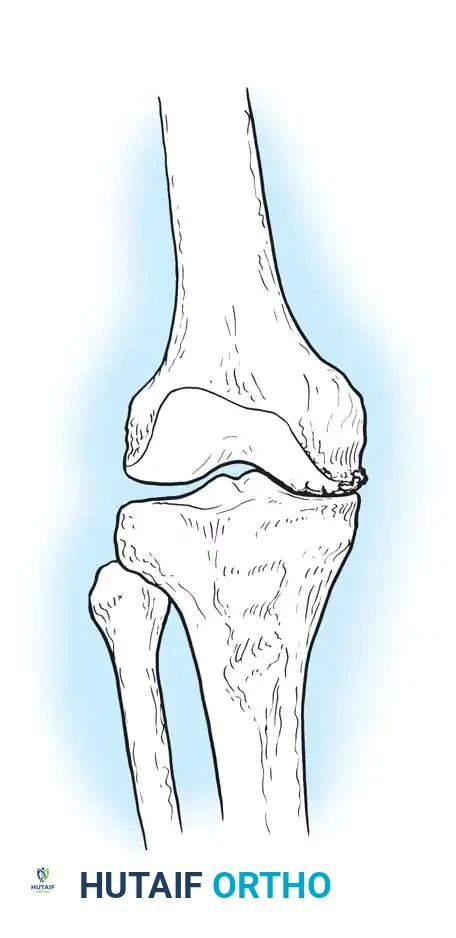
High Tibial Osteotomy (HTO)
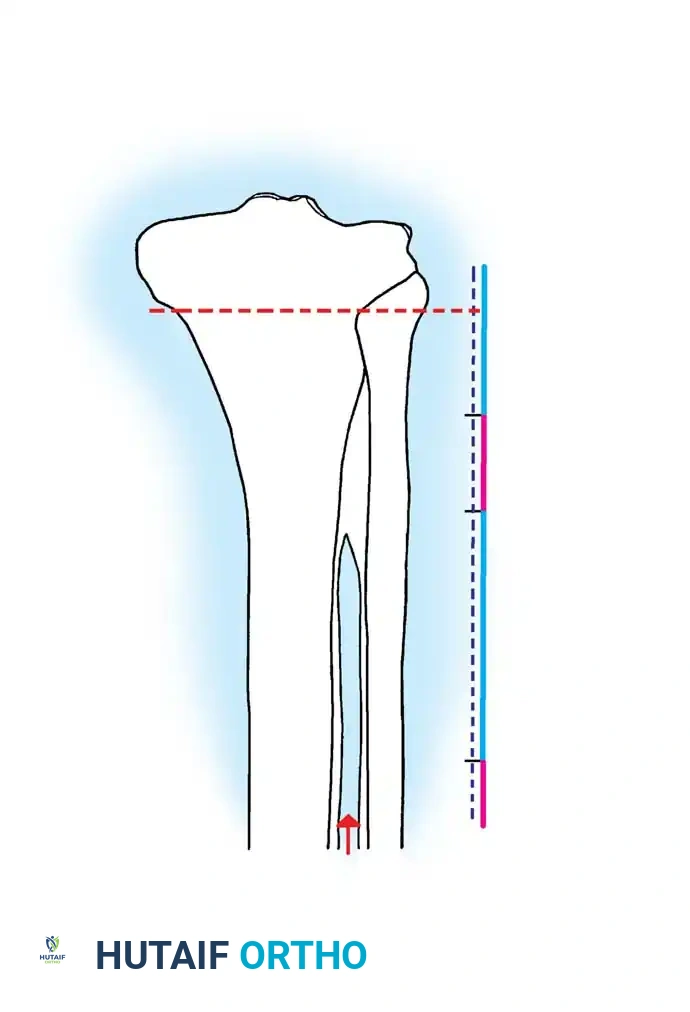
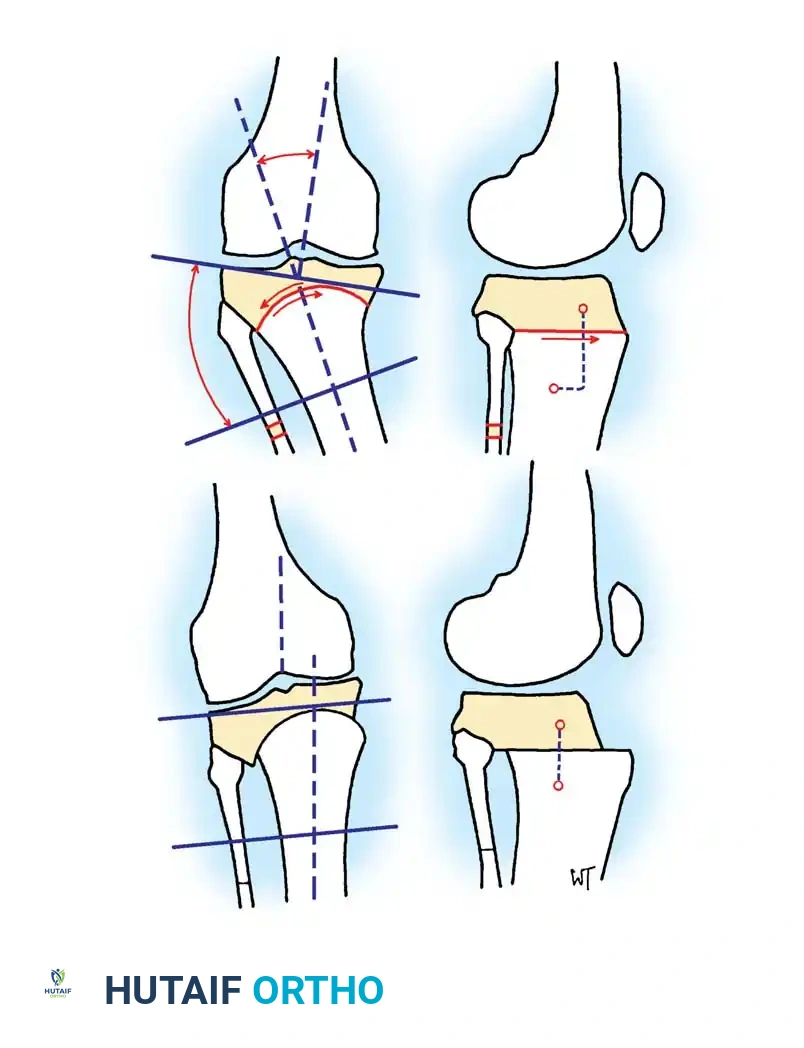
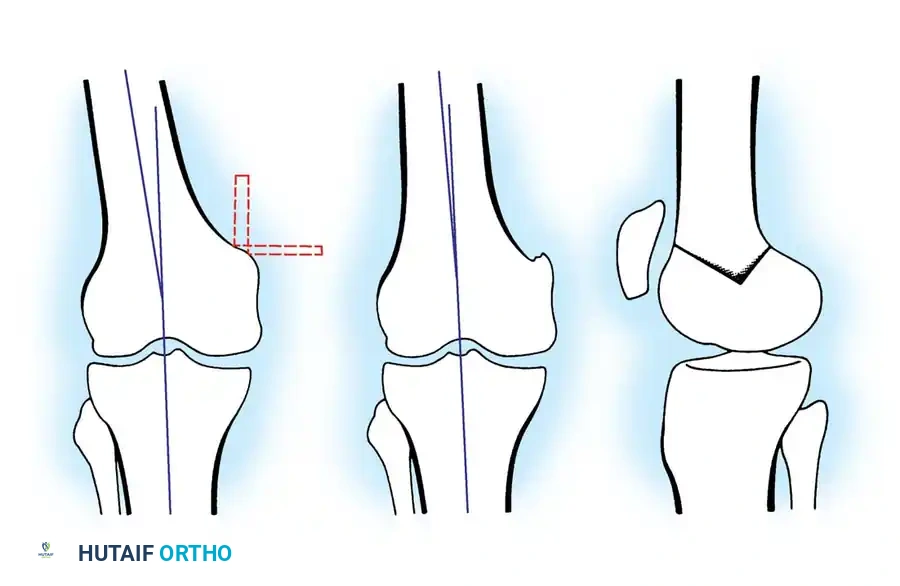
HTO is primarily indicated for medial compartment osteoarthritis associated with varus deformity. The goal is to shift the mechanical weight-bearing axis slightly lateral to the midline of the knee joint (the