Management of the Spastic Upper Extremity: Nonoperative Strategies and Surgical Reconstruction
Key Takeaway
The management of the spastic upper extremity in cerebral palsy requires a multidisciplinary approach. While nonoperative modalities like splinting, hand therapy, and botulinum toxin injections temporarily mitigate spasticity and prevent contractures, definitive treatment often necessitates surgical intervention. Procedures such as fractional lengthening, FCU-to-ECRL tendon transfers, and thumb-in-palm reconstruction are critical for restoring functional wrist extension, pinch kinematics, and overall upper extremity biomechanics in carefully selected patients.
Comprehensive Introduction and Patho-Epidemiology
The management of the spastic upper extremity, most frequently encountered in the context of cerebral palsy (CP), traumatic brain injury (TBI), or cerebrovascular accidents (CVA), represents one of the most complex challenges in reconstructive orthopaedic surgery. Spasticity is formally defined as a velocity-dependent increase in the tonic stretch reflex (muscle tone) with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex as one component of the upper motor neuron (UMN) syndrome. This neuropathological state arises from the disruption of descending inhibitory pathways, specifically the corticospinal and reticulospinal tracts, which subsequently leads to uninhibited alpha and gamma motor neuron activity at the spinal cord level. The resulting continuous, unchecked muscle contraction initiates a cascade of biomechanical and histological alterations within the affected extremity.
Epidemiologically, cerebral palsy remains the most common motor disability in childhood, with a prevalence of approximately 2 to 3 per 1,000 live births. Upper extremity involvement is nearly universal in spastic hemiplegia and quadriplegia. In the adult population, traumatic brain injury and stroke contribute to a vast and growing cohort of patients suffering from acquired upper extremity spasticity. Regardless of the etiology, the natural history of the spastic limb follows a predictable pathophysiological continuum. Initially, the deformity is purely dynamic, driven entirely by neuromuscular hypertonia. During this phase, the limb assumes abnormal postures during active movement or agitation but can be passively corrected to a neutral physiological position when the patient is relaxed or asleep.
However, if left untreated, this dynamic hypertonia inexorably progresses to fixed myostatic contracture. At the cellular level, prolonged spasticity induces a reduction in the number of serial sarcomeres within the muscle belly, an increase in intramuscular connective tissue, and the deposition of non-contractile collagen. This structural shortening of the musculotendinous unit is further compounded by secondary capsular contractures of the adjacent joints. The primary goals of intervention—whether nonoperative or surgical—are to interrupt this degenerative continuum, improve the patient's functional capacity, facilitate activities of daily living (ADLs), enhance hygiene, and optimize the cosmetic appearance of the limb.
Historically, the paradigm of care relied heavily on prolonged, and often rigid, nonoperative modalities. However, modern orthopaedic consensus recognizes that while nonoperative management is foundational, it serves primarily to delay the onset of fixed myostatic contractures, optimize the patient for eventual surgical reconstruction, and maximize the efficacy of postoperative rehabilitation. The contemporary approach requires a highly nuanced, multidisciplinary strategy that seamlessly integrates the expertise of orthopaedic surgeons, neurologists, physiatrists, and specialized hand therapists to tailor interventions to the patient's specific pattern of motor deficit, cognitive capacity, and functional potential.
Detailed Surgical Anatomy and Biomechanics
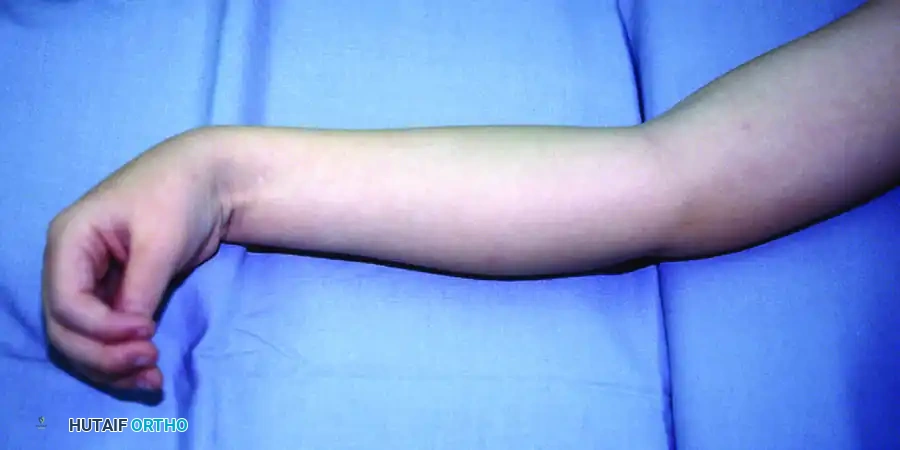
A profound understanding of the surgical anatomy and the altered biomechanics of the spastic upper extremity is the absolute prerequisite for successful reconstructive intervention. The characteristic posture of the spastic upper limb is a direct manifestation of the predictable imbalance between the dominant, hypertonic flexor-pronator muscle groups originating from the medial epicondyle and the weaker, often overstretched extensor-supinator groups originating from the lateral epicondyle. The classic presentation includes internal rotation and adduction of the shoulder, flexion of the elbow, pronation of the forearm, flexion and ulnar deviation of the wrist, flexion of the digits, and a severe thumb-in-palm deformity.

