DEFINITION
Injury to the nail usually occurs by traumatic setting. Because of its location at the distal end of the digits, the perionychium is the most frequently injured part of the hand.9Restoration of normal nail appearance and function is best achieved by acute repair of the nail matrix. Reconstructive techniques may be used to provide a more normal-appearing nail.Excision of benign and malignant tumors involving the nail bed matrix may require techniques of nail bed repair and reconstruction also used for trauma.Optimal treatment depends on thorough understanding of the components of the perionychium—skin, sterile matrix, germinal matrix, eponychial fold, and distal phalanx—and their anatomic relationship with each other.
ANATOMY
The nail serves multiple functions: protecting the fingertip, regulating peripheral circulation, and contributing to sensory feedback of the fingertip.9,10The perionychium includes the nail plate, nail bed, hyponychium, eponychium and fold, and paronychium (FIG 1).The proximal portion of the nail matrix (approximately one-fourth of the nail length) is the germinal matrix and the distal three-fourths is the sterile matrix. The germinal matrix produces about 90% of the nail, whereas the sterile matrix produces the remaining 10% of the nail and produces the cells on the undersurface of the nail responsible for nail adherence.The hyponychium is the skin distal to the nail bed, the paronychium is the skin on each side of the nail, and the eponychium is the skin over the nail fold.The nail bed is adherent to the periosteum of the distal phalanx.
PATHOGENESIS
The main causes of nail deformity are trauma and tumor.The middle finger is the most commonly injured finger because of its length.13 Inadequate treatment in the acute setting often leads to a nail deformity.There is an associated distal phalanx fracture in 50% of nail bed injuries. This type of injury should be considered an open fracture and treated as such with irrigation and débridement, reduction of the fracture andfixation if necessary, and repair of the nail bed (FIG 2).1,4 Scarring can lead to a split nail deformity.Absence of nail matrix can lead to detachment of the nail.Lack of support from the distal phalanx leads to the hook nail deformity.Benign tumors (glomus tumor, distal interphalangeal joint ganglion) and malignant tumors (squamous cell carcinoma, melanoma) can affect nail appearance.
NATURAL HISTORY
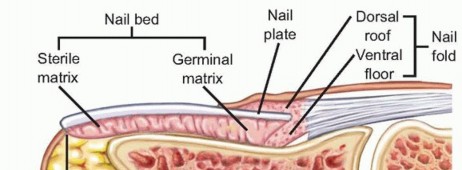
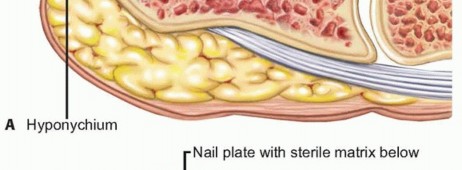
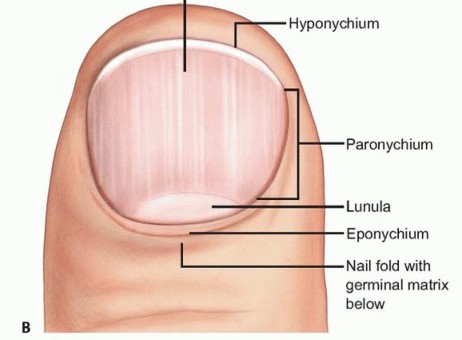
FIG 1 • A,B. The perionychium and its associated structures.
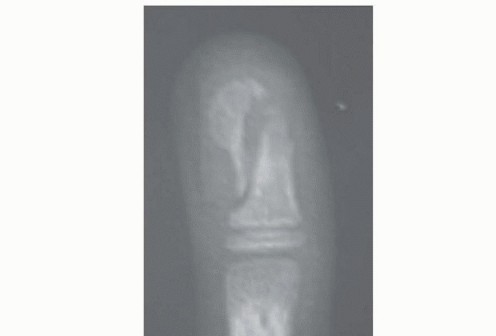

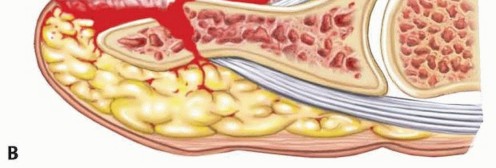
FIG 2 • A. Radiograph showing distal phalanx fracture associated with a nail bed crush injury. B. Nail bed injury with concomitant distal phalanx fracture. With a break in the periosteum, there is communication of the distal phalanx with the outside environment. There is a risk for osteomyelitis if not treated appropriately. If placed back on after repair, the old nail will remain adherent for 1 to 3 months and then fall off as a new nail pushes it off.12After nail repair, it will take about 12 months for the nail to achieve its final appearance. Thickening of the nail proximal to the level of injury is seen for about 50 days (FIG 3).9,12,13
PATIENT HISTORY AND PHYSICAL FINDINGS