Fujisawa point, typically 62% of the tibial width from the medial edge).
Surgical Approaches:
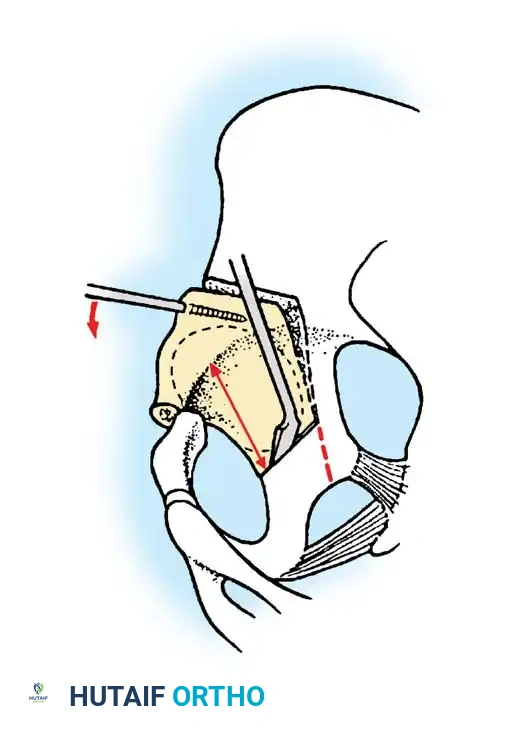
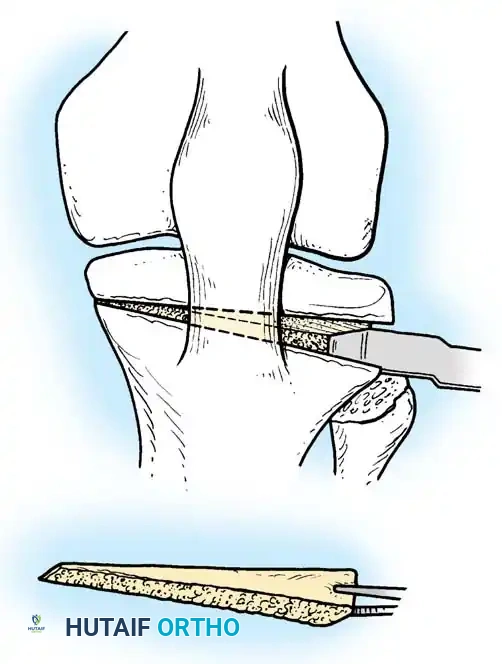
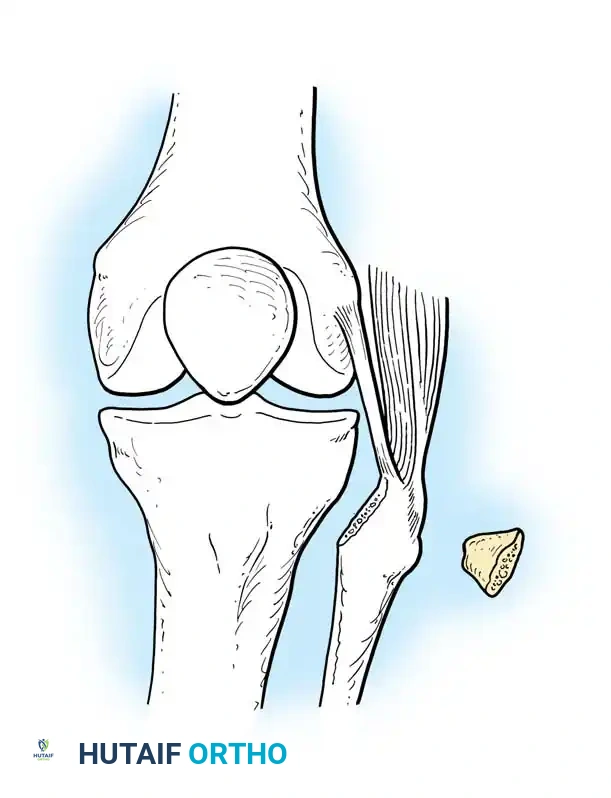
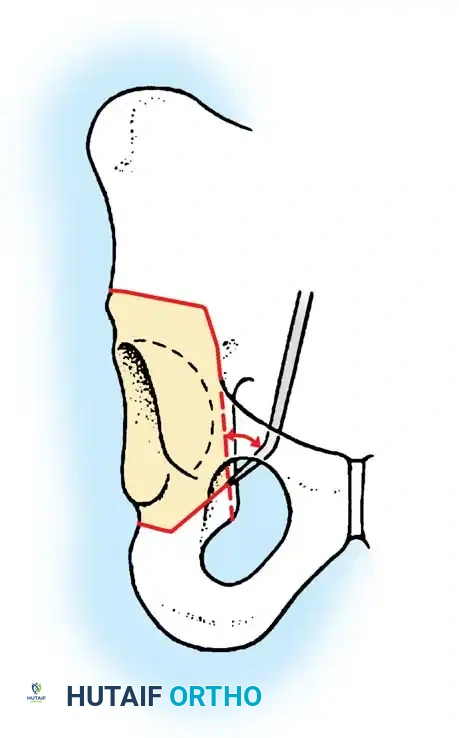
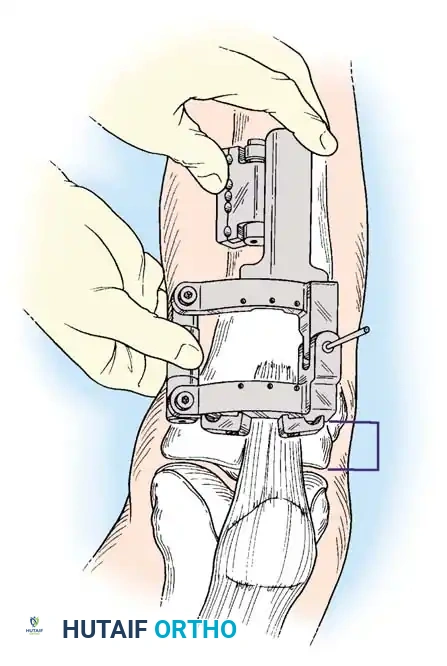
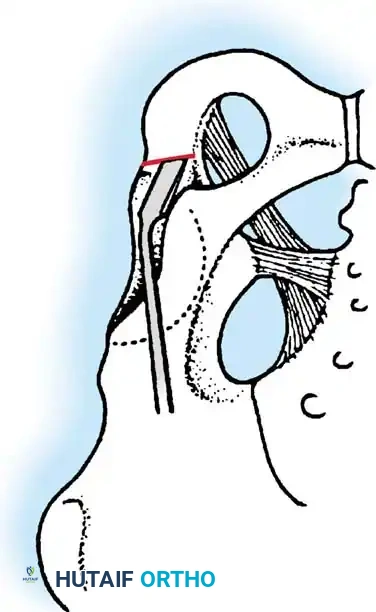
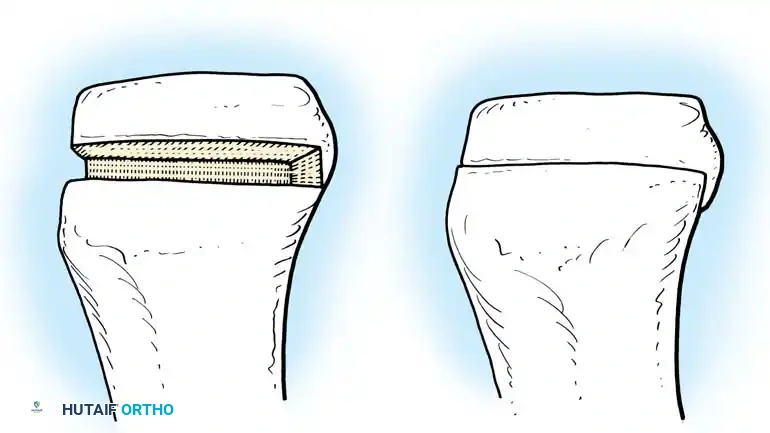