The biomechanics of the spastic wrist are primarily dictated by the overpowering force of the flexor carpi ulnaris (FCU) and the pronator teres (PT). The FCU is typically the most spastic and functionally dominant muscle in the forearm. Its anatomical insertion onto the pisiform, hook of the hamate, and base of the fifth metacarpal provides it with a massive moment arm for both wrist flexion and ulnar deviation. This continuous volar and ulnar pull overpowers the extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), and extensor carpi ulnaris (ECU). The pronator teres, acting in concert with the pronator quadratus, drives the forearm into fixed pronation, severely limiting the patient's ability to position the hand in space for functional grasp and release.
The thumb-in-palm deformity is a complex, multi-planar biomechanical fault that profoundly devastates hand function by obliterating the first web space and preventing opposition. This deformity is driven by a combination of extrinsic and intrinsic spasticity. Extrinsically, the flexor pollicis longus (FPL) pulls the thumb interphalangeal (IP) joint into severe flexion. Intrinsically, the adductor pollicis (transverse and oblique heads), the deep head of the flexor pollicis brevis (FPB), and the first dorsal interosseous contract to pull the first metacarpal tightly against the second metacarpal. This spastic dominance is exacerbated by the profound weakness of the antagonistic abductor pollicis longus (APL), extensor pollicis brevis (EPB), and extensor pollicis longus (EPL).
At the digital level, spasticity of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) results in a tightly clenched fist. The biomechanical interplay between the extrinsic flexors and the intrinsic musculature (lumbricals and interossei) can also lead to secondary swan-neck deformities. In the spastic hand, intrinsic hypertonia causes flexion at the metacarpophalangeal (MCP) joints and hyperextension at the proximal interphalangeal (PIP) joints. When planning surgical reconstruction, the surgeon must meticulously evaluate the tension across all joints to differentiate between extrinsic tightness (which worsens with wrist extension) and intrinsic tightness (which worsens with MCP extension), as this dictates the specific level of surgical release or lengthening required.
Exhaustive Indications and Contraindications
The decision-making process regarding when to transition from nonoperative management to surgical reconstruction is highly complex and individualized. Surgery is generally indicated when nonoperative modalities (such as targeted botulinum toxin injections, dynamic splinting, and therapy) have been exhausted, or when fixed myostatic contractures and severe dynamic deformities impede function, cause pain, or prevent adequate hygiene. In patients with functional potential, the primary indication is to improve the active positioning of the hand in space, facilitate voluntary grasp and release, and enhance the performance of bimanual activities. In non-functional, severely affected extremities, the indications pivot toward salvage goals: facilitating nursing care, preventing skin maceration in the palmar creases, and alleviating pain associated with severe contractures.
A critical factor in determining surgical candidacy is the patient's cognitive status, voluntary motor control, and sensory perception. Patients with a profound intellectual disability who cannot comply with rigorous postoperative rehabilitation protocols are generally poor candidates for complex tendon transfers, as these procedures require cortical re-education to fire the transferred muscle in its new functional phase. Similarly, profound sensory impairment, particularly astereognosis or a lack of two-point discrimination, often leads to "learned nonuse." Even if a perfect biomechanical reconstruction is achieved, a patient with a sensate-deprived hand will neurologically ignore the extremity, rendering the surgical functional outcome poor. In such cases, surgical goals must be strictly limited to hygiene and passive positioning.
