Management of Old Unreduced Dislocations: Principles and Surgical Techniques
Key Takeaway
Old unreduced dislocations present a formidable challenge in orthopedic surgery, characterized by rapid hyaline cartilage degeneration, severe soft-tissue contractures, and disuse osteopenia. Management requires a highly individualized approach, balancing the patient's functional demands against the joint's viability. While closed reduction with skeletal traction may occasionally succeed, most chronic dislocations necessitate meticulous open reduction, often combined with salvage procedures such as arthroplasty or arthrodesis to restore stability and mitigate debilitating pain.
Introduction to Old Unreduced Dislocations
The management of old, unreduced dislocations represents one of the most technically demanding challenges in operative orthopedics. By fundamental orthopedic principles, any joint dislocation should be reduced as emergently as possible. When a joint remains dislocated over a prolonged period—typically defined as greater than three weeks—a cascade of irreversible pathophysiological changes occurs. The normal metabolic environment of the joint is severely disrupted, leading to rapid degradation of articular cartilage, profound soft-tissue contracture, and significant periarticular osteopenia.
Consequently, when an old unreduced dislocation is finally addressed, the surgeon and the patient must recognize that restoring normal, painless joint motion and native kinematic function is rarely achievable. The surgical strategy must pivot from simple anatomic restoration to functional salvage, often necessitating complex open reductions, arthroplasty, or arthrodesis. The selected intervention depends heavily on patient-specific factors, including the specific joint involved, the degree of articular cartilage necrosis, the presence of associated fractures, and the patient’s age, functional demands, and occupation.
Pathophysiology and Biomechanics of the Chronically Dislocated Joint
Understanding the pathophysiology of a chronic dislocation is paramount for preoperative planning and managing postoperative expectations.
Articular Cartilage Degeneration
Hyaline cartilage is avascular and relies entirely on the diffusion of nutrients from synovial fluid, a process driven by the cyclic loading and unloading of the joint. In a dislocated state, this mechanical pumping action ceases. Furthermore, the synovial fluid itself becomes pathologically altered due to capsular tearing and subsequent inflammatory cascades. The cartilage, deprived of nutrition and subjected to abnormal pressure against non-articular bony surfaces, undergoes rapid chondrocyte apoptosis and matrix degradation. Within weeks, irreversible fibrillation and full-thickness cartilage loss can occur.
Soft Tissue Contracture and Fibrosis
The empty joint capsule rapidly fills with dense, organized fibrovascular scar tissue. The ligaments and capsular structures on the side of the dislocation become foreshortened and contracted, while the structures on the opposing side become attenuated and scarred in an elongated position. This creates a formidable mechanical block to reduction.
Disuse Osteopenia
The absence of normal mechanical stress across the joint leads to rapid and profound regional osteopenia according to Wolff’s Law. The subchondral bone becomes structurally compromised, significantly increasing the risk of iatrogenic fractures during attempted reduction maneuvers.
Surgical Warning: Osteoporosis from disuse rapidly weakens the bones after a dislocation. Manipulative techniques, especially those employing rotational torque or excessive leverage, carry a high risk of iatrogenic fracture. If open techniques are employed, extreme caution must be exercised when using instruments such as bone levers or elevators, as the softened articular surfaces and metaphyses can be easily crushed or fractured.
General Principles of Management
The treatment algorithm for old unreduced dislocations is dictated by the chronicity of the injury, the patient's physiological age, and the specific joint involved.
Non-Operative Management
In select elderly or low-demand patients, an unreduced dislocation may eventually form a pseudoarthrosis that is relatively painless and allows for acceptable activities of daily living. If the unreduced dislocation is not restricting daily activities, is not excessively painful, and does not compromise distal neurovascular status, surgical treatment may be deferred in favor of benign neglect and functional rehabilitation.
Closed Reduction and Skeletal Traction
There is no arbitrary time limit beyond which a dislocation absolutely cannot be reduced by closed means, though success rates plummet after 2 to 3 weeks.