1. Lateral Closing Wedge HTO: Involves removing a laterally based wedge of bone from the proximal tibia and fixing the osteotomy with a plate or staples. It requires a fibular osteotomy or proximal tibiofibular joint disruption.
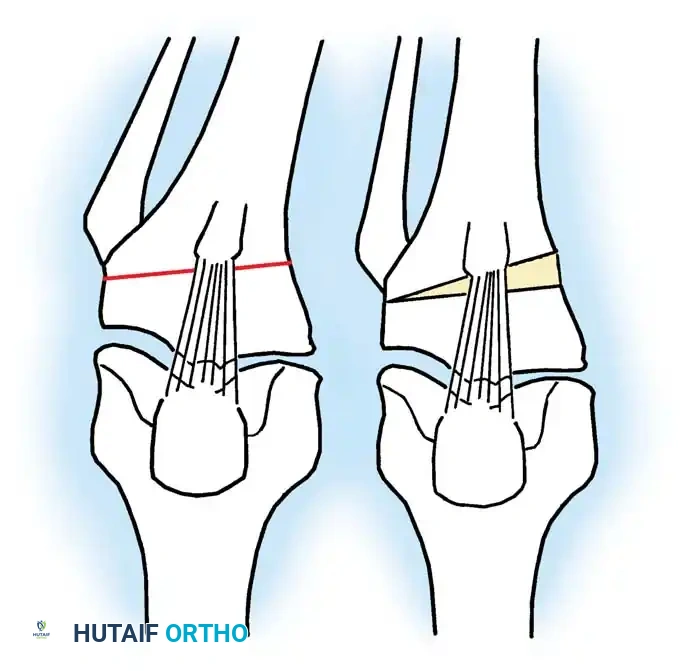
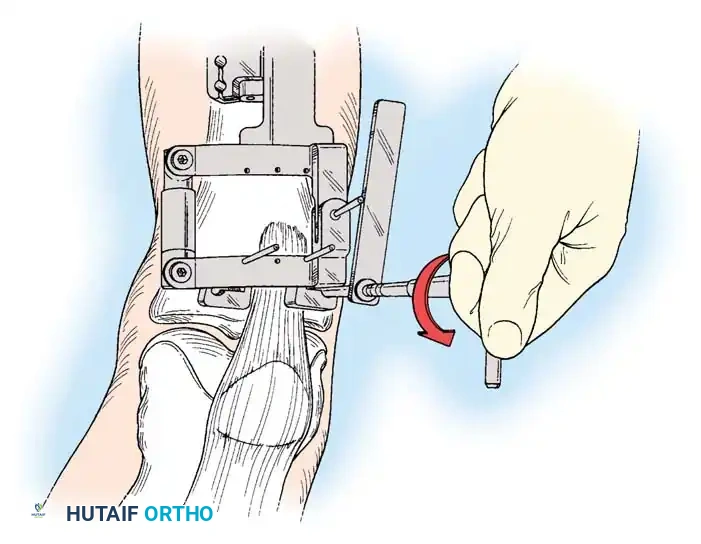
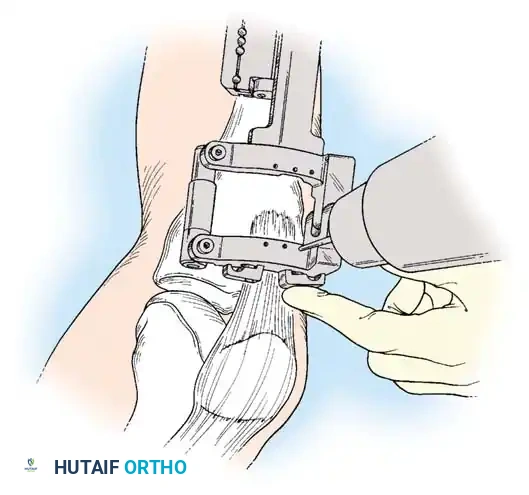
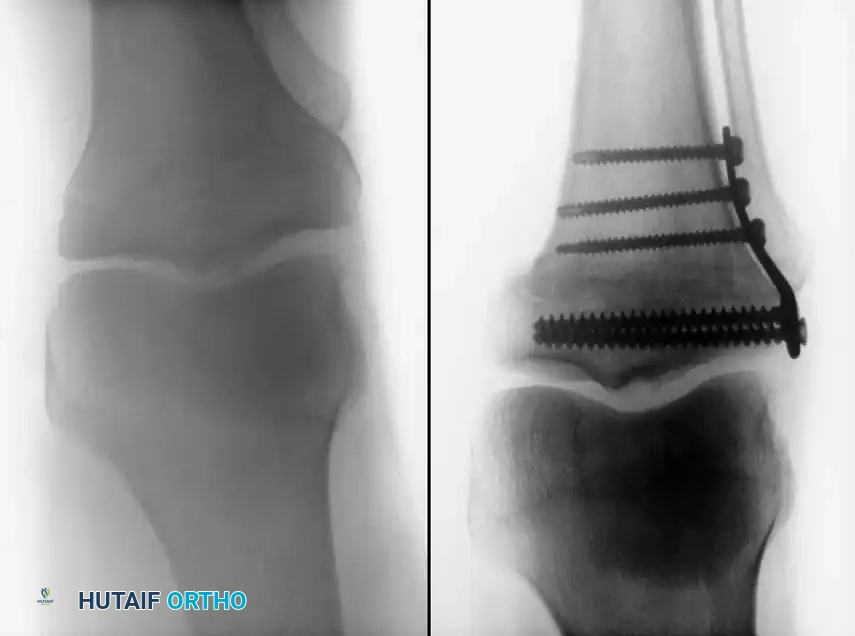