Contraindications to surgical reconstruction must be carefully respected to avoid catastrophic functional deterioration. Absolute contraindications include the presence of purely dynamic spasticity that is still highly responsive to botulinum toxin type A (BoNT-A) in a very young child (typically under the age of 5 or 6), as the neurological maturation of the central nervous system is still ongoing. Operating too early on dynamic deformities frequently leads to over-lengthening, resulting in an irreversible loss of grip strength and an iatrogenic extension deformity. Furthermore, the presence of severe, uncontrolled athetosis or dystonia is a strong relative contraindication, as these unpredictable, involuntary movement disorders can rapidly destroy surgical repairs and tendon transfers.
| Category | Indications for Surgical Reconstruction | Contraindications for Surgical Reconstruction |
|---|---|---|
| Functional Status | Presence of selective voluntary motor control; Ability to perform bimanual tasks; Adequate cognitive capacity for rehabilitation. | Lack of voluntary motor control (for functional tendon transfers); Severe, profound cognitive impairment precluding therapy. |
| Contracture Type | Fixed myostatic contractures unresponsive to serial casting or BoNT-A; Severe dynamic deformities causing functional impairment. | Purely dynamic deformities in young children (< 5 years); Deformities fully correctable with nonoperative modalities. |
| Sensory Function | Intact protective sensation; Presence of stereognosis and acceptable two-point discrimination. | Profound astereognosis; Dense sensory loss leading to irreversible "learned nonuse." |
| Neurological Stability | Stable, non-progressive neurological lesion (e.g., static encephalopathy, remote stroke). | Evolving neurological status; Severe, uncontrolled athetosis, chorea, or dystonia. |
| Hygiene/Salvage | Severe flexion contractures causing palmar skin maceration, recurrent fungal infections, or intractable pain. | Medically unstable patient unfit for general anesthesia; Active local soft tissue infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative clinical assessment is the cornerstone of successful surgical intervention in the spastic upper extremity. The surgeon must meticulously differentiate between dynamic spasticity and fixed myostatic contracture. This is often achieved through the judicious use of diagnostic nerve blocks or botulinum toxin injections. By temporarily paralyzing the hypertonic muscle group (e.g., a median and ulnar nerve block at the elbow), the surgeon can unmask the true underlying structural contracture. If the deformity completely resolves following the block, it is purely dynamic, and tendon lengthening may be deferred or minimized. If the deformity persists, a fixed myostatic or capsular contracture is present, necessitating structural surgical release.

Clinical evaluation must utilize validated classification systems to guide surgical templating. The Zancolli classification is paramount for evaluating the spastic wrist and hand. A Zancolli Group 1 patient has active finger extension with the wrist in neutral or extension. A Group 2 patient has active finger extension only when the wrist is flexed (Group 2A: active wrist extension is possible with fingers flexed; Group 2B: no active wrist extension is possible). Group 3 patients possess no active finger or wrist extension. This classification directly dictates the surgical plan: Group 1 may only need flexor lengthening; Group 2A requires flexor lengthening and possible FCU transfer; Group 2B requires flexor lengthening, robust tendon transfers (e.g., FCU to ECRB/ECRL), and potentially intrinsic releases; Group 3 may require salvage procedures such as proximal row carpectomy or total wrist arthrodesis.
Similarly, the House classification is utilized to categorize the thumb-in-palm deformity based on the specific spastic muscles involved. House Type I involves simple adductor spasticity. Type II involves adductor and FPB spasticity. Type III involves adductor, FPB, and FPL spasticity. Type IV involves the entire intrinsic and extrinsic flexor complex. Preoperative templating involves mapping out each specific muscular deficit and matching it with an available, expendable donor muscle of appropriate excursion and cross-sectional area. The brachioradialis (BR), pronator teres (PT), and flexor carpi ulnaris (FCU) are the most common donors utilized in the spastic upper extremity.
Patient positioning and operating room setup must be optimized for complex, multi-level upper extremity reconstruction. The patient is positioned supine with the affected arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied high on the brachium. The entire upper extremity, from the fingertips to the axilla, is prepped and draped free to allow for intraoperative assessment of resting tension and the tenodesis effect. Loupe magnification (typically 2.5x to 3.5x) is essential for the meticulous dissection of musculotendinous junctions and the preservation of critical neurovascular structures during fractional lengthenings and tendon transfers.
Nonoperative Strategies: Splinting, Therapy, and Chemodenervation
Prior to surgical intervention, a rigorous trial of nonoperative management is mandatory. Hand therapy focuses on strengthening nonspastic antagonist muscles, utilizing neurodevelopmental techniques to control exaggerated reflexes, and providing serial assessments to evaluate cognitive readiness for postoperative rehabilitation. Orthotic management has evolved from rigid, full-time splinting—which often causes functional inhibition and learned nonuse—to dynamic, functional orthoses that provide wrist extension while allowing active digital flexion.
Neuromodulation via electrical stimulation (NMES) is frequently utilized as a preoperative conditioning tool to recruit Type II muscle fibers in weakened extensors. Furthermore, the targeted use of Botulinum Toxin Type A (BoNT-A) has revolutionized preoperative planning. By cleaving the SNAP-25 protein and inhibiting acetylcholine release, BoNT-A provides a reversible chemical denervation. This pharmacological lengthening creates a "window of opportunity" for therapy, helps correct resting posture, and serves as an invaluable diagnostic tool to differentiate dynamic spasticity from fixed contractures prior to committing to the scalpel.
