Introduction to Septic Arthritis of the Hand
Septic arthritis of the finger joints—specifically the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints—represents a profound orthopedic emergency. The articular cartilage of the small joints of the hand is highly susceptible to rapid enzymatic degradation. Proteolytic enzymes and matrix metalloproteinases released by both the invading pathogens (most commonly Staphylococcus aureus, or Pasteurella multocida in the context of animal bites) and the host's polymorphonuclear leukocytes can cause irreversible chondrolysis within 24 to 48 hours of inoculation.
Prompt surgical intervention via open drainage and copious irrigation is the gold standard of treatment. Delayed intervention invariably leads to catastrophic complications, including joint subluxation, secondary osteoarthritis, arthrofibrosis, and contiguous spread resulting in sequestrating osteomyelitis. This guide details the rigorous, evidence-based surgical protocols required for the open drainage of septic finger joints, including the management of complex proximal extensions into the flexor tendon sheaths and deep fascial spaces of the hand.
Surgical Anatomy and Biomechanics
A masterful understanding of the complex synovial and fascial anatomy of the hand is prerequisite for safely draining septic joints and addressing concomitant tenosynovial infections. The small joints of the hand are intimately associated with the extensor mechanism dorsally and the flexor tendon sheaths volarly.
The Metacarpophalangeal (MCP) Joint
The MCP joint is a condyloid joint stabilized by the proper and accessory collateral ligaments, the volar plate, and the sagittal bands of the extensor mechanism. The collateral ligaments are eccentric; they are lax in extension and taut in flexion (the "cam effect"). Surgical approaches to the MCP joint must respect these ligaments to prevent postoperative instability. Incisions into the joint capsule must be made strictly dorsal to the collateral ligaments.
Flexor Tendon Sheaths and Deep Hand Spaces
Infections of the volar finger joints frequently communicate with the flexor tendon sheaths, leading to acute pyogenic flexor tenosynovitis. The synovial sheaths of the index, middle, and ring fingers typically terminate at the level of the distal palmar crease. However, the sheaths of the thumb and little finger extend proximally into the wrist.

The flexor pollicis longus (FPL) sheath continues proximally as the radial bursa, while the sheath of the little finger continues proximally as the ulnar bursa.

In approximately 50% to 80% of patients, the radial and ulnar bursae communicate in the proximal palm or distal forearm (Parona's space), creating the anatomic basis for a "horseshoe abscess."
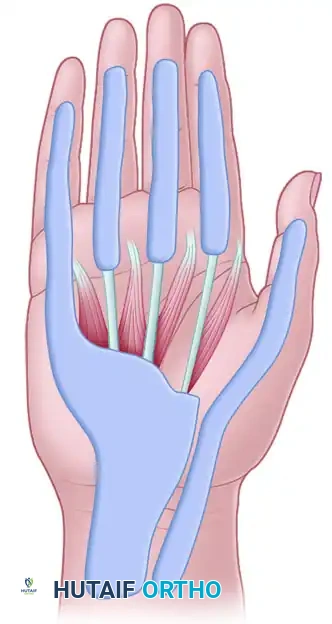
Furthermore, purulence can rupture from the tendon sheaths into the deep fascial spaces of the hand, specifically the thenar space and the midpalmar space, which are separated by the midpalmar septum extending from the third metacarpal.
The lumbrical canals also serve as potential conduits for the spread of infection from the palmar spaces to the dorsal subcutaneous spaces of the web spaces.

💡 Clinical Pearl: The Horseshoe Abscess
When evaluating a septic little finger with tenosynovial extension, always palpate the volar thumb and radial bursa. Due to the high rate of proximal communication between the ulnar and radial bursae, an infection originating in the fifth digit can rapidly track into the thumb, necessitating bilateral drainage.
Preoperative Preparation
Imaging and Laboratory Evaluation
Standard posteroanterior, lateral, and oblique radiographs of the affected digit and hand are mandatory. While early radiographs may only show soft tissue swelling or joint effusion, they serve as a critical baseline to rule out foreign bodies, fractures, or pre-existing osteomyelitis.
Laboratory evaluation should include a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). However, normal inflammatory markers do not preclude the diagnosis of a septic joint.
Anesthesia and Tourniquet Principles
General anesthesia or a regional brachial plexus block is preferred. Local infiltration (e.g., digital block) is strictly contraindicated in the setting of acute infection due to the risk of tracking bacteria into unaffected tissue planes and the reduced efficacy of local anesthetics in acidic, purulent environments.