2. Medial Opening Wedge HTO: Increasingly popular due to the avoidance of the peroneal nerve and preservation of bone stock. A medial osteotomy is created, opened to the desired correction angle, and stabilized with a rigid locking plate. The void may be filled with allograft or synthetic bone substitute.
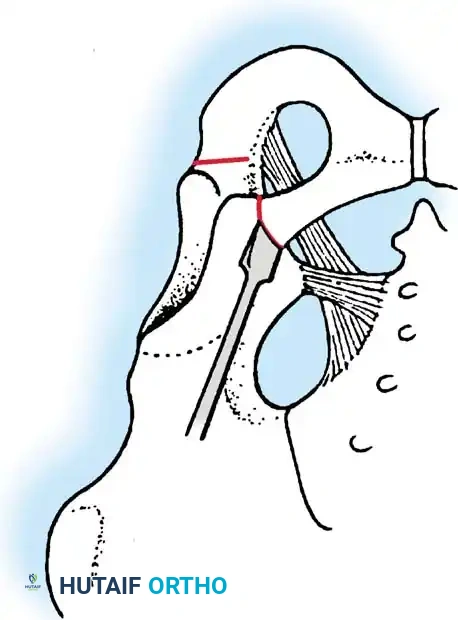
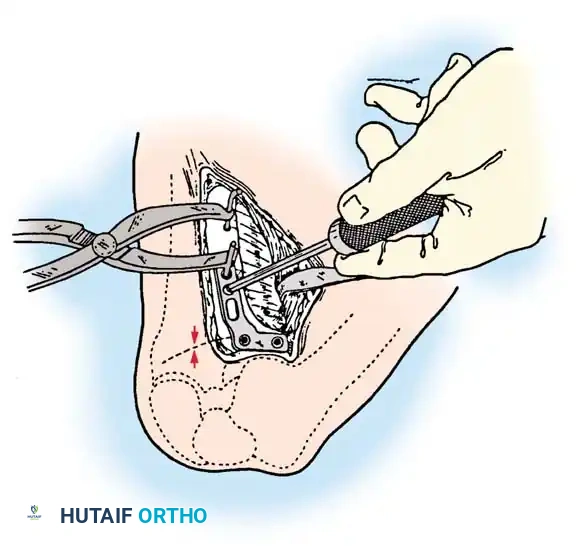
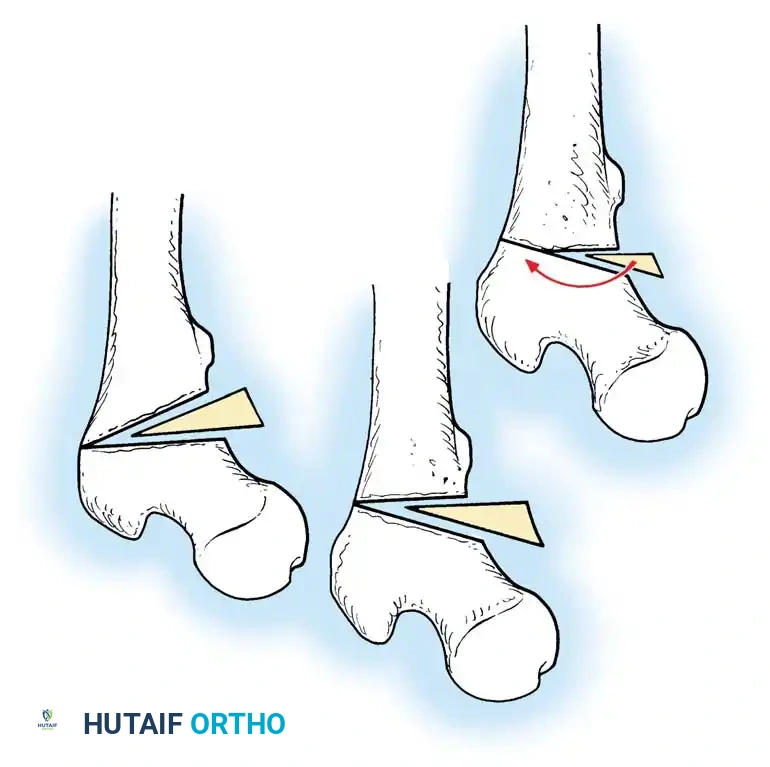
