Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Prior to transport, the face mask should be removed so that the airway can be easily accessible. If serious injury is suspected, the helmet and shoulder pads should be left in place until he is assessed at the hospital and radiographs are obtained. Leaving the helmet and shoulder pads in place helps to keep the spine in the most neutral alignment. Removal of the helmet will result in extension of the neck, whereas removal of the shoulder pads will most likely result in flexion of the neck. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347. Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med 2001;11:82-86. Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Question 2
The pathophysiology of a claw toe deformity includes muscular imbalance caused by which of the following relatively strong structures?

Explanation
The dynamic forces acting to maintain the position of the proximal phalanx at the head of the metatarsal are a balance between the extensor digitorum longus and the weaker intrinsic muscles. With hyperextension at the metatarsophalangeal joint, the intrinsic muscles become less efficient as plantar flexors. Consequently, the hyperextension deformity progresses in the metatarsophalangeal joint as the opposition of the intrinsic muscles to the extensor tendon lessens. This is in contrast to the situation in the interphalangeal joints, where the stronger flexors overpower the weaker intrinsic muscles, which act as the extensors. This combination of events leads to hyperextension at the metatarsophalangeal joint and flexion deformities at the interphalangeal joints, resulting in claw toe. Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal Joints. J Am Acad Orthop Surg 1995;3:166-173.
Question 3
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?

Explanation
The infant has a well-positioned hip in the Pavlik harness and treatment should be continued in the current position. The success rate is over 90% with the use of this device for a dislocatable hip. Ultrasound is a useful tool to confirm appropriate positioning of the cartilaginous femoral head during treatment. If the femoral head is not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 4
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Explanation
Weil osteotomies are useful in achieving shortening of a lesser metatarsal with preservation of the distal articular surface. The osteotomy is oriented from distal-dorsal to proximal-plantar; therefore, proximal displacement of the distal fragment is associated with plantar (not dorsal) displacement as well. Plantar displacement can result in the intrinsics acting dorsal to the center of the metatarsophalangeal joint and the development of an extended or "floating toe." Nonunion, osteonecrosis, and inadequate shortening are infrequent complications associated with the Weil lesser metatarsal osteotomy. Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 5
Figure 42 is a transverse MRI scan of the left shoulder. The arrow points to which of the following structures?

Explanation
The figure shows an axial image of the shoulder immediately inferior to the coracoid process. The subscapularis tendon, which can be traced from the myotendinous junction, is torn and detached from its lesser tuberosity attachment on the humerus. Lateral to the lesser tuberosity, the bicipital groove is empty. The arrow points to the subluxated biceps tendon. Superficial fibers of the subscapularis tendon are contiguous with the biceps retinaculum, which covers the bicipital groove and hold the biceps tendon in place. The vast majority of subscapularis tendon tears result in disruption of the biceps retinaculum with resultant subluxation of the tendon. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Scientific References
-
:
Question 6
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
A large annular defect at the site of a lumbar disk herniation is associated with persistent radicular pain postoperatively. Large sequestered herniations and a positive SLR preoperatively correlate with good outcomes after diskectomy. Neither symptoms of more than 3 months' duration nor preoperative epidural steroid injections correlate with postoperative results after diskectomy. Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Question 7
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 8
High Yield
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0 degrees of dorsiflexion and 20 degrees of plantar flexion. The patient's knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of

Explanation
The patient has bilateral hypertrophic synovitis that is causing repeated hemarthroses and progressive arthropathy. Ankle synovectomy in patients with hemophilia is effective in significantly reducing the rate of joint bleeding and in slowing the progression of the arthropathy; therefore, bilateral synovectomies is the treatment of choice. Range of motion can be effectively maintained after ankle synovectomy. Bracing and prophylactic transfusions would be ineffective at this time. Ankle arthrodesis should be reserved for patients with severe pain. Compared with patients who have juvenile rheumatoid arthritis, patients with hemophilia generally do not have involvement of the subtalar joint and rarely require a pantalar arthrodesis. Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Question 9
High Yield
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Detailed Explanation
There are no red flags in the history or examination to warrant MRI. Limited bed rest (less than 3 days) has been shown to be more beneficial to early recovery compared with prolonged bed rest (more than 7 days). No data support the use of epidural or facet steroid injections for acute low back pain.
Question 10
A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?

Explanation
When managing a complex intra-articular fracture, it is imperative that there is adequate visualization of the joint; this usually means an extensile approach. At the elbow, this is usually through a transolecranon osteotomy. The recent addition of a muscle-sparing approach as described by Bryan and Morrey has gained popularity, but it is difficult to maintain soft-tissue viability and it may put the ulnar nerve at risk. A triceps-splitting approach, which can be used for simple single articular splits into the joint where extra-articular reduction is available, is possible and good results have been reported. To date, there is minimal data on these alternative approaches for comminuted intra-articular distal humeral fractures. McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522 McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707. Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop 2000;370:19-33.
Question 11
What are the five most common tumors that metastasize to bone?
Explanation
The five most common primary carcinomas that metastasize to bone are breast, prostate, lung, renal, and thyroid in decreasing order of incidence. Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 12
High Yield
When compared with fresh-frozen bone allograft, freeze-dried bone allograft (FDBA) is characterized by
Explanation
The compaction of FDBA is faster than that of fresh-frozen bone. The maximal stiffness reached by both materials when tested was the same (55 MPa), but the FDBA required fewer impactions to achieve that stiffness. Because it is easier to impact, the FDBA may be mechanically more efficient than the fresh-frozen bone in surgical conditions. The brittleness of irradiated FDBA, caused by loss of the capacity to absorb energy in a plastic way, increases the compactness and stiffness of morcellized grafts. The failure rate of fusion in adolescent idiopathic scoliosis has been shown to be much higher in FDBA than in either iliac crest bone graft or composite autograft with demineralized bone matrix. There is a greater erosive surface response to allograft when compared to autograft or frozen allograft, with a larger number of osteoclast and osteoblast nuclei seen microscopically. Cornu O, Libouton X, Naets B, et al: Freeze-dried irradiated bone brittleness improves compactness in an impaction bone grafting model. Acta Orthop Scand 2004;75:309-314. Price CT, Connolly JF, Carantzas AC, et al: Comparison of bone grafts for posterior spinal fusion in adolescent idiopathic scoliosis. Spine 2003;28:793-798.
Question 13
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
Surgical curettage or en bloc resection is the treatment of choice for osteoid osteoma. Night pain and relief of symptoms with nonsteroidal anti-inflammatory drugs are classic findings for osteoid osteoma. Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598. Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Question 14
Figures 19a and 19b show the AP and lateral radiographs of an 18-year-old man who has had knee pain for 3 months. Figure 19c shows a histopathologic photomicrograph of the biopsy specimen. Which of the following factors is most likely to affect his survival?



Explanation
The presence of metastatic disease at diagnosis is the most significant prognostic factor in a patient with osteosarcoma. Limb-sparing surgery, when compared with amputation, is not noted to be associated with any difference in the rate of survival. The presence of a mutated p53 gene has been noted in a minority of patients with osteosarcoma; however, the prognostic importance on an individual basis is unclear. Tumor location and a relative poor response to chemotherapy would be secondary to the presence of metastatic disease in estimating a patient's prognosis. Weis L: Common malignant bone tumors: Osteosarcoma, in Simon MA, Springfield DS (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
Question 15
High Yield
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?
Explanation
Focal calcifications causing small radiopacities are found in 15% to 20% of synovial sarcomas. Their irregular contours differentiate them from the phleboliths found in a benign hemangioma. Ewing's sarcoma, clear cell sarcoma, and malignant fibrous histiocytoma do not commonly have calcifications within the lesions. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 761.
Question 16
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?