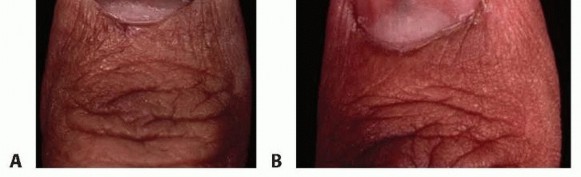
FIG 3 • A. Nail appearance at 3 months after repair. Patients should be aware of the heaped-up appearance as the nail grows distally. B. Nail appearance at 1 year after repair. Features of acute nail bed injurySubungual hematoma (FIG 4A,B): bleeding beneath the nail from laceration of the nail bedPain secondary to pressure in the space between the nail plate and the nail bed Treated with evacuation of hematoma by trephinationLaceration of nail bed (FIG 4C,D)Mechanism of injury usually is crush.Concomitant injury to fingertip skin or distal phalanx fracture may be present.Nail lacerations can be described in one of four ways: simple laceration, stellate laceration, severe crush, and avulsion.Repair of nail bed laceration and Kirschner wire fixation of distal phalanx fracture if unstable Nail bed avulsion (FIG 4E)Quality of avulsed nail matrix and size of defect will determine treatment.Treatment options include returning avulsed piece back into the defect or harvesting a split nail graft from the adjacent matrix or from the great toe. (A skin graft will prevent new grooving nail to adhere.)Posttraumatic nail deformitiesNail nonadherence or split nail (FIG 4F)Usually due to injury to the sterile matrix, which produces the cells responsible for adherence Excision of scar and primary closure or nail matrix reconstruction with a split graft from the great toeHook nail deformity (FIG 4G)Due to excessive tension at junction of nail bed and hyponychial skin and loss of support of distal phalanxRevision amputation or reconstruction of nail bed and bone graft to the distal tip of the distal phalanx Nail remnant (FIG 4H)Due to presence of residual germinal matrix not completely ablated at the time of initial repair or revision amputationComplete nail matrix ablation or revision amputationPincer nail deformity (FIG 4I): characterized by excessive transverse curvature of the nail and progressive pinching off of the distal fingertip, causing pain and abnormal appearancePartial or complete nail ablationReconstruction of nail bed with elevation of the lateral nail bed using dermal graft or AlloDerm
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP) and lateral radiographs of the distal phalanx are recommended to rule out a fracture.Depending on the level of injury, the following fractures are seen: distal tuft fracture, comminuted fracture, and a transverse or oblique fracture of the midshaft.Intra-articular fractures at the distal interphalangeal joint are rare with an associated nail bed injury.
DIFFERENTIAL DIAGNOSIS



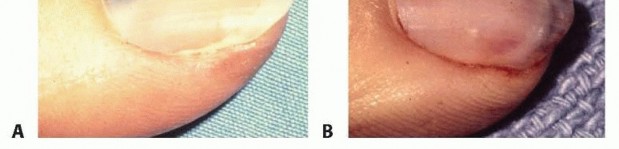
FIG 4 • Nail deformities. A,B. Subungual hematoma. C,D. Laceration of nail bed. E. Nail bed avulsion out of eponychial fold. F. Split nail deformity. G. Hook nail deformity. H. Nail remnant. I. Pincer nail deformity. Malignant tumorSquamous cell carcinoma Melanoma
NONOPERATIVE MANAGEMENT
Left untreated, traumatic injury to the nail matrix may result in an abnormal appearance and shape of the nail.
SURGICAL MANAGEMENT
Repair in the acute period increases the chance of a normal-appearing nail.Both surgeon and patient should be aware of the stages of nail growth and characteristic appearance at different points in the healing process as the nail regrows.Reconstruction of the nail matrix in a chronic injury should be approached with realistic expectations.Reconstruction of the nail matrix after tumor excision will depend on the amount of nail bed excised and the amount remaining.2,6,7,8
PREOPERATIVE PLANNING
Management of malignant tumors involving the nail bed requires an understanding of the optimal level ofamputation (usually to the level of the more proximal joint) and the need for sentinel node biopsy.
POSITIONING
To provide a bloodless field, use of a Penrose drain tourniquet at the base of the digit secured with a clamp is recommended (FIG 5).Use of a portion of a surgical glove as a tourniquet is discouraged because of the risk of leaving the tourniquet at the base of the digit after repair and placement of the dressing. The dressing may then hide the tourniquet, and vascular compromise and subsequent necrosis of the finger is possible in the postoperative period.
APPROACH