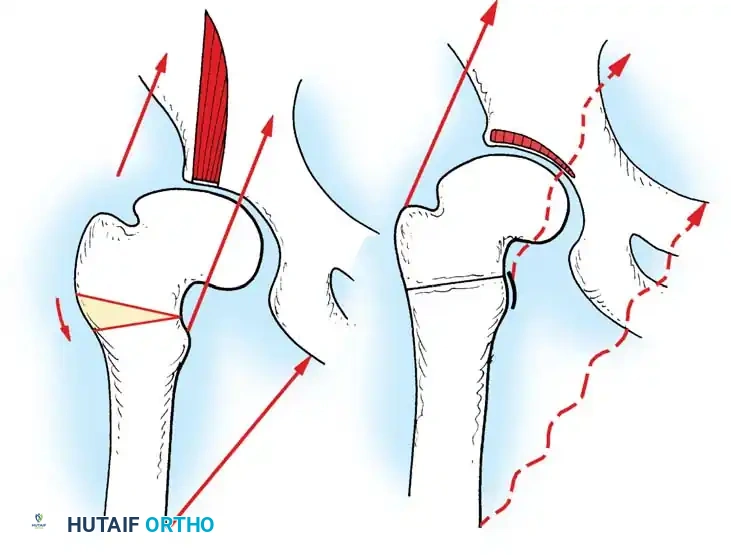
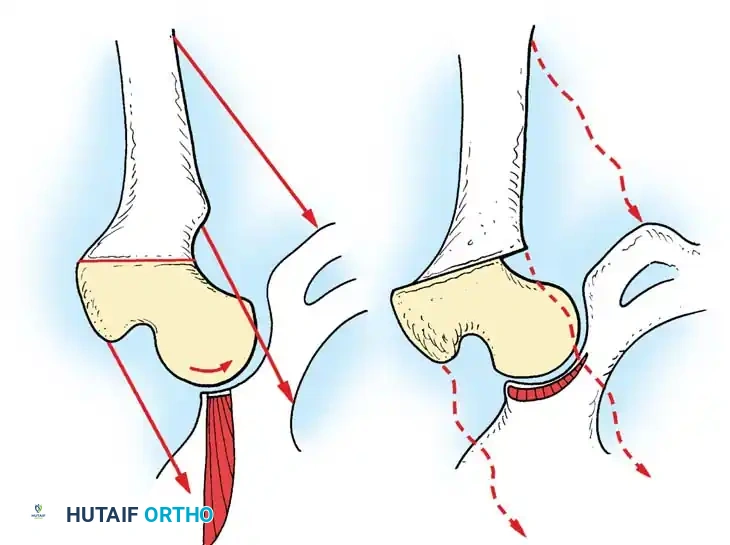
Distal Femoral Osteotomy (DFO)
DFO is indicated for lateral compartment osteoarthritis associated with a valgus deformity. Because the deformity in a valgus knee is typically located in the distal femur rather than the proximal tibia, a medial closing wedge or lateral opening wedge osteotomy of the distal femur is performed.