Explanation
Muliple neurofibromas result in marked foraminal enlargement as seen on the sagittal MRI scan. Collagen disorders leading to dural ectasia may show similar enlargement, but none of these is listed as a possible answer. Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 17
High Yield
Figure 26 shows the clinical photograph of a patient who has developed a residual limb ulcer following a traumatic transtibial amputation 2 years ago. What is the preferred treatment to resolve the ulcer?

Explanation
The first step in the treatment of an amputation residual limb (stump) ulcer is local wound care and adjustment of the residual limb-prosthetic interface, as well as adjusting prosthetic alignment. Surgical revision should be undertaken only when prosthetic modification is unsuccessful. Murnaghan JJ, Bowker JH: Musculoskeletal complications, in Smith DG, Michael JW, Bowker JH (eds): Atlas of Amputations and Limb Deficiencies, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 683-700.
Scientific References
-
:
Question 18
High Yield
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?
Explanation
Medial clavicle excision alone can be associated with postoperative instability of the clavicle. The clavicle should be stabilized to the first rib by reconstructing the costoclavicular ligament if it is torn or if the resection is lateral to its clavicular insertion. Therefore, care must be taken to resect only that part of the clavicle that is medial to the costoclavicular ligament. Adequate protection for vital structures that lie posterior to the medial end of the clavicle must be provided. Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Question 19
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?


Explanation
The patient has chronic tibial osteomyelitis that is due to low virulent bacteria. The history and studies do not suggest the need for an amputation or a free-flap procedure. This is a localized tibial infection that is in a healed bone; there is no need to resect the entire area of the tibia bone around the infection. The most appropriate treatment is curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics. Studies have shown that in cases of localized osteomyelitis that are of low virulence, as little as 1 week of IV antibiotics followed by 6 weeks of oral antibiotics is successful. Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.
Question 20
The vascularity of the digital flexor tendons is significantly richer in what cross-sectional region?
Explanation
The vascularity of the dorsal portion of the digital flexor tendons is considerably richer than the volar portion. The other regions are not preferentially more vascular. Hunter JM, Scheider LH, Makin EJ (eds): Tendon Surgery in the Hand. St Louis, MO, Mosby, 1987, pp 91-99.
Question 21
High Yield
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of

Explanation
This fracture, known as a pilon fracture, represents comminution of the base of the middle phalanx with both palmar and dorsal cortical disruption. The treatment method that allows the best function and fewest complications is indirect reduction achieved through specific dynamic splinting or the use of specifically designed proximal interphalangeal joint external fixators. Early mobilization can be achieved by either of these techniques. Volar plate arthroplasty is indicated for a simple fracture-dislocation of the proximal interphalangeal joint with comminution of the volar fracture fragment and dorsal dislocation of the remaining articular surface. Open reduction and internal fixation or percutaneous pinning adds surgical risks and scarring and typically will not provide added stability. Cast immobilization will not achieve the goal of early range of motion. Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Question 22
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of

Explanation
The patient's chronic symptoms are associated with a fracture of the base of the hook of the hamate; therefore, the treatment of choice is simple excision of the fracture fragment, with reasonable expectations of functional return. Acute fractures may be difficult to treat because of the high incidence of nonunion, but once nonunion is discovered, nonsurgical management usually is unsuccessful. Bone grafting may be a surgical alternative, but successful outcomes with percutaneous fixation or trephination of the fibrous union have not been reported. Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Question 23
High Yield
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Question 24
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?

Explanation
The presence of drainage 3 weeks after surgery is a sign of wound infection. This infection most likely involves deep tissues until proven otherwise. Oral or IV antibiotics, in the absence of debridement, are not sufficient. Removal of the hardware would lead to rapid progression of the scoliosis in a spine that has been surgically destabilized by removal of the facet joints. The appropriate treatment is debridement with wound culture, IV antibiotics, and retention of hardware. The wound should be closed over drains. Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Question 25
High Yield
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include


Explanation
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 26
High Yield
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 27
What is the most common result if the acetabulum is rotated too far anteriorly during a periacetabular osteotomy?
Explanation
In patients with hip dysplasia who undergo a periacetabular osteotomy, the authors note that the freed acetabular segment can be overcorrected for the deformity. If it is placed too anteriorly, then hip flexion is limited. Posterior dislocation is a rare complication. The other complications should not occur as a result of this procedure. Hussell JG, Rodriguez JA, Ganz R: Technical complications of the Bernese periacetabular osteotomy. Clin Orthop 1999;363:81-92.
Question 28
High Yield
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
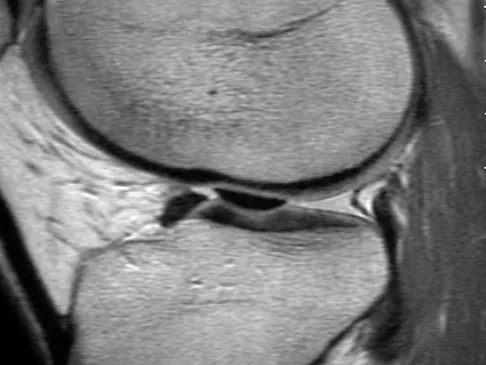
Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 29
High Yield
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
Because there is a significant possibility that the patient may have a fracture of the lateral process of the talus, there is some disagreement as to the best radiographic study to identify this injury. A CT scan is an appropriate diagnostic tool to visualize the fracture and identify any displacement. Displaced lateral process fractures are best treated surgically. Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder's foot and ankle. Am J Sports Med 1998;26:271-277.
Question 30
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?


Explanation
The radiographs show a benign-appearing, well-defined lytic lesion with a thin rim of surrounding reactive bone. The photomicrograph shows spindle cells with a myxoid cartilaginous matrix. These findings are diagnostic of chondromyxoid fibroma. This is a rare, benign tumor that usually causes pain and can be locally aggressive. Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Question 31
The strongest biomechanical construct for open reduction and internal fixation of a talar neck fracture uses what interval and entry point?
Explanation
The strongest biomechanical construct is posterior to anterior fixation with the entry point being at the level of the posterolateral tubercle of the talus. This uses the interval between the peroneus brevis and the flexor hallucis longus. The interval between the flexor digitorum longus and the flexor hallucis longus with entry at the posteromedial tubercle of the talus is not an accepted approach for fixation of talar neck fractures. All of the other options use screw placements from anterior to posterior. Swanson TV, Bray TJ, Homes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
Question 32
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?


