INTRODUCTION AND PATHOANATOMY
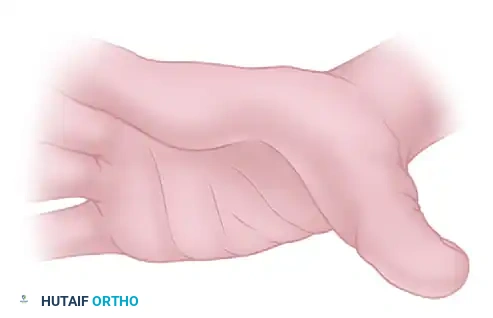
The thumb-in-palm deformity is one of the most debilitating upper extremity manifestations of upper motor neuron syndromes, most notably cerebral palsy, traumatic brain injury, and cerebrovascular accidents. This complex postural anomaly severely compromises hand function by obstructing the palm, thereby preventing effective grasp, pinch, and release mechanisms.
The pathoanatomy is driven by a profound muscle imbalance between spastic flexor-adductor forces and weak or flaccid extensor-abductor forces. Specifically, spasticity typically involves the adductor pollicis, the first dorsal interosseous, the flexor pollicis brevis (FPB), and the flexor pollicis longus (FPL). Conversely, the abductor pollicis longus (APL), extensor pollicis brevis (EPB), and extensor pollicis longus (EPL) are frequently weak or overstretched. Over time, this dynamic imbalance leads to fixed myostatic contractures and secondary joint instability, particularly at the metacarpophalangeal (MCP) and carpometacarpal (CMC) joints.
Clinical Pearl: Successful surgical reconstruction mandates a comprehensive approach. Addressing only the muscular contracture without augmenting the weak antagonist muscles or stabilizing a hypermobile MCP joint will inevitably lead to recurrence or a paradoxical deformity.
CLASSIFICATION OF THUMB-IN-PALM DEFORMITY
Surgical decision-making is heavily guided by the classification system popularized by House et al., which categorizes the deformity based on the specific joints involved and the underlying muscle imbalances:
- Type I: Isolated adduction contracture of the thumb metacarpal at the CMC joint. The MCP and interphalangeal (IP) joints are relatively spared.
- Type II: Metacarpal adduction contracture combined with a flexion deformity of the MCP joint.
- Type III: Metacarpal adduction contracture combined with a hyperextension deformity of the MCP joint. This is often a compensatory mechanism to clear the thumb from the palm.
- Type IV: Metacarpal adduction contracture combined with flexion deformities of both the MCP and IP joints, typically driven by severe FPL spasticity.
SURGICAL TECHNIQUE: COMPREHENSIVE THENAR MYOTOMY
For severe, fixed contractures where dynamic reconstruction is less feasible, a comprehensive thenar myotomy may be indicated to release the thumb from the palm and facilitate hygiene or basic assist-hand function.
Step-by-Step Approach
- Incision and Exposure: Make a longitudinal or slightly curved incision bordering the thenar crease in the palm.
- Nerve Protection: Carefully dissect through the subcutaneous tissue. It is absolutely critical to identify and protect the recurrent motor branch of the median nerve (the "million-dollar nerve") as it enters the thenar musculature, as well as the deep branch of the ulnar nerve innervating the adductor pollicis.
- Adductor Pollicis Release: Retract the long flexors of the fingers ulnarward. Identify the origin of the adductor pollicis on the third metacarpal and strip it subperiosteally.
- Thenar Intrinsic Release: Proceed to the deep transverse carpal ligament. Release approximately two-thirds of the origin of the abductor pollicis brevis (APB) and the entire origins of the flexor pollicis brevis (FPB) and opponens pollicis.
- First Dorsal Interosseous Release: Strip the origin of the first dorsal interosseous muscle from the ulnar aspect of the first metacarpal.
- Joint Assessment: Evaluate the MCP joint. If severe capsular contracture persists, perform a volar capsulorrhaphy of the MCP joint to allow neutral positioning.
Surgical Warning: Over-aggressive release without protecting the neurovascular bundles can lead to an insensate, flail thumb. Meticulous hemostasis and loupe magnification are mandatory.
SURGICAL TECHNIQUE: THE HOUSE ET AL. DYNAMIC APPROACH
For patients with functional potential, a dynamic reconstructive approach is preferred. This involves a triad of interventions: release of contractures, augmentation of weak muscles, and skeletal stabilization.
Step 1: Release of Contractures
The goal of this phase is to eliminate the deforming spastic forces while preserving bridging muscle fibers where possible to maintain some active control.