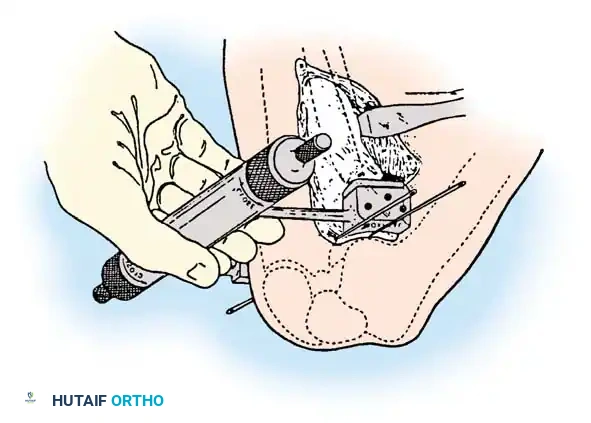
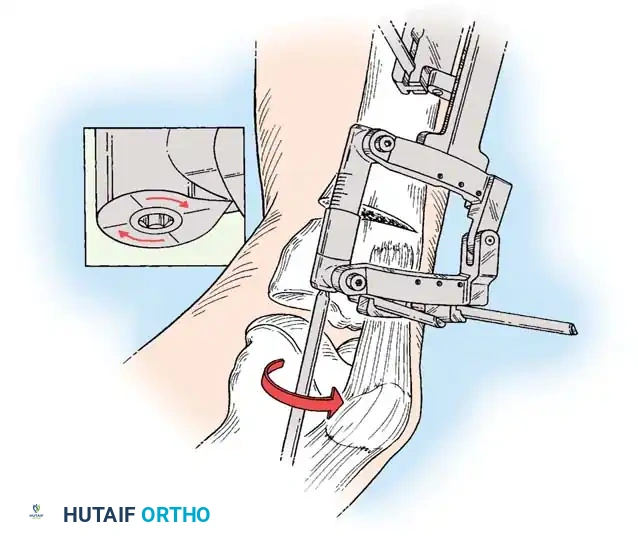
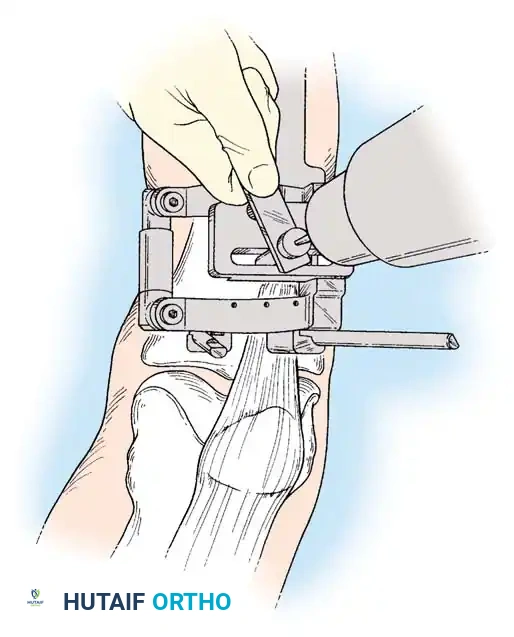
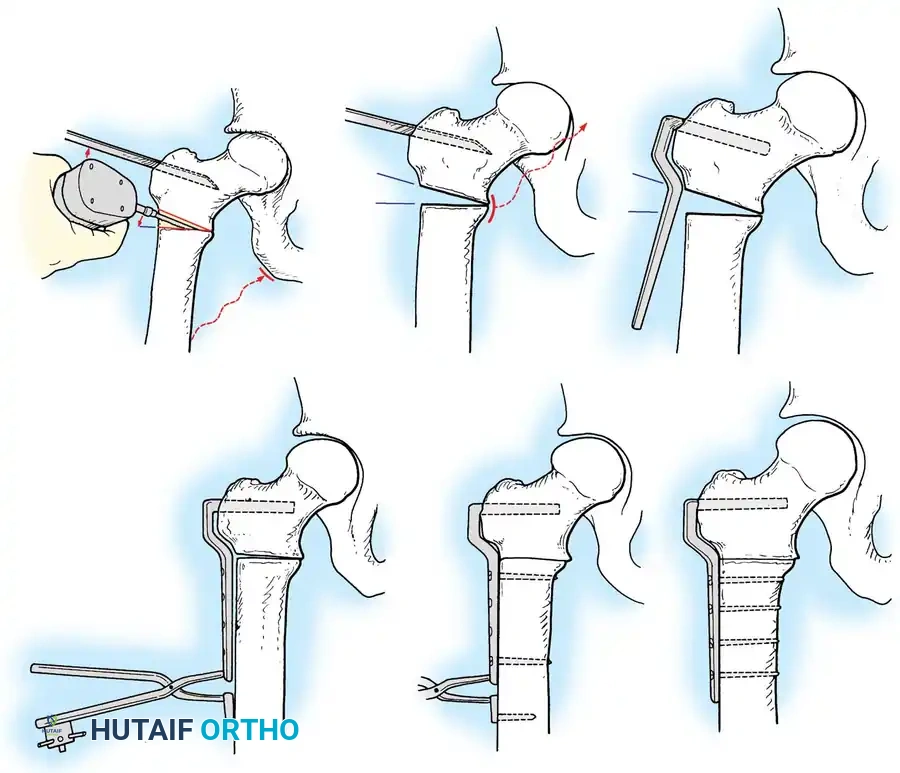
Surgical Atlas: Osteotomy and Realignment Biomechanics
The following radiographic and illustrative figures detail the preoperative planning, biomechanical axes, and intraoperative fixation strategies critical for successful osteotomies around the knee.
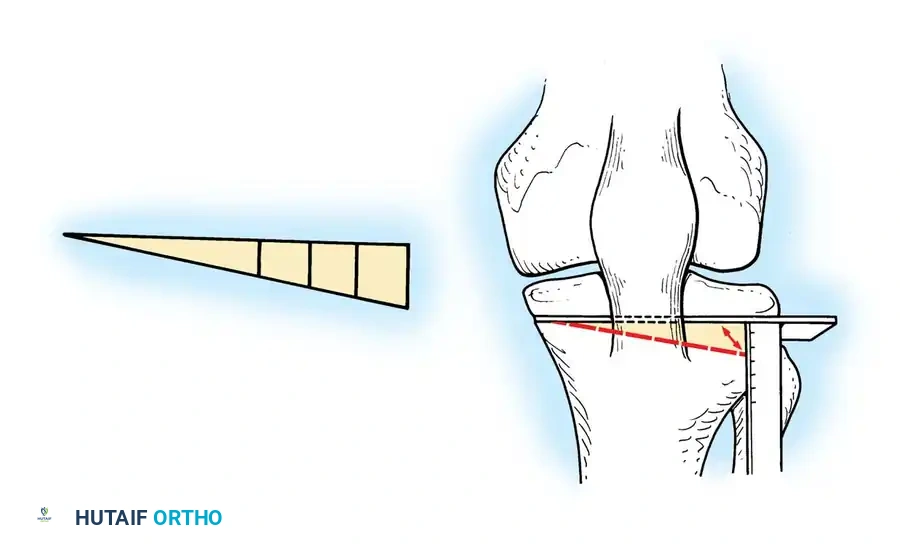
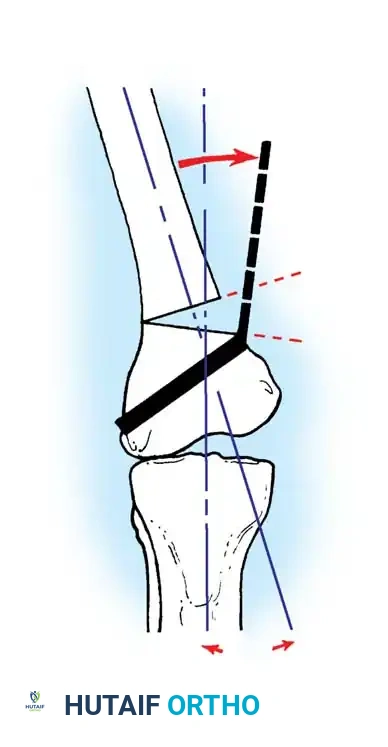
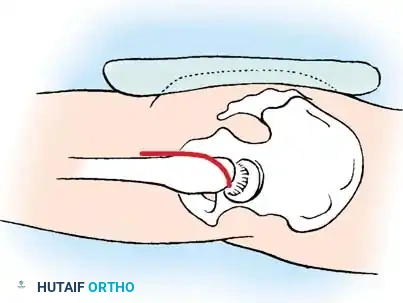
Preoperative templating is mandatory. The mechanical axis must be drawn from the center of the femoral head to the center of the ankle mortise. The degree of correction is calculated to ensure the new weight-bearing line passes through the targeted compartment.