Explanation
The radiographs reveal both cement debonding at the lateral shoulder of the prosthesis and a cement mantle fracture. Both of these indicate a loose femoral component. The radiographs show a stress fracture with reactive bone on the lateral femoral cortex in conjunction with the cement mantle fracture. The acetabular component shows no evidence of loosening. Heterotopic bone usually is not a source of pain when it is Brooker grade I, as in this case. Parkinsonism generally is not associated with hip pain. Harris WH, McCarthy JC, O'Neill DA: Femoral component loosening using contemporary techniques of femoral cement fixation. J Bone Joint Surg Am 1982;64:1063-1067. Callaghan JJ, Rosenberg AG, Rubash H (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 960, 1228-1229.
Question 33
High Yield
Figure 11 shows the radiograph of an 18-year-old soccer player who reports recurrent lateral foot pain after sustaining an inversion injury. History reveals that 6 months ago he had been treated in a non-weight-bearing cast for a fifth metatarsal fracture. Management should consist of

Explanation
Fractures in this area of the fifth metatarsal have a high incidence of delayed union, nonunion, and recurrence with nonsurgical management. In an acute fracture, prolonged casting in a non-weight-bearing cast may allow for healing; however, in the presence of prolonged symptoms, recurrent fracture, and intermedullary sclerosis, surgical treatment is preferred. Surgery most commonly consists of intermedullary fixation or medullary curettage and bone grafting, followed by application of a non-weight-bearing cast. Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
Question 34
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?

Explanation
The palmar cutaneous branch of the median nerve separates from the median nerve approximately 4 to 6 cm proximal to the wrist crease and travels between the median nerve and the flexor carpi radialis tendon. It supplies the skin of the thenar region. This nerve is at risk for injury with retraction of the digital flexor tendons in plating the distal radius. Wartenberg's syndrome is compression of the superficial radial nerve which innervates the dorsum of the thumb and the first dorsal web space. Carpal tunnel syndrome causes dysesthesias of the thumb, index, and/or middle fingers. C7 radiculopathy affects the index and middle fingers. Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Question 35
What percent of the adult human meniscus is vascularized?
Explanation
The adult menisci are considered to be relatively avascular structures, with the peripheral blood supply originating predominately from the lateral and medial genicular arteries. Branches of these vessels form the perimeniscal capillary plexus, which supplies the peripheral border throughout its attachment to the joint capsule. Vascular penetration studies have shown that 10% to 30% of the peripheral portion of the medial meniscus and 10% to 25% of the lateral meniscus are vascularized. Arnoczky SP, Warren RF: Microvasculature of the human meniscus. Am J Sports Med 1982;10:90-95.
Question 36
High Yield
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of



Detailed Explanation
Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 37
High Yield
The specificity of intraoperative frozen sections obtained for the evaluation of infected total hip arthroplasty may be improved by
Detailed Explanation
Lonner and associates conducted a prospective study to determine the reliability of analysis of intraoperative frozen sections for the identification of infection during 175 consecutive revision total joint arthroplasties (142 hips and 33 knees). The mean interval between the primary arthroplasty and the revision arthroplasty was 7.3 years (range, 3 months to 23 years). Of the 175 patients, 23 had at least 5 polymorphonuclear leukocytes per high-powered field on analysis of the frozen sections and were considered to have an infection. Of these 23 patients, five had 5 to 9 polymorphonuclear leukocytes per high-powered field and 18 had at least 10 polymorphonuclear leukocytes per high-powered field. The frozen sections for the remaining 152 patients were considered negative. On the basis of cultures of specimens obtained at the time of the revision surgery, 19 of the 175 patients were considered to have an infection. Of the 152 patients who had negative frozen sections, three were considered to have an infection on the basis of the results of the final cultures. Of the 23 patients who had positive frozen sections, 16 were considered to have an infection on the basis of the results of the final cultures; all 16 had frozen sections that showed at least 10 polymorphonuclear leukocytes per high-powered field. The sensitivity and specificity of the frozen sections were similar regardless of whether an index of 5 or 10 polymorphonuclear leukocytes per high-powered field was used. Analysis of the frozen sections had a sensitivity of 84% for both indices, whereas the specificity was 96% when the index was 5 polymorphonuclear leukocytes and 99% when it was 10 polymorphonuclear leukocytes. However, the positive predictive value of the frozen sections increased significantly (P < 0.05), from 70% to 89%, when the index increased from 5 to 10 polymorphonuclear leukocytes per high-powered field. The negative predictive value of the frozen sections was 98% for both indices. At least 10 polymorphonuclear leukocytes per high-powered field was predictive of infection, while 5 to 9 polymorphonuclear leukocytes per high-powered field was not necessarily consistent with infection. Less than 5 polymorphonuclear leukocytes per high-powered field reliably indicated the absence of infection. Feldman DS, Lonner JH, Desai P, Zuckerman JD: The role of intraoperative frozen sections in revision total joint arthroplasty. J Bone Joint Surg Am 1995;77:1807-1813. Lonner JH, Desai P, Dicesare PE, Steiner G, Zuckerman JD: The reliability of analysis of intraoperative frozen sections for identifying active infection during revision hip or knee arthroplasty. J Bone Joint Surg Am 1996;78:1553-1558. Spangehl MJ, Younger AS, Masri BA, Duncan CP: Diagnosis of infection following total hip arthroplasty, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 285-295.
Question 38
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
The majority of large collagen fibers within the menisci are oriented circumferentially. It is these fibers that develop the hoop stress with compressive loading of the menisci. Most meniscal tears are longitudinal and occur between these circumferential fibers. Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
Question 39
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
Breech positioning has been noted as the risk factor that most increases the relative risk of developmental dysplasia of the hip in multiple series and meta-analysis. All the other factors also increase the risk but to a lesser magnitude. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 40
High Yield
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 41
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?

Explanation
The radiograph reveals osteonecrosis of both femoral heads with reasonably maintained joint surfaces. There may be some slight flattening of the femoral heads. Hip arthrodesis is difficult to perform because of the necrotic bone. Its use in patients with osteonecrotic hips is limited because of the 80% bilaterality; therefore, it is not an acceptable alternative. All the other options are acceptable interventions. Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 42
High Yield
What is the most likely consequence of a vertebral compression fracture associated with osteoporosis?
Explanation
After an osteoporotic vertebral compression fracture, the risk of subsequent fractures at adjacent levels increases. This is felt to be the result of a shifting of the sagittal alignment more anteriorly, putting more stress on the osteopenic vertebral bodies and their anterior cortices. Pain generally resolves with rest, but this may take weeks or months. It has been demonstrated experimentally that osteoporotic vertebral bodies are actually less stiff and weaker after a compression fracture; therefore, deformity predisposes to further deformity. The extensor musculature often fatigues over time and usually does not hypertrophy. Frontal plane deformity is a rare development. Heaney RP: The natural history of vertebral osteoporosis: Is low bone mass an epiphenomenon? Bone 1992;13:S23-S26.
Question 43
High Yield
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
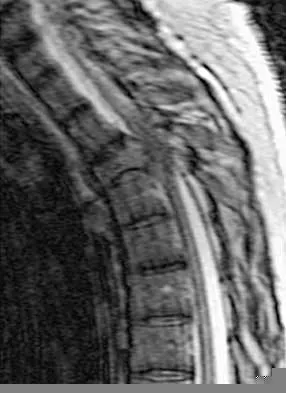
Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Question 44
Which of the following properties apply to the human meniscus when compared with articular cartilage?

Explanation
The meniscal cartilage, like articular cartilage, possesses viscoelastic properties. The extracellular matrix is a biphasic structure composed of a solid phase (collagen, proteoglycan) that acts as a fiber-reinforced porous-permeable composite, and a fluid phase that may be forced through the solid matrix by a hydraulic pressure gradient. Although these properties are shared with articular cartilage, the meniscus is more elastic and less permeable than articular cartilage. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
Question 45
High Yield
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?