FIG 5 • Use of Penrose drain tourniquet at base of digit.
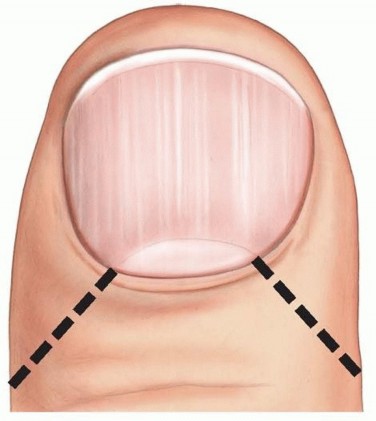
FIG 6 • Incisions made perpendicular to eponychial fold for exposure of the germinal matrix.
TECHNIQUE
Drainage of Subungual Hematoma
A standard surgical preparation is performed to prevent introducing bacteria into the subungual space.
Trephination of the nail can be accomplished using a heated paper clip, needle, or handheld battery-powered cautery (TECH FIG 1).
DRAINAGE OF SUBUNGUAL HEMATOMA
TECH FIG 1 • Trephination of the nail to drain a subungual hematoma using a heated paper clip (A) or battery-powered cautery (B).



TECH FIG 2 • Repair of nail bed laceration. A. Laceration with nail plate present. The nail plate is cleaned and will be used later as a splint to maintain the eponychial fold. B. Repair of nail bed and surrounding skin after débridement.(continued)


TECH FIG 2 •(continued)C. Nail plate being placed back into fold. D. Completed nail bed laceration repair.

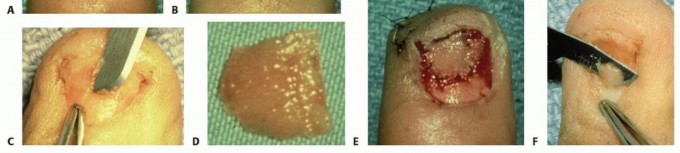
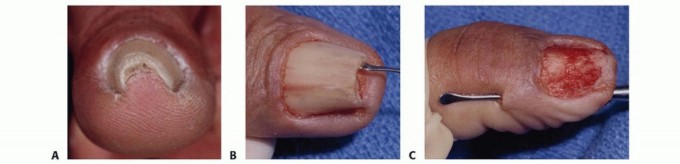
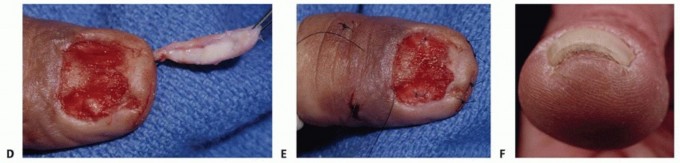
TECH FIG 3 • Treatment of nail bed loss with split nail graft. A. Initial presentation of this nail bed crush injury. B. Available tissue has been repaired, leaving a significant nail matrix defect. Exposed bone is visualized deep to the defect. C. Harvest of split sterile nail matrix graft from toe. D. Harvested split sterile nail matrix graft. E. Graft inset into defect to cover the exposed bone. F. Harvest of germinal matrix from the toe.