* Skeletal Traction: Heavy, prolonged skeletal traction can sometimes overcome severe soft-tissue contractures and slowly distract the joint, facilitating a delayed closed reduction or making a subsequent open reduction safer.
* Manipulation: If attempted after 2 to 3 weeks, manipulation must be performed under deep anesthesia with complete muscle relaxation. Force must be applied cautiously and gently, strictly avoiding high-velocity or high-torque maneuvers.
Open Reduction
Most old unreduced dislocations ultimately require open reduction. The surgical approach must be extensile to allow for complete visualization and circumferential release of contracted tissues.
* Young Adults and Children: Reduction alone (with meticulous repair or reconstruction of stabilizing ligaments) usually suffices, as their cartilage has a higher tolerance for ischemic insult and their functional demands require joint preservation.
* Middle-Aged and Elderly Patients: Open reduction is frequently combined with immediate arthroplasty or arthrodesis. The prognosis for a painless, functional native joint in this demographic is highly unfavorable due to pre-existing degenerative changes compounded by the dislocation.
Regional Considerations: The Ankle Joint
An old unreduced dislocation of the ankle without an associated fracture is an extreme clinical rarity. The inherent stability of the ankle mortise—provided by the congruency of the talus within the tibial plafond and the robust medial (deltoid) and lateral ligamentous complexes—dictates that the bone will typically fail before the ligaments in high-energy trauma. Therefore, the type and severity of the dislocation almost always depend on the specific fracture pattern.
Anterior Fracture-Dislocations
Anterior dislocations of the ankle are usually complicated by a fracture of the anterior margin of the distal articular surface of the tibia (a variant of a pilon fracture).
* Pathoanatomy: The talus translates anteriorly, driven by the wedge-like action of the posterior talar dome against the anterior tibial lip.
* Surgical Approach: An anterior approach to the ankle is typically utilized. The extensor retinaculum is incised, and the neurovascular bundle (deep peroneal nerve and anterior tibial artery) is carefully mobilized and protected.
* Reduction: The anterior tibial fragment must be mobilized, the joint debrided of intra-articular fibrosis, and the talus reduced posteriorly. Fixation is achieved with anterior-to-posterior lag screws or an anterior buttress plate.
Posterior Fracture-Dislocations
Posterior dislocations are the most common variant and are usually complicated by a fracture of the posterior margin of the distal tibia (Volkmann’s triangle) or by a complex trimalleolar fracture.
* Pathoanatomy: The talus is displaced posteriorly, often carrying a large posterior malleolar fragment attached via the intact posterior inferior tibiofibular ligament (PITFL).
* Surgical Approach: A posterolateral approach allows excellent visualization of the posterior malleolus and the lateral malleolus.
* Reduction: The fibula is typically reduced and provisionally fixed first to restore lateral column length. The posterior malleolus is then directly reduced and fixed with posterior-to-anterior lag screws or a posterior buttress plate, which inherently reduces the talus into the mortise.
Lateral Fracture-Dislocations
Lateral dislocations are invariably associated with bimalleolar or bimalleolar-equivalent (syndesmotic rupture with fibular fracture) injuries.
* Management: Treatment requires standard medial and lateral approaches to restore the fibular length and repair the medial malleolus or deltoid ligament, ensuring the talus is perfectly centralized beneath the tibial plafond.
Clinical Pearl: In chronic ankle fracture-dislocations, the articular cartilage of the talar dome is often severely scored or necrotic. If intraoperative assessment reveals full-thickness cartilage loss in a patient with high functional demands, primary tibiotalar arthrodesis should be strongly considered to prevent the need for a secondary salvage operation.
Regional Considerations: The Proximal Tibiofibular Joint
Dislocations of the proximal tibiofibular joint are frequently missed during initial trauma evaluations, often presenting weeks or months later as chronic lateral knee pain, instability, or peroneal nerve palsy.