Detailed Explanation
The flexor hallucis longus tendon provides the best, most direct route of transfer for filling Achilles tendon gaps. The tendon lies lateral to the neurovascular structures, making it safe for harvest and providing a direct route for transfer into the calcaneus without crossing these important structures. The flexor hallucis longus tendon also has muscle belly that extends distal on the tendon itself, often beyond the actual tibiotalar joint. When the tendon is transferred, this muscle belly brings excellent blood supply to the anterior portion of the reconstruction. Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Question 46
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology?
Explanation
Hypothenar atrophy is a nonspecific sign that can be seen in ulnar neuropathy, C8 radiculopathy, or even cervical myelopathy; however, the atrophy usually is not unilateral and includes other muscle groups. The Spurling test is an excellent method of eliciting cervical radicular pain but involves hyperextension and ipsilateral rotation of the cervical spine, resulting in nerve root compression by reducing the cross-sectional area of the ipsilateral neuroforamen. Tinel's sign at the levator scapulae, if present, is indicative of an upper cervical (C3 or C4) radiculopathy. A subluxable ulnar nerve at the cubital tunnel, while often asymptomatic, points toward cubital tunnel syndrome as an etiology for this patient's pain. The shoulder abduction relief (SAR) sign (relief of upper extremity pain with shoulder abduction) is virtually pathognomic of cervical radiculopathy because this maneuver results in relaxation of a compressed and/or inflamed cervical nerve root. The SAR sign is the converse analog of the straight leg raising sign in the lumbar examination for lumbar radiculopathy, as it relieves tension in the nerve root, thereby relieving symptoms. Ducker TB, Zeidman SM: Neurologic and functional evaluation, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 143-161. An HS: Clinical presentation of discogenic neck pain, radiculopathy, and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Question 47
A 46-year-old woman has bilateral groin pain, with more severe pain on the left side than on the right side. Figures 44a and 44b show a radiograph and a T1-weighted MRI scan. What is the most likely diagnosis?


Explanation
The radiograph reveals bilateral patchy sclerosis of the femoral heads without evidence of collapse. The MRI scan shows bilateral head involvement with a common serpentine-like low-intensity signal of the superior femoral head that is common to osteonecrosis. Changes confined to the femoral head effectively exclude rheumatoid arthritis and osteoarthritis. Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3160-3162.
Question 48
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
Prepubescent athletes gain strength through neurogenic adaptations, including recruitment of motor units, reduced inhibition, and learned motor skills. Myogenic adaptations (muscle hypertrophy) occur after puberty and include increased contractile proteins, thickening of the connective tissue, and increased short-term energy sources such as creatine phosphate. Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Question 49
In the spine, osteoblastomas usually originate in the

Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 50
High Yield
Figure 6 shows the clinical photographs of a newborn who underwent a colostomy for an imperforate anus. Examination shows extended knees, flexed hips, and equinovarus feet. Dimpling is noted over the buttocks. Patients with these findings differ from patients with myelodysplasia in that they

Explanation
The patient has sacral agenesis. Clinical signs include the classic dimpling over the buttocks and the characteristic lower extremity deformities. Imperforate anus is often associated with this disorder. Although motor function correlates with the level of vertebral defect, sensation is usually intact. This is important therapeutically, because patients are not as prone to pressure sores as are those with myelodysplasia. Kyphosis may develop in many patients with lumbosacral agenesis, but lordosis is unusual. Latex allergy and progressive neural deterioration may occur in patients with either myelodysplasia or sacral agenesis but is more common in the former.
Question 51
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
Recent articles have looked at the cyclic load failure and ultimate load failure of biceps tenodesis techniques. The interference screw has proved superior to bone tunnel, suture anchor, and soft-tissue tenodesis techniques in laboratory cadaveric testing. Whether this is clinically relevant or not is still unknown. Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Question 52
A 52-year-old woman reports nagging shoulder pain that has been present for months and is slowly progressive in nature. The patient also reports nocturnal pain and notes that the pain is not activity related. Figures 27a and 27b show the radiograph and bone scan, and Figures 27c through 27e show T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. Based on these findings, what is the most likely diagnosis?





Explanation
The radiograph reveals a metaphyseal lesion with some stippled mineralization suggesting a chondroid tumor. The bone scan shows increased uptake, beyond what is expected for a simple enchondroma, and beyond the limits of the lesion. The MRI sequences shows a lobular lesion on the T1- and T2-weighted (bright on the T2 sequence) images with inhomogeneous uptake of gadolinium; both findings are typical for a chondroid lesion. The history of pain, the positive bone scan, the age of the patient, the size of the lesion, and the central location (enostotic) of the lesion all suggest a malignant cartilage tumor. The images are not consistent with the other diagnoses. In particular, plasmacytoma is more uniformly bright on T2-weighted images and often has a negative bone scan. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 187-194.
Question 53
High Yield
Figures 46a through 46e show the radiographs of a 22-year-old man who injured his wrist in a motorcycle accident. He has no other injuries. What is the best course of action?





Detailed Explanation
The patient has a fracture-dislocation of the radiocarpal joint. Attached to the large radial styloid fragment are the extrinsic wrist ligaments to the carpus. This injury should be treated with open reduction and internal fixation of the styloid fracture. Radiolunate fusion or extrinsic ligament repair is suggested when the extrinsic ligaments are ruptured, resulting in ulnar translocation of the carpus. Dumontier C, Meyer ZU, Reckendorf G, et al: Radiocarpal dislocations: Classification and proposal for treatment: A review of twenty-seven cases. J Bone Joint Surg Am 2001;83:212.
Question 54
High Yield
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with



Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 55
High Yield
A 47-year-old patient has had persistent pain and weakness after undergoing a reamed intramedullary nailing for a midshaft humerus fracture 8 months ago. There is no evidence of infection. Radiographs are shown in Figures 19a and 19b. Management should consist of


Detailed Explanation
Compression plating remains the treatment of choice for most established humeral nonunions. Autograft is felt to be superior to allograft. Electrical stimulation has not been found to improve healing rates in patients with nonunion after intramedullary nailing. Retrograde nailing with flexible nails gives inadequate rotational control to promote healing in this patient. Adding cancellous graft alone will not stabilize the nonunion site. Dynamic locking has been successful only in the lower extremity because the bone can be loaded axially. McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
Question 56
A 32-year-old man notes increasing back pain and progressive paraparesis over the past few weeks. He is febrile, and laboratory studies show a WBC of 12,500/mm3. MRI scans are shown in Figures 6a and 6b. Management should consist of


Explanation
Indications for surgery in spinal infections include progressive destruction despite antibiotic treatment, an abscess requiring drainage, neurologic deficit, need for diagnosis, and/or instability. This patient has a progressive neurologic deficit. Debridement performed at the site of the abscess should effect canal decompression. Once the debridement is complete back to viable bone, the defect can be reconstructed with a strut graft. Additional posterior stabilization is used as deemed necessary by the degree of anterior destruction. CT-guided needle aspiration, while occasionally useful in the earliest phases of an infection, produces frequent false-negative results and would provide little useful information in the management of this patient. Emery SE, Chan DP, Woodward HR: Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 1989;14:284-291. Lifeso RM: Pyogenic spinal sepsis in adults. Spine 1990;15:1265-1271.
Question 57
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
There has been a recent increase in the use of outcome instruments to document and measure effects of treatment of medical conditions, including shoulder disorders. The most important feature of an instrument is whether it actually measures what it purports to measure; this is defined as its validity. Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Question 58
High Yield
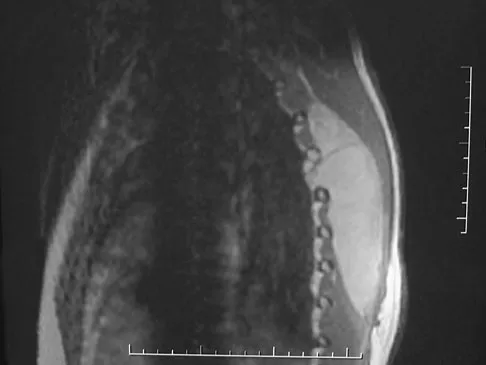
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?