- Incision: Utilize a broad Z-plasty incision located along the first web space. This not only provides excellent exposure but also addresses the cutaneous web space contracture that invariably accompanies long-standing adduction deformities.
- First Dorsal Interosseous Release: Through the dorsal limb of the incision, identify and release the origin of the first dorsal interosseous muscle from the thumb metacarpal.
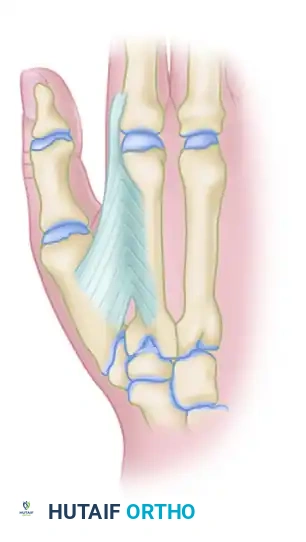
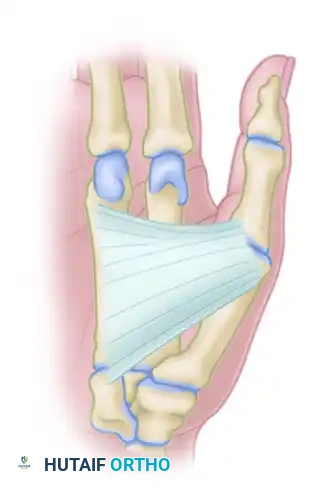
Figure 72-13A: Release of the adduction contracture through a Z-plasty first web incision, demonstrating the release of the first dorsal interosseous and adductor pollicis.
- Adductor Pollicis Lengthening: Expose the intramuscular portion of the adductor pollicis tendon. Divide it obliquely. This technique allows for a relative lengthening of the tendon while preserving bridging muscle fibers, preventing a complete loss of adduction power.
- Addressing Type-Specific Deformities:
- Type II Deformity (MCP Flexion): Release the origin of the adductor and the flexor pollicis brevis (FPB) to correct the MCP flexion posture.
- Type IV Deformity (FPL Spasticity): If the IP joint is held in rigid flexion due to FPL spasticity, perform a fractional lengthening of the FPL tendon proximal to the wrist via a separate volar forearm incision.
Step 2: Augmentation of Weak Muscles
Once the deforming forces are released, the weak abductors and extensors must be augmented to pull the thumb out of the palm dynamically.
- APL Mobilization: If adduction of the thumb at the CMC joint is considerable and the APL is weak, release the APL tendon from the first dorsal extensor compartment. Allow the tendon to subluxate volarly, which improves its mechanical advantage for palmar abduction.
- Active Tendon Transfer:
- Identify and divide the palmaris longus (PL) tendon at the level of the wrist crease.
- Reroute the PL and suture it into the mobilized APL tendon in an end-to-side fashion using a Pulvertaft weave or strong core sutures.
- Alternative Donors: If the PL is absent or unsuitable, the brachioradialis (BR) or the flexor carpi radialis (FCR) can be utilized.
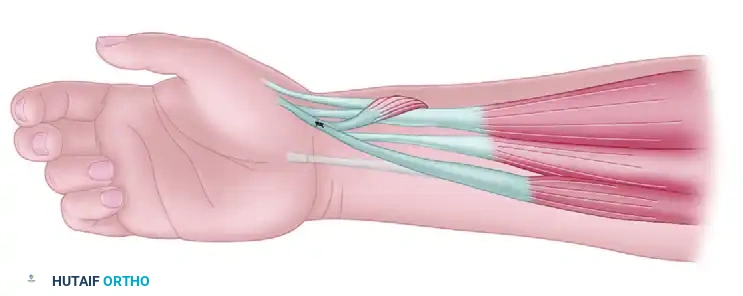
Figure 72-13B: Transfer of the palmaris longus to the intact abductor pollicis longus, which has been released from the first dorsal compartment to enhance abduction vector.
- Dynamic Tenodesis (Salvage): If there is no suitable donor muscle available for an active transfer, a dynamic tenodesis is performed.
- Divide the APL tendon proximally.
- Reroute its distal portion volarly and attach it in an end-to-side fashion to the FCR tendon.
- Set the tension strictly to maintain metacarpal abduction. This provides a passive "checkrein" that abducts the thumb when the wrist is extended (tenodesis effect).