🚨 Surgical Warning: Tourniquet Application
With the patient under appropriate anesthesia, apply and inflate a pneumatic tourniquet to the proximal arm, but do not wrap the arm with an Esmarch bandage for exsanguination. Exsanguinating an infected limb by wrapping it tightly from distal to proximal will forcefully express purulent material into proximal, uninfected fascial planes and the systemic circulation. Instead, elevate the arm for 3 to 5 minutes to allow for gravity exsanguination prior to tourniquet inflation.
Surgical Technique: Step-by-Step Open Drainage
1. Approach to the Metacarpophalangeal (MCP) Joint
The goal of the MCP joint approach is to achieve dependent drainage while preserving the critical stabilizing structures of the joint.
- Incision: Make a longitudinal incision on either the radial or ulnar side of the metacarpal head. The choice of side depends on the area of maximal fluctuance or erythema. A dorsal longitudinal incision directly over the extensor tendon should be avoided to prevent tendon adhesions and subsequent extensor lag.
- Dissection: Deepen the incision through the subcutaneous tissue, taking care to identify and protect the dorsal sensory branches of the radial or ulnar nerves.
- Extensor Mechanism: Identify the sagittal band and the extensor expansion. Retract the extensor expansion distally and dorsally to expose the underlying joint capsule.
- Capsulotomy: Identify the collateral ligament. Open the joint capsule strictly dorsal to the collateral ligament. Make the capsulotomy sufficiently large to allow for free drainage and the introduction of irrigation cannulas. Incising volar to or directly through the collateral ligament will result in profound postoperative joint instability.
- Debridement and Lavage: Obtain synovial fluid and tissue samples for aerobic, anaerobic, mycobacterial, and fungal cultures. Thoroughly irrigate the joint with a minimum of 500 mL to 1 liter of sterile normal saline. Use a blunt probe to gently break up any loculations within the joint recesses.
2. Approach to the Proximal and Distal Interphalangeal Joints (PIP and DIP)
- Incision: Utilize a mid-axial incision on either the radial or ulnar aspect of the affected digit. The mid-axial line connects the apices of the flexion creases and lies dorsal to the neurovascular bundle.
- Dissection: Carry the dissection down to the joint capsule, retracting the neurovascular bundle volarly.
- Capsulotomy: Similar to the MCP joint, incise the capsule dorsal to the collateral ligament. In the DIP joint, take extreme care not to violate the terminal extensor tendon insertion to prevent a postoperative mallet finger deformity.
- Irrigation: Perform copious irrigation. Given the small volume of these joints, a 20-gauge angiocatheter attached to a 10-cc syringe provides excellent pressurized irrigation.
3. Management of Tenosynovial Extension and Bursae
If the septic joint has ruptured volarly and seeded the flexor tendon sheath (pyogenic flexor tenosynovitis), the sheath must be drained concomitantly.
- Distal Drainage: Make a mid-axial incision over the middle or distal phalanx to access the distal extent of the flexor tendon sheath.
- Proximal Drainage: Make a palmar incision over the A1 pulley (distal palmar crease).
- Catheter Placement: Insert small 16- or 18-gauge polyethylene drainage tubes proximally into the sheath, and place small rubber drains distally. This allows for continuous or intermittent postoperative irrigation.
- Ulnar Bursa Exploration: If the little finger is involved, open the ulnar bursa on the ulnar side of the fifth digit. Pass a blunt probe proximally. Make a separate incision proximal to the wrist crease (in the distal forearm) to open the proximal extent of the ulnar bursa.
- Bursal Communication: If both the radial and ulnar bursae are involved (horseshoe abscess), one proximal ulnar incision in the distal forearm may be sufficient to drain both, because the two bursae communicate proximally in Parona's space in most patients. However, if drainage is inadequate, a separate volar radial incision proximal to the wrist crease must be made to drain the radial bursa.
4. Closure and Dressing
- Leave Wounds Open: The surgical incisions for septic joints and tenosynovitis must never be primarily closed. Primary closure traps residual bacteria and leads to recurrent abscess formation.
- Drains: Secure the 16- or 18-gauge polyethylene tubes with non-absorbable sutures.
- Dressing: Apply a non-adherent dressing (e.g., Xeroform or Adaptic) over the open wounds, followed by fluffed sterile gauze.
- Splinting: Apply a volar plaster splint in the intrinsic-plus position (safe position): wrist extended 20 to 30 degrees, MCP joints flexed 70 to 90 degrees, and PIP/DIP joints in full extension. This position maintains the collateral ligaments of the MCP joints at their maximal length, preventing contracture.
Complications of Delayed or Inadequate Treatment
Failure to promptly and adequately drain a septic finger joint leads to devastating sequelae. The enzymatic destruction of cartilage results in rapid joint space narrowing and secondary osteoarthritis, often necessitating eventual arthrodesis or arthroplasty.