Explanation
The injury shown is a fracture-dislocation and it is highly unstable. In addition to this concern, spinal epidural hematomas have a much higher incidence in people with ankylosing spondylitis following knee fracture. It is felt to be due to disrupted epidural veins, with hypervascular epidural soft tissue in the setting of a rigid spinal canal. Patients with ankylosing spondylitis may have other significant comorbidities, especially cardiac and pulmonary, and these should be carefully assessed. Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004, pp 279-290.
Question 59
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
Sexual dysfunction is a common condition after extensive anterior lumbar surgical dissection. Erectile dysfunction usually is nonorganic but may be related to parasympathetic injury. The parasympathetic nerves are deep in the pelvis at the level of S2-3 and S3-4 and usually are not involved in the surgical field for anterior L4-5 and L5-S1 procedures. Retrograde ejaculation is the result of injury to the sympathetic chain on the anterior surface of the major vessels crossing the L4-5 level and at the L5-S1 interspace. Erectile function and orgasm are not affected by sympathetic injury. The pudendal nerve is primarily a somatic nerve and is not located in the surgical field. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Question 60
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?


Explanation
It is often tempting to assign a diagnosis of plantar fasciitis in patients with hindfoot pain. In this patient, the radiographs confirm a diagnosis of a calcaneal insufficiency fracture. The dense condensation of bone on the lateral view confirms the diagnosis. There is no radiographic evidence of a heel spur, osteochondral lesions, or chondrocalinosis. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 2591. Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Question 61
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
Complications of elbow arthroscopy are usually minor or temporary. However, serious complications include nerve injuries. The deep radial nerve is the closest to any of the portals, resting as close as 1 mm away from the scope inserted in the anterolateral portal. The capsule can be displaced anteriorly by distending the joint with about 25 mL of saline solution, thus moving the deep radial nerve approximately 1 cm anteriorly and decreasing the risk of injuring it while establishing the anterolateral portal. Keeping plastic cannulae in the portals may help to diminish fluid extravasation and swelling, which is more of an impediment than a serious complication. The image intensifier has no documented role in guiding loose body removal. While the proximal anteromedial portal is probably the safest anterior portal to establish, it is actually easier to remove a large loose body from this portal while viewing it from an anterolateral position. There is less tendon and muscle bulk to pass through at the site of the proximal anteromedial portal than at the anterolateral portal, making it less likely for the loose body to get stuck in the soft tissues. Techniques have been developed to permit removal of loose bodies as large as 2 cm in diameter without breaking them up into pieces. If it is possible to remove a large loose body intact, doing so greatly simplifies and shortens the procedure. Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
Question 62
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?

Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 63
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of


Explanation
The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 64
High Yield
Which of the following is a recognized consequence of hip fusion?

Explanation
Low back pain is an expected long-term complication of fusion; ipsilateral knee laxity is frequently encountered, as is degeneration of the contralateral hip. Hip fusion is equally valuable for both men and women, with both genders reporting satisfactory sexual function. Female patients often deliver by elective Cesarean section, although vaginal deliveries are reported. Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Question 65
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 66
High Yield
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include


Explanation
The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting. Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141. Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Question 67
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of

Explanation
The radiograph shows a type V acromioclavicular separation with greater than 100% superior elevation of the clavicle. This finding implies detachment of the deltoid and trapezius from the distal clavicle. Because of severe compromise of function and potential compromise to the overlying skin, surgery is the treatment of choice for type V acromioclavicular separations. During reduction and repair, meticulous repair of the deltotrapezial fascia will also aid in securing the repair. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 68
High Yield
What is the most common complication following arthroscopic capsular release in a patient with adhesive capsulitis of the shoulder?

Explanation
Although all of the above are potential complications after arthroscopic capsular release for adhesive capsulitis, the most common problem is the failure to regain normal glenohumeral motion. An immediate physical therapy program is critical to prevent this complication. Ghalambor N, Warner JJP: Arthroscopic capsular release: Evolution of the technique and its applications. Tech Shoulder Elbow Surg 2000;1:52-60.
Question 69
High Yield
Which of the following statements best describes why the ulnar nerve is most prone to neuropathy at the elbow?

Detailed Explanation
The ulnar nerve is more prone to neuropathy than the radial or median nerves for many reasons. It has the greatest longitudinal excursion required to accommodate elbow range of motion, subjecting it to potential traction forces. The dimensions of the entrance of the cubital tunnel change with elbow motion, potentially causing compression in flexion. For these two reasons, the ulnar nerve is subjected to both compression and traction during elbow motion. Although it passes between two muscle heads as it enters the forearm, so do the median and radial nerves. Finally, the vascular supply is adequate because of the anastamoses between the superior ulnar collateral artery, the posterior ulnar recurrent artery, and the inferior ulnar collateral artery. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 369-378. Prevel CD, Matloub HS, Ye Z, Sanger JR, Yousif NJ: The extrinsic blood supply of the ulnar nerve at the elbow: An anatomic study. J Hand Surg Am 1993;18:433-438.
Question 70
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?




Explanation
The "sunburst" radiographic appearance suggests an osteosarcoma, and the histologic findings confirm the diagnosis with malignant cells surrounded by pink osteoid. MRI scans are not particularly helpful in the diagnosis of osteosarcoma but are mandatory for surgical planning. Osteosarcomas are high-grade sarcomas that are best treated with chemotherapy and wide resection. Even though the peroneal nerve is involved, limb salvage is indicated. Survival after limb salvage is equivalent to amputation, with better function. Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637. Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Question 71
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
The association of a nail puncture wound with a gram-negative infection (Pseudomonas aeruginosa) has been attributed to the local environmental factors in shoes. Osteomyelitis is rare, occurring only in about 1% of patients. Tetanus prophylaxis should be given if it is not up to date. While the remaining organisms listed are periodically involved, they are more common in patients who are immunocompromised or who have diabetes mellitus. Therefore, obtaining a culture of the infected wound is appropriate in such individuals because of the multifactorial nature of the infection. Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Question 72
A 17-year-old girl with Charcot-Marie-Tooth disease reports the development of progressive instability when walking on uneven surfaces. Her involved heel is positioned in varus when viewed from behind. Examination reveals that she walks on the outer border of the involved foot. She has full passive motion of the ankle and hindfoot joints. She is able to dorsiflex the ankle against resistance. The heel varus fully corrects with the Coleman block test. Standing radiographs reveal a cavus deformity with valgus of the forefoot. She would like to avoid using an ankle-foot orthosis. What is the best surgical option?