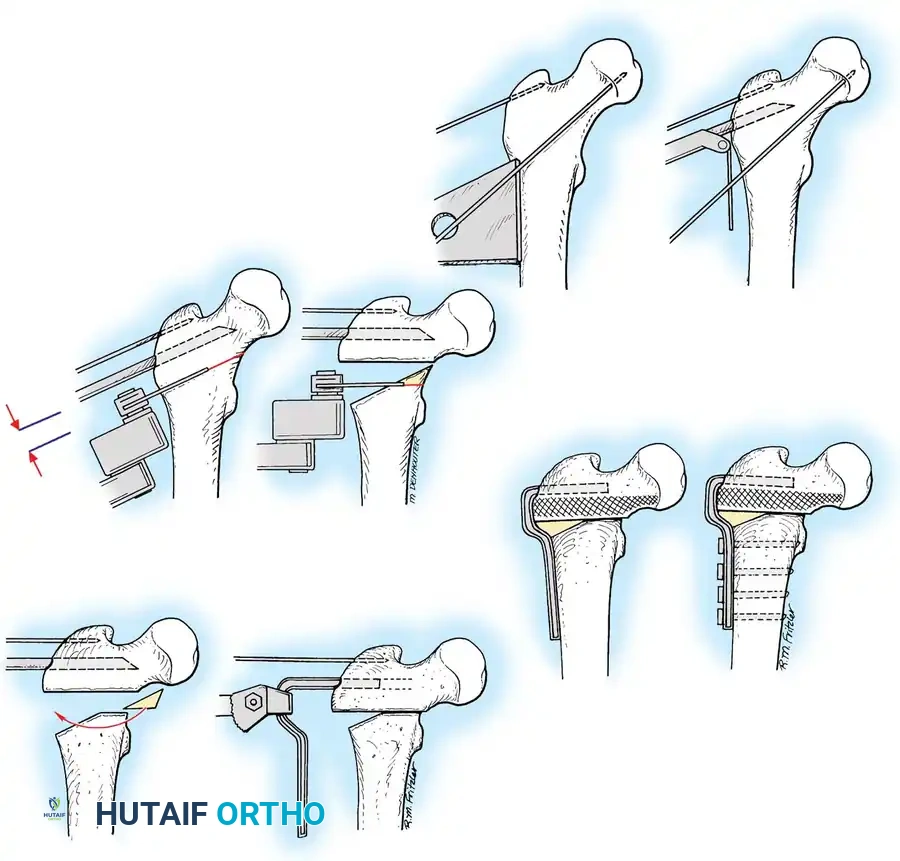
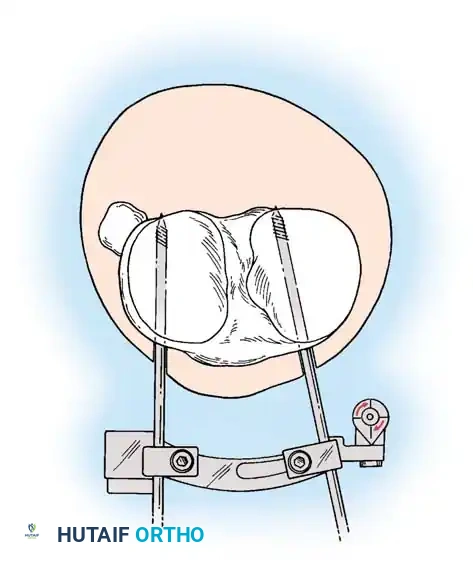
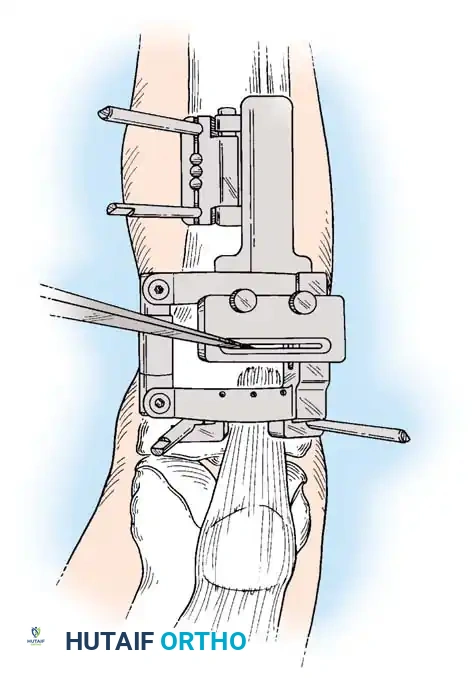
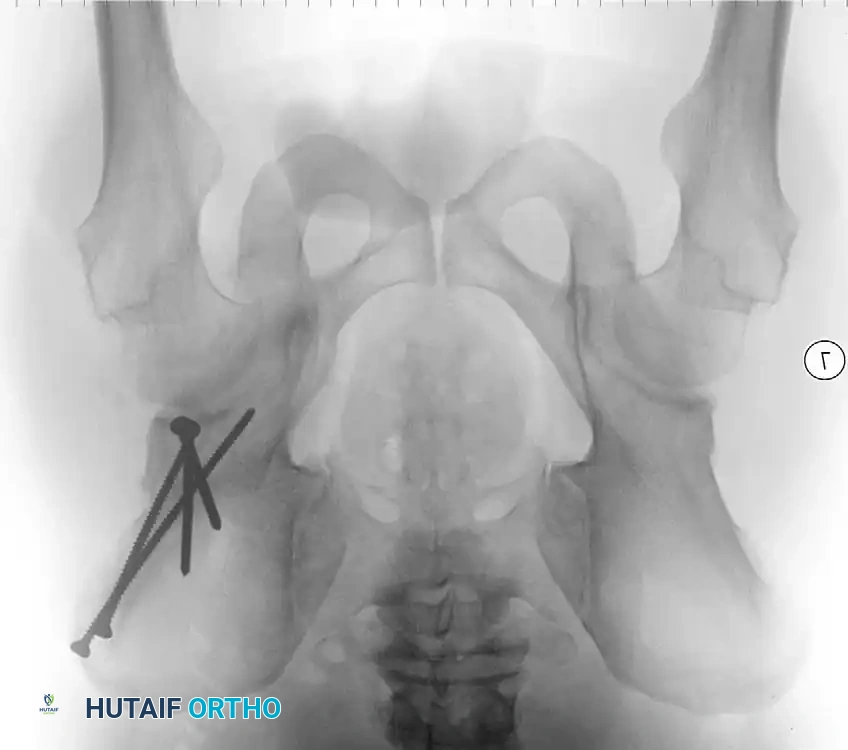
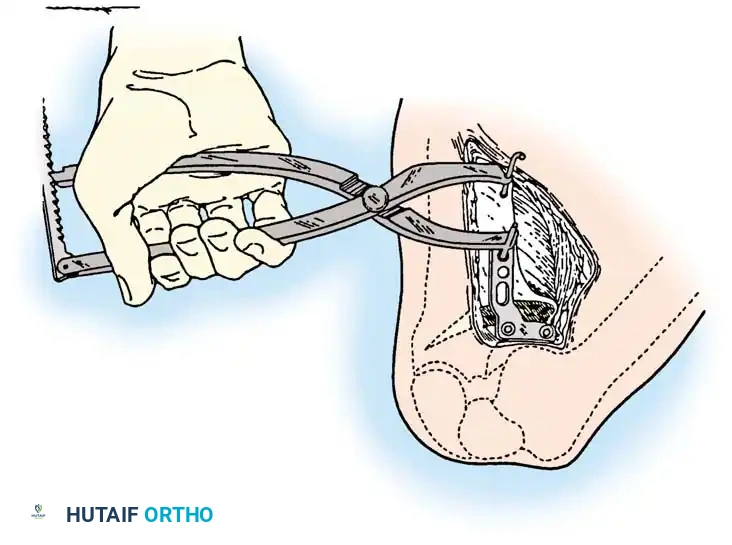
Intraoperative fluoroscopy is utilized to confirm the osteotomy trajectory. Guide pins are placed parallel to the joint line, ensuring the hinge point remains intact to provide intrinsic stability to the osteotomy site.

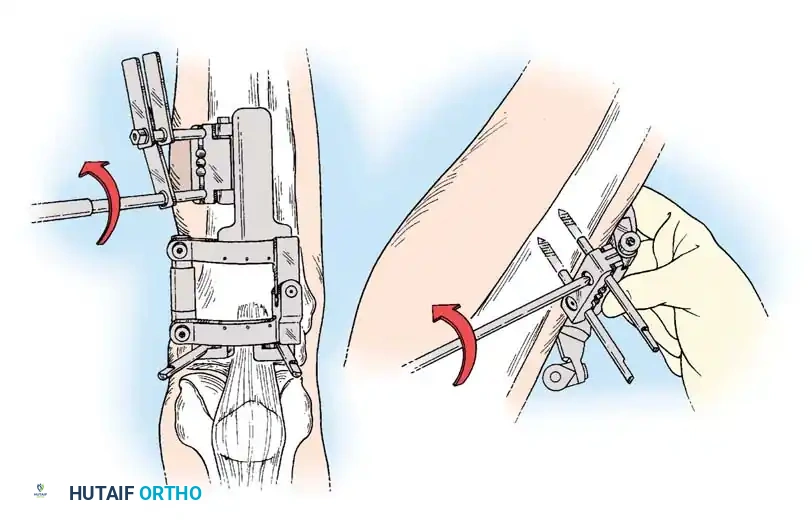
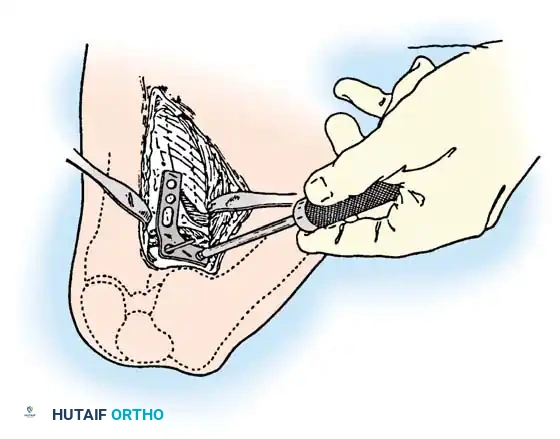
Rigid internal fixation is achieved using anatomically contoured locking plates. In opening wedge osteotomies, the plate acts as a buttress to maintain the correction angle while the osteotomy heals.

Careful soft tissue management is required. In medial opening wedge HTO, the superficial medial collateral ligament (sMCL) must be partially released distally to allow the osteotomy to open without increasing medial compartment contact pressures.
For distal femoral osteotomies, the plate is typically applied to the medial or lateral cortex depending on the wedge orientation. The fixation must be robust enough to withstand the significant bending moments present at the distal femur.

Postoperative rehabilitation following osteotomy involves a period of protected weight-bearing. Early range of motion is encouraged to prevent arthrofibrosis and nourish the articular cartilage.

Complications of osteotomy include delayed union, nonunion, loss of correction, and neurovascular injury. Meticulous surgical technique and adherence to biomechanical principles minimize these risks.
Ultimately, while osteotomy does not cure osteoarthritis, it significantly alters the mechanical environment, providing durable pain relief and delaying the need for total joint arthroplasty in appropriately selected patients.

Conclusion
The operative management of osteoarthritis requires a nuanced understanding of joint biomechanics, patient-specific functional demands,