Anatomy and Biomechanics
The proximal tibiofibular joint is a synovial joint that dissipates torsional stresses applied at the ankle and lateral tibial bending moments. Its stability relies on a complex ligamentous network.
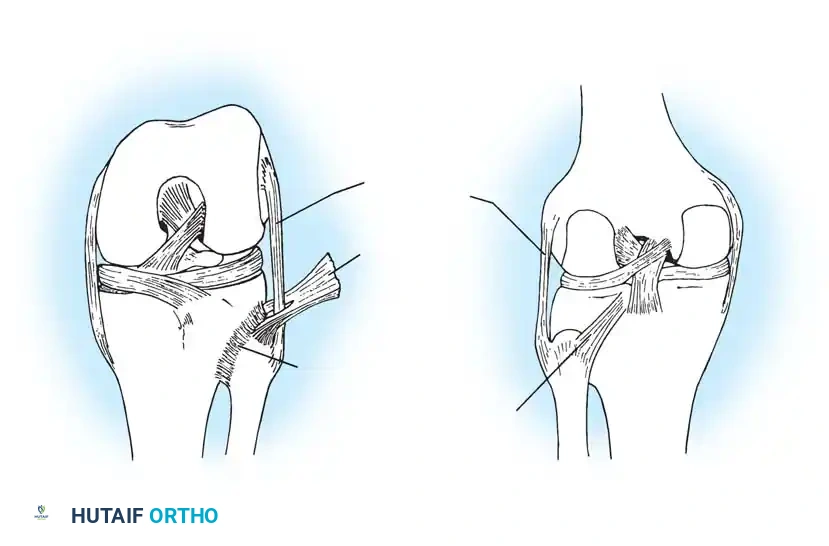
Fig. 58-1 Anatomy of proximal tibiofibular joint. Note the critical stabilizing structures: the Fibular collateral ligament, Posterior tibiofibular ligament, Biceps femoris tendon, and Anterior tibiofibular ligament.
As illustrated, the anterior and posterior tibiofibular ligaments provide primary restraint to anteroposterior translation. The biceps femoris tendon and the fibular collateral ligament (LCL) insert on the fibular head, meaning that proximal tibiofibular instability can profoundly affect the posterolateral corner (PLC) stability of the knee.
Classification of Chronic Dislocations
- Anterolateral: Most common. Caused by a fall on a flexed knee with the foot inverted and ankle plantarflexed.
- Posteromedial: Often associated with direct trauma or severe twisting injuries; carries a high risk of common peroneal nerve injury.
- Superior: Rare, usually associated with high-energy tibial shaft fractures or severe ankle syndesmotic injuries.
Surgical Management of the Chronic Proximal Tibiofibular Joint
When the dislocation is old and unreduced, simple open reduction and ligamentous repair are rarely successful due to severe attenuation of the anterior and posterior tibiofibular ligaments and contracture of the biceps femoris.
- Arthrodesis: Fusion of the proximal tibiofibular joint can provide definitive stability. However, it abolishes the normal physiologic rotation of the fibula during ankle dorsiflexion and plantarflexion. This can lead to increased stress on the distal tibiofibular syndesmosis and subsequent ankle pain. Therefore, arthrodesis is generally reserved for salvage cases and may require concurrent excision of a segment of the fibular shaft to de-couple the proximal and distal joints.
- Fibular Head Resection: Excision of the proximal fibula relieves the painful subluxation but completely destabilizes the lateral collateral ligament and biceps femoris. If this option is chosen, meticulous reconstruction of the posterolateral corner (advancing and anchoring the LCL and biceps tendon to the lateral tibial metaphysis) is absolutely mandatory.
- Ligamentous Reconstruction: In active patients, reconstructing the proximal tibiofibular ligaments using a semitendinosus autograft or allograft routed through bone tunnels in the tibia and fibula is the preferred method to restore stability while preserving physiologic joint mechanics.