Explanation
This deformity is early in the disease process. The foot is still flexible, as evidenced by correction with the Coleman block test. A simple dorsiflexion osteotomy of the first metatarsal should provide a plantigrade foot. More complex osteotomies are required later in the disease process when the foot is not flexible and the deformity does not correct with the Coleman block test. The patient may also require a tibialis anterior transfer later in the disease process but not at the present time. Richardson EG (ed): Orthopaedic Knowledge Upate: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-144.
Question 73
Figure 24 shows the sitting AP and lateral spinal radiographs of a nonambulatory 12½-year-old boy with Duchenne muscular dystrophy who is being evaluated for scoliosis. The lumbar curve from T12 to L5 measures 36 degrees, and the thoracic curve from T3 to T12 measures 24 degrees on the AP radiograph. He has 5 degrees of pelvic obliquity. His forced vital capacity is 45% of predicted for height and weight. What is the most appropriate treatment for the spinal deformity?

Explanation
Posterior spinal fusion is the treatment of choice for scoliosis in patients with Duchenne muscular dystrophy once they are no longer able to walk. This treatment improves quality of life and upright wheelchair positioning. Its effect on pulmonary function is less clear, as pulmonary function will continue to decline because of the underlying muscle disease. While bracing and wheelchair modifications may slow the progression of the curve, progression will continue. Surgical intervention at this stage does not have to include the pelvis, which, in general, is indicated in curves of greater than 40 degrees, and when pelvic obliquity is greater than 10 degrees. Fixation to the pelvis should also be considered in lumbar curves where the apex is lower than L1. Surgical treatment usually can be safely performed if the vital capacity is greater than 35%. Hahn GV, Mubarak SJ: Muscular dystrophy, in Weinstein SL (ed): The Pediatric Spine, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 819-832.
Question 74
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 75
An 8-year-old girl has had a painless enlarging mass of insidious onset in the left thigh for the past 3 weeks. Her mother denies any history of trauma, fever, or disease. Examination reveals a nontender, mobile mass in the left medial thigh. Her gait is normal. Figures 25a through 25d show the frog-lateral radiograph, the axial and coronal T1-weighted MRI scans, and the axial T2-weighted MRI scan. Biopsy results reveal a nonrhabdomyosarcoma soft-tissue sarcoma. The most appropriate treatment should consist of




Explanation
In childhood, the more common soft-tissue sarcomas are rhabdomyosarcoma, synovial sarcoma, and fibrosarcoma. Rhabdomyosarcoma, treated with radiation therapy and chemotherapy, is a round cell tumor and is inconsistent with this patient's histologic findings. Synovial sarcoma can be monophasic or biphasic with both spindle and epithelial-like cells and is associated with the characteristic reciprocal chromosomal translocation of t(x:18)(p11;q11) which is not found in fibrosarcoma. Synovial sarcoma also can be associated with cystic loculated areas best seen in a T2-weighted MRI scan. Nonrhabdomyosarcoma childhood soft-tissue sarcomas are treated with surgical excision in conjunction with chemotherapy and/or radiation therapy. The histology reveals no inflammatory cells to suggest an abscess; therefore, antibiotics and drainage are unnecessary. The MRI scans clearly show a mass of soft tissue and no bone involvement; therefore, proximal femoral resection is not appropriate. Serial observation is not appropriate because of the history of enlargement and insidious onset. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, p 757.
Question 76
A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment?


Explanation
The patient is a young laborer with osteoarthritis. Initial treatment should begin with nonsurgical management that may include anti-inflammatory drugs, cortisone injections, and physical therapy to diminish pain and improve motion. The other choices may eventually be necessary but should only follow a course of nonsurgical management. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Question 77
High Yield
Figures 36a and 36b show the radiographs of a 3-year old child who has a congenital upper extremity deformity. Which of the following features would be a major contraindication to a centralization procedure?


Explanation
The patient has bilateral absent radii or radial clubhand. Patients who lack elbow flexion take advantage of the hand position to reach their mouths, and a centralization procedure would take away that ability. This procedure can be performed on patients with partial to complete absence of the radius. A hypoplastic thumb can be addressed at a staged procedure; it does not represent a contraindication to centralization. Complete thumb absence can be addressed by pollicizing the index ray. Green DP: Operative Hand Surgery, ed 2. New York, NY, Churchill Livingstone, 1988, pp 269-271.
Question 78
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?


Explanation
The radiograph and pathology are consistent with adamantinoma. While the mechanism underlying adamantinoma has not been identified, it is believed to be closely related to osteofibrous dysplasia, which may represent a precursor. The other diagnoses are not known to give rise to adamantinoma.
Question 79
High Yield
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?

Explanation
Whenever a patient's condition changes following a test or a procedure, the physician must determine the cause. A steroid flare reaction will not cause incontinence or weakness of the lower extremities. An L4-5 diskectomy may alleviate the problem if the right-sided L4-5 disk herniation is the etiology of the symptoms. However, it is unlikely that a right-sided disk herniation alone will cause a cauda equina syndrome. Possible etiologies include a further extrusion of a disk fragment at L4-5 that now obliterates the spinal canal, a disk herniation at another level, or an epidural abscess following injection of corticosteroids through a caudal approach. In the presence of a possible infection, myelography should not be performed from a lumbar puncture. The fastest and least invasive way to make an appropriate diagnosis is to obtain an MRI of the lumbar spine. In this patient, the MRI revealed an epidural abscess that was compressing the cauda equina. Because of the large dose of steroids that were injected, the patient did not manifest symptoms such as fevers and chills until late in the course. Knight JW, Cordingley JJ, Palazzo MG: Epidural abscess following epidural steroid and local anaesthetic injection. Anaesthesia 1997;52:576-578.
Question 80
High Yield
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of

Explanation
If the patient's medical condition and prognosis remain good in the presence of significant and progressive neurologic deficit from cord compression, then the most reliable means of restoring function is via surgical decompression and fusion. Decompression should be directed toward the compressing structure (eg, anteriorly if the compression is from the anterior side). This procedure can be done via a posterolateral technique, such as costotransversectomy in some cases.
Question 81
Figure 16 shows the clinical photograph of a 3-month-old infant with a foot deformity that has been nonprogressive since birth. Examination reveals that the deformity corrects actively and with passive manipulation. There is no associated equinus. Management should consist of

Explanation
The patient has bilateral metatarsus adductus deformities. In a long-term follow-up study by Farsetti and associates, deformities that were passively correctable spontaneously resolved and no treatment was required. More rigid deformities were successfully treated with serial manipulation, with good results in 90%. There were no poor results. Therefore, observation is the management of choice for passively correctable deformities. In feet that are more rigid, serial manipulation and casting is the management of choice.
Question 82
High Yield
Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis of this bony lesion?