Osteitis and Osteomyelitis
If the infection breaches the subchondral bone, or if a contiguous soft tissue infection (such as a felon in the digital pulp) is left untreated, osteitis and subsequent osteomyelitis will develop.

FIGURE 78-16: Osteitis of the distal phalanx caused by an untreated infection in the finger pulp (felon). Note the lytic destruction and loss of cortical margins at the tuft.
As osteomyelitis progresses, the vascular supply to the bone is compromised by purulent exudate under pressure and septic microthrombi. This leads to ischemic necrosis of the bone, resulting in the formation of a sequestrum (a piece of dead bone that has become separated during the process of necrosis from normal bone).
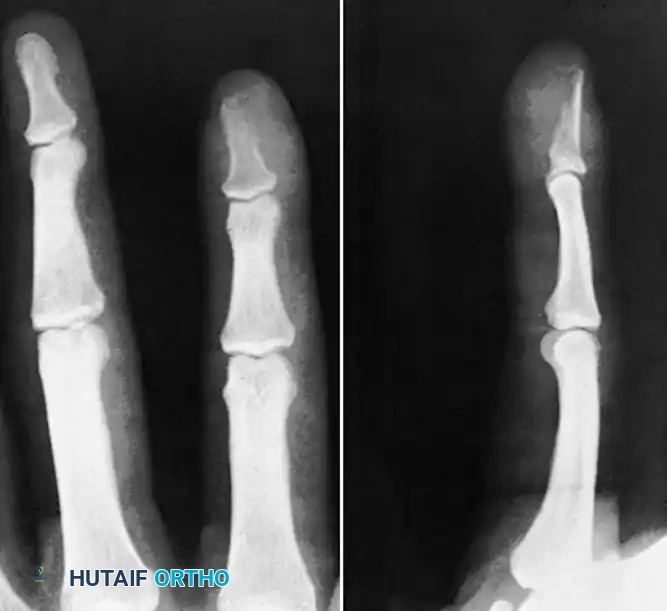
FIGURE 78-17: Sequestrating osteomyelitis of the middle phalanx. The radiograph demonstrates profound bony destruction, periosteal reaction, and a central radiodense sequestrum surrounded by a radiolucent involucrum.
Management of sequestrating osteomyelitis requires aggressive surgical debridement, removal of all necrotic bone (sequestrectomy), and often placement of local antibiotic spacers (e.g., PMMA beads) followed by prolonged systemic antimicrobial therapy. In severe cases with extensive bone loss and soft tissue compromise, ray amputation may be the most functional and definitive treatment.
Tendon Rupture
Prolonged exposure of the flexor or extensor tendons to purulence leads to tendon necrosis and spontaneous rupture. The flexor tendons are particularly vulnerable within the fibro-osseous canals due to their reliance on synovial diffusion for nutrition.
Postoperative Protocol and Rehabilitation
The postoperative management of a septic finger joint is a delicate balance between eradicating the infection and preventing debilitating stiffness.
- Inpatient Monitoring: The patient should be admitted for intravenous antibiotic therapy, elevation of the affected extremity, and close clinical monitoring.
- Antibiotic Therapy: Empiric broad-spectrum intravenous antibiotics (typically covering MRSA and Gram-negative organisms, e.g., Vancomycin and Ceftriaxone) should be initiated immediately after intraoperative cultures are obtained. The regimen is subsequently tailored based on final culture and sensitivity results.
- Irrigation: If continuous irrigation catheters were placed (16- or 18-gauge polyethylene tubes), they are typically flushed with sterile saline every 4 to 6 hours for the first 24 to 48 hours, or until the effluent is clear and clinical signs of infection improve.
- Wound Care: The bulky dressing is taken down at 48 hours. If the wound is clean and granulating, the drains are removed. If there is persistent purulence or necrotic tissue, a return to the operating room for a second-look debridement is mandatory.
- Rehabilitation: Early active range of motion (ROM) is the cornerstone of functional recovery. Once the acute inflammation has subsided (usually within 48 to 72 hours), the rigid splint is removed during the day to allow for supervised active and active-assisted ROM exercises under the guidance of a certified hand therapist. The splint is worn at night and between exercise sessions to prevent contractures.
- Outpatient Transition: Once the infection is clinically controlled and the patient is afebrile with down-trending inflammatory markers, they may be transitioned to oral antibiotics (based on sensitivities) to complete a 2- to 4-week course, depending on the presence of bone involvement.
By adhering to strict anatomical principles during surgical drainage and instituting aggressive postoperative rehabilitation, the orthopedic surgeon can successfully eradicate the infection while maximizing the functional salvage of the hand.