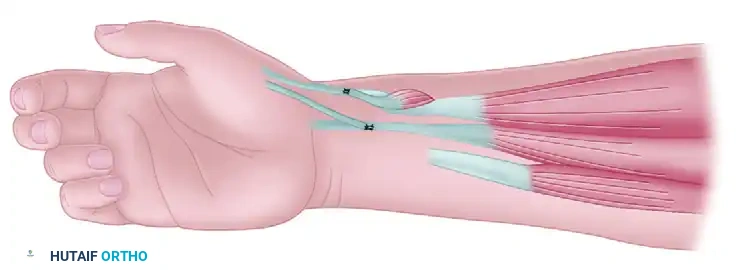
Figure 72-13C: Dynamic tenodesis utilizing the distal portion of the APL tendon transferred to the FCR, with the proximal segment of the APL transferred into the EPB.
Clinical Pearl: If a significant flexion deformity exists at the MCP joint but joint stability is otherwise normal, a similar tenodesis of the extensor pollicis brevis (EPB) tendon may be performed. However, extreme caution must be exercised to avoid overtensioning, which can create a disabling iatrogenic hyperextension deformity at the MCP joint.
Step 3: Skeletal Stabilization
A hypermobile or unstable MCP joint will absorb the force of any tendon transfer, rendering the reconstruction ineffective. Stabilization is paramount, particularly in Type III (hyperextension) deformities.
Option A: Chondrodesis (For Skeletally Immature Patients)
1. Approach the MCP joint dorsally.
2. Carefully shave and remove the articular cartilage of the MCP joint down to bleeding subchondral bone, strictly avoiding damage to the open physis.
3. Position the thumb in approximately 15 to 20 degrees of flexion and secure it with a single, centrally placed 1.0-mm or 1.2-mm Kirschner wire driven longitudinally across the joint.
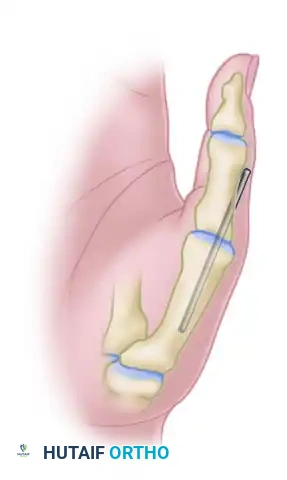
Figure 72-13D: Chondrodesis of the thumb metacarpophalangeal joint for the correction of a hyperextension deformity.
Option B: Sesamoid Arthrodesis (Zancolli, Lawson, and Tonkin Technique)
For patients with MCP extension instability where joint preservation is desired, volar capsulodesis via sesamoid advancement is highly effective.
- Approach: Expose the MCP joint through a dorsoradial or mid-lateral incision.
- Mobilization: Identify the palmar plate. Divide the accessory collateral ligament at its insertion to fully mobilize the palmar plate-sesamoid complex.
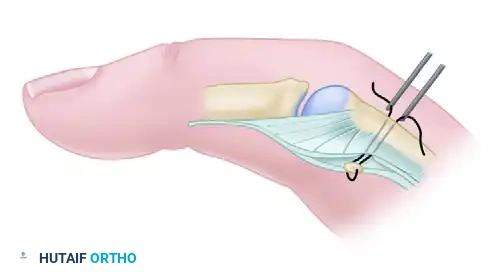
Figure 72-14A: The palmar plate is mobilized by dividing the accessory collateral ligament. The articular surface of the sesamoid is denuded of cartilage, and a cortical defect is created at the metacarpal head-neck junction.
- Preparation: Denude the articular cartilage from the dorsal surface of the radial sesamoid. Create a matching cortical trough or defect at the volar head-neck junction of the first metacarpal.
- Fixation: Pass two heavy non-absorbable intraosseous sutures (e.g., 2-0 Polypropylene or braided composite) through the sesamoid-palmar plate complex.
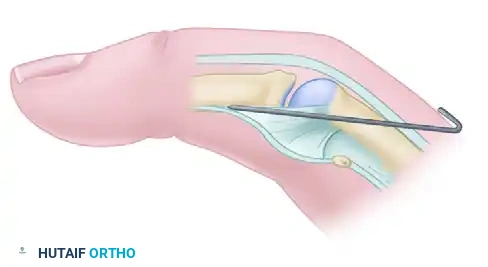
Figure 72-14B: Two straight needles are used to pass the suture through the sesamoid-palmar plate complex and the metacarpal neck to secure the sesamoid into the created cortical defect.
- Tensioning and Pinning: Flex the thumb MCP joint to 30 degrees. Draw the sutures through the metacarpal neck and tie them securely over the dorsal surface of the metacarpal, deep to the extensor tendons.