Surgical Warning: The common peroneal nerve wraps directly around the fibular neck. In chronic posteromedial dislocations, the nerve may be encased in dense scar tissue or stretched over the displaced fibular head. A meticulous neurolysis must be the first step in any surgical approach to this region to prevent devastating iatrogenic foot drop.
Regional Considerations: The Foot
Old unreduced dislocations of the foot—including Lisfranc (tarsometatarsal) fracture-dislocations, Chopart (midtarsal) dislocations, and isolated subtalar dislocations—present unique challenges due to the complex, multi-planar biomechanics of the pedal arch.
Chronic midfoot dislocations inevitably lead to severe midfoot collapse, planovalgus or cavovarus deformities, and intractable pain. Because the articular cartilage of these tightly constrained joints is rapidly destroyed following dislocation, open reduction and internal fixation (ORIF) is rarely indicated in the chronic setting. Instead, the gold standard of treatment is in situ or corrective arthrodesis.
For chronic Lisfranc injuries, a partial or complete tarsometatarsal arthrodesis is performed, utilizing rigid plantar plating or crossed compression screws after meticulous debridement of the fibrotic neo-articulations. Restoration of the medial column length and the anatomic arch is critical to achieving a plantigrade, painless foot.
Postoperative Protocols and Rehabilitation
The postoperative management of old unreduced dislocations is a delicate balance between protecting the tenuous surgical repair and preventing profound joint stiffness.
- Immobilization: Due to the extensive soft-tissue releases required to achieve reduction, the joint is often inherently unstable postoperatively. A period of rigid immobilization (cast or heavy splint) is usually required for 2 to 6 weeks, depending on the joint and the security of the fixation.
- Graduated Range of Motion: Once initial soft-tissue healing has occurred, a highly supervised, graduated active and active-assisted range of motion protocol is initiated. Passive, forceful stretching is contraindicated, as it may provoke heterotopic ossification (especially in the elbow and hip) or compromise ligamentous reconstructions.
- Weight-Bearing: For lower extremity dislocations (ankle, knee, hip), weight-bearing is strictly protected until radiographic evidence of bony healing (in cases of fracture-dislocations or arthrodesis) or sufficient ligamentous maturation is observed, typically spanning 8 to 12 weeks.
Conclusion
The surgical management of old unreduced dislocations requires a masterclass in orthopedic judgment and technical execution. The surgeon must navigate distorted anatomy, severe soft-tissue contractures, and compromised bone stock. By adhering to strict principles of extensile exposure, meticulous neurovascular protection, and realistic functional goals—often utilizing arthroplasty or arthrodesis as primary salvage tools—the orthopedic surgeon can successfully restore stability and improve the quality of life for patients suffering from these debilitating chronic injuries.
📚 Medical References
- old unreduced dislocations of the shoulder, Surg Clin North Am 43:1671, 1963.
- Neviaser TJ: Old unreduced dislocations of the shoulder, Orthop Clin North Am 11:287, 1980.
- Oyston JK: Unreduced posterior dislocation of the shoulder treated by open reduction and transposition of the subscapularis tendon, J Bone Joint Surg 46B:256, 1964.
- Rockwood CA Jr: Fractures and dislocations about the shoulder. In Rockwood CA Jr, Green DP, eds: Fractures in adults, 2nd ed, Philadelphia, 1984, JB Lippincott. Rowe CR, Zarins B: Chronic unreduced dislocation of the shoulder, J Bone Joint Surg 64A:494, 1982.
- Schulz TJ, Jacobs B, Patterson RL: Unrecognized dislocations of the shoulder, J Trauma 9:1009, 1969.
- Wilson JC, McKeever FM: Traumatic posterior (retroglenoid) dislocation of the humerus, J Bone Joint Surg 31A:160, 1949.
- Yanmis I, Komurcu M, Oguz E, et al: The role of arthroscopy in chronic
You Might Also Like