Detailed Explanation
The radiographs reveal a geographic lesion of the proximal femur with the classic "ground glass" appearance noted in fibrous dysplasia. This intramedullary lesion is modestly expansile, demonstrates some minimal cortical thinning, and has no aggressive features. Chondroblastoma, giant cell tumor, and osteoblastoma are more lytic in appearance, and the location is not typical for giant cell tumor or chondroblastoma. While enchondroma may be considered, the uniform ground glass appearance, lack of punctuate mineralization, and distinct margination of the lesion make that diagnosis less likely.
Question 83
High Yield
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?
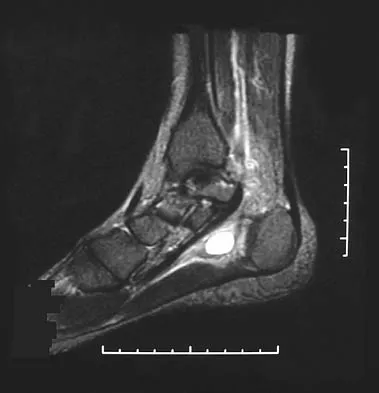
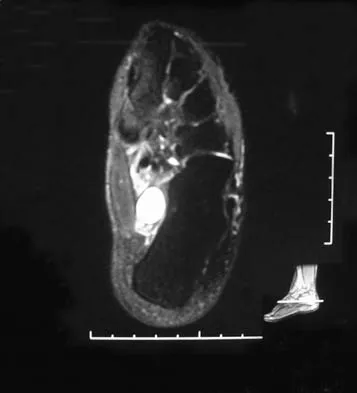
Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 84
High Yield
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 85
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
Neurologic injury after shoulder replacement is relatively uncommon, occurring in 4% of shoulders in one large series. The importance of identifying and protecting the musculocutaneous and axillary nerves cannot be overemphasized; it is especially critical during revision arthroplasty when the normal anatomic relationships have been distorted. The long deltopectoral approach leaving the deltoid attached to the clavicle was found to be significant in the development of postoperative neurologic complications. A correlation was found between surgical time and postoperative neurologic complications, with long surgical times being associated with more neurologic complications. The presumed mechanism of injury is traction on the plexus that occurs during the surgery. A neurologic injury after total shoulder arthroplasty usually does not interfere with the long-term outcome of the arthroplasty itself; it is best managed by protective measures with passive range of motion of the involved extremity. Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 86
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Explanation
Absence of the rotator cuff results in superior migration of the humeral head because of unopposed deltoid function. This proximal migration results in eccentric loading of glenoid components with early loosening. Hemiarthroplasty yields good pain relief with limited goals of active elevation of 90 degrees. The coracoacromial arch should be preserved. Achieving satisfactory subscapularis tension is preferred to the use of an oversized humeral component. Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348. Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491. Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Question 87
Which of the following is considered an important factor in improved cemented femoral stem survivorship?
Explanation
Cement technique, relative stem to canal size and position, stem design, surgical technique, and femoral anatomy are important factors in cemented stem survivorship. Varus stem position, a wide diaphyseal to metaphyseal ratio (stovepipe femur), thin cement mantles (1 mm or less), and nonrounded femoral stem designs are negative prognostic factors for stem survivorship. Precoating with methylmethacrylate has not been shown to provide any increased survivorship over nonprecoated stems. Noble PC, Collier MB, Maltry JA, Kamaric E, Tullos HS: Pressurization and centalization enhance the quality and reproducibility of cement mantles. Clin Orthop 1998;355:77-89. Crowninshield RD, Brand RA, Johnston RC, Milroy JC: The effect of femoral stem cross-sectional geometry on cement stresses in total hip reconstruction. Clin Orthop 1980;146:71-77.
Question 88
High Yield
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?

Explanation
Varus position of the stem is most commonly associated with failure of the cemented femoral component because of association with an inadequate cement mantle in the proximal medial and distal lateral zones. An inadequate cement mantle and obesity have been associated with increased loosening but not as frequently as a varus deformity. The influences of gender and osteoporotic bone on the outcome of cemented femoral components have not been established. Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Question 89
Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of


Explanation
Treatment of congenital pseudarthrosis of the tibia is problematic. To achieve union, a resection of the pseudarthrosis, stabilization, and bone grafting must be performed. Simple cast immobilization does not yield union. There are various options for the resection, immobilization, and grafting. On the first surgical attempt, retrograde intramedullary nailing offers the best chance for success by transfixing the ankle and subtalar joints with abundant autogenous bone grafting. Distraction osteogenesis and vascularized free fibular graft are reserved as salvage procedures. Gilbert A, Brockman R: Congenital pseudarthrosis of the tibia: Long-term follow-up of 29 cases treated by microvascular bone transfer. Clin Orthop 1995;314:37-44. Boero S, Catagni M, Donzelli O, Facchini R, Frediani PV: Congenital pseudarthrosis of the tibia associated with neurofibromatosis - 1: Treatment with Ilizarov's device. J Pediatr Orthop 1997;17:675-684.
Question 90
The parents of a 13-year-old boy with Down syndrome report that he has an increasing limp and decreased endurance with activities. Lateral flexion-extension radiographs of the cervical spine show no evidence of instability. Examination reveals a right Trendelenburg limp and an obvious limb-length discrepancy. Hip motion is symmetric except for some decreased abduction on the right side. A standing AP radiograph is shown in Figure 20. Management should consist of

Explanation
Ligamentous laxity and muscle hypotonia seen in Down syndrome contribute to the incidence of hip subluxation and dislocation. These factors can be progressive and lead to degenerative arthritis in adults with Down syndrome. Because this patient has a progressive limp and decreased endurance, observation and a shoe lift are not options. Bracing may be an option in the younger child before significant bony changes occur. Surgical intervention is the treatment of choice in this patient; however, all components of the deformity need to be addressed. Because of the increased capsular laxity, there is a high likelihood of recurrence if capsulorrhaphy is not included with the pelvic and femoral osteotomies. Surgery in these patients is associated with a high rate of complications. Shaw ED, Beals RK: The hip joint in Down's syndrome: A study of its structure and associated disease. Clin Orthop 1992;278:101-107. Aprin H, Zinc WP, Hall JE: Management of dislocation of the hip in Down's syndrome. J Pediatr Orthop 1985;5:428-431.
Question 91
High Yield
A 17-year-old boy underwent open reduction and internal fixation of a navicular fracture 5 days ago. A follow-up examination now reveals a tensely swollen foot with erythema and multiple skin bullae. The patient is febrile and has marked pain with palpation of the entire forefoot and hindfoot. What is the next step in management?
Detailed Explanation
Necrotizing fasciitis is a rapidly progressive soft-tissue infection with the potential to threaten both life and limb. Patients who are immunocompromised (HIV infection, diabetes mellitus, alcohol abuse) are at increased risk. However, any patient in the immediate postoperative phase is susceptible to wound infection. Early detection is the key. Necrotizing fasciitis is primarily a surgical problem that requires urgent debridement and broad-spectrum IV antibiotics. Rapid diagnosis and prompt treatment help to reduce mortality, which may approach 30%. Debridement of the bullae and observation are not indicated. Although elevation and close follow-up may be warranted early on, in this patient, surgical debridement is the next step. Ault MJ, Geiderman J, Sokolov R: Rapid identification of group A streptococcus as the cause of necrotizing fasciitis. Ann Emerg Med 1996;28:227-230.
Question 92
High Yield
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of