- Temporary Stabilization: Drive a Kirschner wire obliquely across the MCP joint to protect the repair, maintaining the joint in 30 degrees of flexion. Repair the seam in the collateral ligament and suture the proximal radial edge of the palmar plate to the metacarpal periosteum.
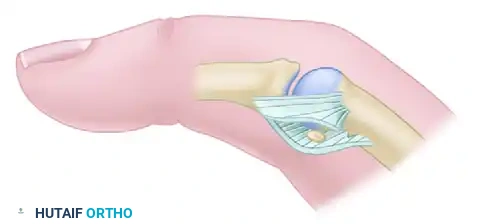
Figure 72-14C: The intraosseous suture is tied over the metacarpal under the extensor tendons. A Kirschner wire maintains the joint in 30 degrees of flexion while the repair heals.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of thumb-in-palm reconstruction relies heavily on strict adherence to postoperative immobilization and subsequent specialized hand therapy.
- Immediate Postoperative Phase (0-4 Weeks):
- Apply a bulky, well-padded pressure dressing in the operating room.
- Transition to a rigid fiberglass or plaster cast (or volar splint) holding the forearm, wrist, and hand.
- Crucial Positioning: The first metacarpal (not just the phalanges) must be held in wide palmar abduction and opposition. If the phalanges are pushed into abduction without controlling the metacarpal, an iatrogenic MCP hyperextension deformity will occur.
- Intermediate Phase (4-6 Weeks):
- At 4 to 5 weeks, the Kirschner wires (if used for skeletal stabilization) are removed in the clinic.
- If tendon transfers were performed, continuous immobilization is maintained for a total of 6 weeks to allow for robust tendon-to-tendon healing.
- Rehabilitation Phase (6+ Weeks):
- Remove the cast and sutures.
- Fabricate a custom thermoplastic resting splint to hold the thumb in abduction and opposition.
- Initiate active and active-assisted range of motion (ROM) exercises for the wrist, thumb, and fingers under the guidance of a certified hand therapist.
- Long-Term Care: Splinting at night is strictly enforced for a minimum of 6 to 12 months, and sometimes indefinitely in growing children with severe spasticity, to prevent recurrence of the myostatic contracture.
COMPLICATIONS AND SURGICAL PITFALLS
- Recurrence of Deformity: The most common complication, usually resulting from inadequate initial release of the adductor pollicis or failure to comply with postoperative night splinting.
- Iatrogenic Hyperextension (Swan Neck of the Thumb): Caused by over-tensioning an EPB tenodesis or failing to stabilize a hypermobile MCP joint during the index procedure.
- Nerve Injury: Damage to the recurrent motor branch of the median nerve or the digital nerves during the first web space Z-plasty. Meticulous superficial dissection is required.
- Tendon Transfer Rupture: Early unprotected mobilization before 6 weeks can lead to pull-out of the Pulvertaft weave. Strict immobilization is non-negotiable.
📚 Medical References
- thumb-in-palm deformity in cerebral palsy: evaluation and results in fi fty-six patients, J Bone Joint Surg 63A:216, 1981.
- Johnstone BR, Richardson PW, Coombs CJ, et al: Functional and cosmetic outcome of surgery for cerebral palsy in the upper limb, Hand Clin 19:679, 2003.
- Manske PR, Langewisch KR, Strecker WB, et al: Anterior elbow release of spastic elbow fl exion deformity in children with cerebral palsy, J Pediatr Orthop 21:772, 2001.
- Matsuo T, Matsuo A, Hajime T, et al: Release of fl exors and intrinsic muscles for fi nger spasticity in cerebral palsy, Clin Orthop Relat Res 384:162, 2001.
- Mital MA: Lengthening of the elbow fl exors in cerebral palsy, J Bone Joint Surg 61A:515, 1979.
- Mital MA, Sakellarides HT: Surgery of the upper extremity in the retarded individual with spastic cerebral palsy, Orthop Clin North Am 12:127, 1981.
- Mowery CA, Gelberman RH, Rhoades CE: Upper extremity tendon transfers in cerebral palsy: electromyographic and functional analysis, J Pediatr Orthop 5:69, 1985.
- Patella V, Franchin B, Moretti B, et al: Arthrodesis of the wrist with mini-fi xators in infantile cerebral palsy, Ital J Orthop Traumatol 10:75, 1984.
- Patella V, Martucci G: Transposition of the pronator radii teres muscle to the radial extensors of the wrist in infantile cerebral paralysis: an improved operative technique, Ital J Orthop Traumatol 6:61, 1980.
- Sakellarides HT, Mital MA, Lenzi WD: Treatment of