TECH FIG 4 • A. Right small finger after nail bed avulsion from fingertip trauma treated with nail bed ablation. Full-thickness skin graft was placed directly on the distal phalanx to preserve length and avoid revision amputation. Good take of skin graft was seen, but a nail remnant appeared on the proximal ulnar aspect of the fingertip, causing pain. B. Subcutaneous abscess from a nail remnant after revision amputation. C. Ablation of symptomatic nail remnant shown in A. An elliptical incision was made and all residual germinal matrices were removed with a scalpel. A curette was used to scrape the distal phalanx. D. A nail cyst is seen after incision and drainage of the abscess shown in B. The nail remnant was found within the cyst. Cyst and nail remnant were removed and symptoms resolved.
TECH FIG 5 • Treatment of pincer nail deformity. A. Pincer nail deformity with characteristic pinched-in appearance. B. The lateral borders of the nail are lifted from the distal phalanx in an atraumatic manner with a Kleinert-Kutz elevator. C. Creation of subcutaneous tunnels through stab incisions on the radial and ulnar sides. D. Placement of AlloDerm or dermal graft in subcutaneous tunnel. The graft is pulled into the tunnels with the aid of a suture in a distal to proximal direction. E. The wounds are closed, and the stitch is placed to hold the nail under the proximal nail fold. F. Postoperative appearance.
PEARLS AND PITFALLS
Traumatic injury1. With prompt treatment of nail bed injury, subacute and chronic problems can be avoided and a more complex reconstruction may be avoided.2. Failure to treat a nail bed laceration and concomitant distal phalanx fracture as an open fracture may result in osteomyelitis.3. Too much tension at the site of nail bed repair or a lack of support from the distal phalanx may result in a hook nail deformity.Nail growth ▪ An accurate repair of the nail matrix allows the nail plate to grow out with a smooth appearance and nail shape.1. The germinal matrix produces about 90% of the nail.2. The sterile matrix contributes cells that are responsible for nail adherence to the underlying nail bed.3. The nail grows at 0.1 mm a day.4. New nail growth is completed by 6-9 months.Nail bed reconstruction6. The goal of reconstruction is to restore the nail bed after loss due to trauma, scarring, or excision to allow more normal growth.7. Reconstruction of the sterile matrix can be accomplished with a split nail bed graft from the adjacent nail bed, an adjacent digit, or a toe.8. Reconstruction of the germinal and sterile matrices can be accomplished with a germinal and sterile matrix graft from the second toe but leaves a defect of the donor digit nail.
POSTOPERATIVE CARE
The postoperative dressing is left on for 5 to 7 days and may need to be soaked in a mixture of hydrogen peroxide and water for removal. The repaired nail is checked for signs of infection, seroma, and hematoma.Nonadherent gauze placed to maintain the eponychial fold should be removed. Any suture used to hold the nail or silicone sheet within the fold should also be removed at 5 to 7 days postoperatively.Sutures placed in the skin of the hyponychium or paronychium should be removed at 10 to 14 days after repair.A fingertip splint that does not include the proximal interphalangeal joint can be used for the first 3 to 5 weeks after injury to protect the nail bed repair and immobilize a distal phalanx fracture if present.Early motion of the proximal interphalangeal joint should be encouraged. The fingertip splint provides protection of the tip and will allow earlier motion of the injured digit.Hypersensitivity of the tip may be present for 1 to 3 months after injury, and desensitization exercises may be necessary to promote use of the affected digit.P.1249
OUTCOMES
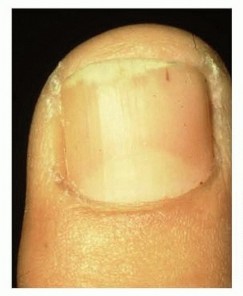
Although repair in the acute period provides the best chance for a normal-appearing nail (FIG 7), scarring at the site of injury may produce a nail deformity and patients should be reminded of this possibility at the time of repair.11,13,14Results of nail bed repair are adversely affected by avulsion or crush injury of the fingertip, presence of a distal phalanx fracture, three or more sites injured, and the need to use a silicone sheet for replacement of the nail.1,4,13Late reconstruction of the nail bed is often not as successful as surgeon or patient would desire.9Management plans must be individualized and realistic expectations must be discussed when treating patients with nail bed injuries.
COMPLICATIONS
REFERENCES
- Brown RE. Acute nail bed injuries. Hand Clin 2002;18:561-575.
- Brown RE, Zook EG, Russell RC. Reconstruction of fingertips with combination of local flaps and nail bed grafts. J Hand Surg Am 1999; 24(2):345-351.
- Brown RE, Zook EG, Williams J. Correction of pincer-nail deformities using dermal grafting. Plast Reconstr Surg 2000;105:1658-1661.
- Guy RJ. The etiologies and mechanisms of the nail bed injuries. Hand Clin 1990;6:9-19.
- Kumar VP, Satku K. Treatment and prevention of “hook nail” deformity with anatomic correlation. J Hand Surg Am 1993;18(4):617-620.
- Shepard GH. Nail grafts for reconstruction. Hand Clin 1990;6:79-102.
- Shepard GH. Perionychial grafts in trauma and reconstruction. Hand Clin 2002;18:595-614.
- Shepard GH. Treatment of nail bed avulsions with split thickness nail bed grafts. J Hand Surg Am 1983;8:49-54.
- Van Beek AL, Kassan MA, Adson MH, et al. Management of acute fingernail injuries. Hand Clin 1990;6:23-35.
- Zook EG. The perionychium: anatomy, physiology, and care of injuries. Clin Plast Surg 1981;8:21-31.
- Zook EG. Reconstruction of a functional and aesthetic nail. Hand Clin 2002;18:577-594.
- Zook EG, Brown RE. The perionychium. In: Green DP, ed. Operative Hand Surgery, ed 3. New York: Churchill Livingstone, 1993: 1283-1287.
- Zook EG, Guy RJ, Russell RC. A study of nail bed injuries: causes, treatment, and prognosis. J Hand Surg Am 1984;9(2):247-252.
- Zook EG, Van Beek AL, Russell RC, et al. Anatomy and physiology of the perionychium: a review of the literature and anatomic study. J Hand Surg Am 1980;5:528-536.