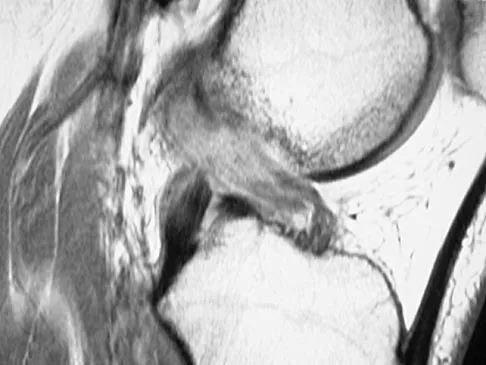
Explanation
The injury mechanism involves a valgus load applied to the knee with the foot in external rotation. The primary stabilizer to valgus laxity is the medial collateral ligament. The secondary restraints to valgus rotation are the cruciate ligaments. Examination indicates disruption of the medial collateral and anterior cruciate ligaments. Valgus opening in extension should also arouse suspicion for an injury to the posterior cruciate ligament; however, in this patient, the valgus opening in extension is mild. The slight opening in extension and the increased anterior drawer, especially with external rotation, indicates disruption of the posteromedial capsule and posterior oblique ligament. Figure 21a shows complete disruption of the superficial and deep medial collateral ligaments involving the meniscofemoral ligament. Figure 21b shows a more posterior coronal section with a torn posterior oblique ligament. Figure 21c shows disruption of the anterior cruciate ligament, while the posterior cruciate ligament at the tibial insertion appears with a homogenous normal signal. Warren LA, Marshall JL, Girgis F: The prime static stabilizer of the medial side of the knee. J Bone Joint Surg Am 1974;56:665-674.
Question 93
High Yield
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0 degrees F (35 degrees C). What is the recommended treatment of the femoral fracture at this time?
Detailed Explanation
This is a "borderline trauma" patient where serious consideration for damage control orthopaedic surgery is required. His prolonged hypotension, abdominal injury, and chest injury put him at higher risk for serious postinjury complications. Further surgery, such as definitive fracture fixation, adds metabolic load and injury to his system. It is prudent to consider femoral fracture stabilization with an external fixator until he is physiologically recovered as evidenced by a normal base excess and/or lactate acid levels, as well as all other parameters of resuscitation. A borderline patient has been described as polytrauma with an ISS > 20 and thoracic trauma (AIS > 2); polytrauma and abdominal/pelvic trauma (Moore > 3) and hemodynamic shock (initial BP < 90 mm Hg); ISS > 40; bilateral lung contusions on radiographs; initial mean pulmonary arterial pressure > 24 mm Hg; pulmonary artery pressure increase during intramedullary nailing > 6 mm Hg. Factors that worsen the situation following surgery include multiple long bones and truncal injury (AIS > 2), estimated surgery time of more than 6 hours, arterial injury and hemodynamic instability, and exaggerated inflammatory response (eg, Il-6 > 800 pg/mL). It is incumbent on the orthopaedic surgeon who is a member of the trauma team to make sure that he or she is aware of these factors and guides the team to the best patient care. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Question 94
High Yield
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?

Detailed Explanation
The patient has a grade 4 spondylolisthesis. Optimal surgical management is posterior spinal fusion from L4 to the sacrum. The use of instrumentation is controversial. Vertebrectomy is typically reserved for spondylo-optosis (grade 5) cases. Spinal fusion from L5 to S1 usually is not successful for a slip that is greater than 50%. Isolated anterior spinal fusion has not been successful, and direct repair of the pars defect is only useful for spondylolysis without spondylolisthesis. Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 2003;52:525-532.
Question 95
High Yield
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?

Detailed Explanation
A compression or burst injury occurs with vertical loading of the spine, such as from a blow to the vertex with the neck flexed (eg, spear tackling in football). This leads to vertebral end plate fractures before disk injury. At higher forces, the entire vertebra and disk may explode into the spinal canal. Analysis has shown this to be the major mechanism of cervical fracture, dislocation, and quadriplegia. With the normal head-up posture, the cervical spine has a gentle lordotic curve, and forces transmitted to the head are largely dissipated in the cervical muscles. When the neck is flexed, the cervical spine becomes straight, with the vertebral bodies lined up under one another. This allows for minimal dissipation of the impact forces to be absorbed by the neck muscles. Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532. Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Question 96
High Yield
A 67-year-old man is requesting revision surgery because of continued pain in the knee after undergoing a total knee replacement 2 years ago. Examination reveals that the knee is not warm, the incision is well-healed, and the skin has normal coloration and hair formation. No varus or valgus instability is noted, and knee range of motion is 5 degrees to 100 degrees. Laboratory studies show an erythrocyte sedimentation rate of 15 mm/h and a WBC of 5,000/mm3. Aspiration of the knee reveals clear fluid that shows no growth on culture. Radiographs reveal an appropriately positioned cruciate-retaining cemented total knee arthroplasty that is well-fixed. What is the probability that the patient's pain will be improved with revision surgery?

Detailed Explanation
The patient has a well-fixed and aligned painful total knee replacement. The success rate of revision knee replacement for pain when no mechanical problem can be identified is approximately 40%. The critical step is to rule out the presence of infection with appropriate laboratory studies and aspiration. If no infection is detected, revision should be avoided. Rand JA: Planning for revision total knee arthroplasty, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 161-166.
Question 97
Figure 27 shows the AP radiograph of a patient who has late instability. The problem most likely occurred as a result of

Explanation
Although dislocation can occur anytime after hip arthroplasty, the highest incidence is observed within the first few months. Dislocation occurring many years after arthroplasty has also been described. In contrast to early dislocation, it appears that late dislocation frequently requires surgical intervention. Recent studies suggest that the incidence of late dislocation may be greater than initially appreciated and that the cumulative rate of dislocation rises with increasing follow-up. The presumed etiologic factors for late instability include long-standing problems with the prosthesis (such as malpositioning of the components) with late manifestation, trauma, deterioration in the neurologic status of the patient, and polyethylene wear. The eccentric position of the femoral head in this patient confirms polyethylene wear. The femoral stem is well-fixed, and the greater trochanter osteotomy has united well. The minor osteolysis observed around the proximal femur is also the consequence of wear and is not the cause of instability. Infection, without component loosening and massive soft-tissue destruction, is not otherwise known to result in late instability. Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14.
Question 98
High Yield
When converting the knee shown in Figure 20 to a total knee arthroplasty, satisfactory outcome can be expected in what percent of patients?

Detailed Explanation
Naranja and associates reviewed 37 knees (35 patients, with 28 women and 7 men) without any motion that were converted to total knee arthroplasties. After an average follow-up of 90 months, the patients lacked an average of 7 degrees of extension and had 62 degrees of flexion. Results showed a short-term complication rate of 24% (stiffness requiring manipulation, delayed wound healing, and recurrent hemarthrosis), a major complication rate of 35% (patellar tendon or tibial tubercle avulsion, persistent pain requiring arthrodesis, loosening, and joint stiffness requiring arthrotomy for excision of scar tissue), and an infection rate of 14%. The total complication rate was 57%. A satisfactory outcome (no pain and an unlimited ambulation distance) was obtained in only 10 patients (29%). There was no relationship between results and the angle at which the knee was ankylosed preoperatively. This study revealed that although success in reconstructing a previously ankylosed or arthrodesed knee is possible, the lack of consistent adequate motion and the complication rate may suggest that the surgeon reconsider the risks and benefits of this difficult procedure.
Question 99
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?

Explanation
While injury of the distal radial metaphysis is a rather common occurrence, the incidence of physeal arrest is only about 4% to 5% of patients. While injury of the distal physis of the ulna is rare, the incidence of physeal arrest is greater than 50% in fractures of this structure. These patients need to be followed closely both clinically and radiographically to look for the signs of distal ulnar/physeal arrest such as loss of the prominence of the ulna and ulnar deviation of the hand. Radiographically, progressive shortening of the ulna is observed. Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Question 100
High Yield
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Although technically challenging, the Ganz periacetabular osteotomy offers advantages over other rotational pelvic osteotomies. Posterior column integrity is maintained, as is the acetabular vascular supply. Free mobility of the fragment makes large corrections in the center edge angle possible. Because of the asymmetric cuts and the need to restore anterior coverage, there is a tendency to anterior displacement of the joint while flexing the acetabulum. The procedure is commonly performed through a Smith-Petersen incision. Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