Step-by-Step Surgical Approach and Fixation Technique
The surgical reconstruction of the spastic hand is highly individualized, but a comprehensive reconstruction for a severe Zancolli Group 2B wrist with a House Type III thumb-in-palm deformity typically involves a triad of procedures: fractional flexor lengthening, tendon transfers for wrist extension, and intrinsic/extrinsic releases for the thumb. The procedure is performed under general anesthesia with tourniquet control.
Fractional Lengthening of the Volar Flexors
To address the severe flexion contracture of the digits and wrist without sacrificing grip strength entirely, fractional (aponeurotic) lengthening is the gold standard. Complete tenotomies or Z-lengthenings in the distal forearm are generally avoided in functional hands, as they carry a high risk of over-lengthening and catastrophic loss of active flexion.
* Surgical Approach: A longitudinal, volar-ulnar incision is made over the middle to distal third of the forearm. The antebrachial fascia is incised, and the flexor carpi ulnaris is retracted ulnarly to expose the underlying flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) muscle bellies.
* Technique: The musculotendinous junctions of the FDS, FDP, and flexor carpi radialis (FCR) are meticulously identified. Using a #15 blade, transverse incisions are made through the glistening tendinous aponeurosis of each muscle belly. It is absolutely critical to preserve the underlying red muscle fibers; cutting into the muscle belly risks denervation and severe hemorrhage.
* Correction and Tensioning: Once the aponeuroses are incised, the surgeon passively extends the wrist and fingers. The intact muscle fibers slide past one another, allowing the musculotendinous unit to lengthen by 1.5 to 2.0 centimeters. The surgeon must carefully observe the resting cascade of the hand to ensure adequate, but not excessive, lengthening has been achieved.
Flexor Carpi Ulnaris (FCU) to Extensor Carpi Radialis Longus (ECRL) Transfer
The FCU is frequently the primary deforming force driving wrist flexion and ulnar deviation. Transferring the FCU to the ECRL (a variation of the classic Green transfer) removes this deforming force and repurposes it to provide robust, active wrist extension and radial deviation, which helps center the hand on the forearm.
* Harvesting the FCU: The FCU tendon is identified at its insertion on the pisiform through a small distal incision. It is sharply detached and mobilized proximally into the main forearm wound. The surgeon must carefully dissect the FCU off the underlying ulnar nerve and artery. The fascial compartments are released proximally to the proximal third of the forearm to ensure a straight line of pull.
* Routing the Transfer: A large subcutaneous tunnel is created around the ulnar border of the forearm, directed toward the dorsal aspect of the wrist. The tunnel must be capacious to prevent any mechanical tethering of the transferred muscle belly.
* Fixation and Weaving: A dorsal transverse incision is made over the base of the second metacarpal to identify the ECRL tendon. The FCU tendon is passed through the subcutaneous tunnel. A classic Pulvertaft weave is utilized, passing the FCU through the ECRL tendon at least three times at 90-degree angles to one another.
* Tensioning: This is the most critical step. The transfer is tensioned with the forearm in neutral rotation, the wrist held in approximately 30° to 45° of extension, and the fingers allowed to rest in slight flexion. The weave is secured with multiple figure-of-eight stitches using 3-0 non-absorbable braided suture.
Thumb-in-Palm Reconstruction
Correcting the thumb-in-palm deformity is essential for restoring functional pinch kinematics.
* Intrinsic Release: A palmar incision is made parallel to the thenar crease. The neurovascular bundles to the thumb are identified and protected. The origin of the transverse head of the adductor pollicis is released from the third metacarpal shaft. If tightness persists, the oblique head and the deep head of the FPB are fractionally released.
* Extensor Augmentation: To provide active abduction and extension, the brachioradialis (BR) is often transferred to the abductor pollicis longus (APL) or extensor pollicis longus (EPL). The BR is harvested via a radial forearm incision, mobilized proximally (releasing its fascial attachments to allow excursion), and woven into the APL/EPL using a Pulvertaft weave. Alternatively, the EPL can be rerouted out of Lister's tubercle and transposed radially to provide a more direct abduction vector.
Complications, Incidence Rates, and Salvage Management
Surgical reconstruction of the spastic upper extremity is fraught with potential complications, primarily due to the unpredictable nature of the underlying upper motor neuron lesion, the difficulty in perfectly balancing tendon transfers, and the challenges of postoperative compliance in cognitively impaired patients. The most devastating functional complication is over-lengthening of the volar flexors. If the aponeurotic cuts are made too aggressively, or if a Z-lengthening stretches out postoperatively, the patient will lose all active grip strength, rendering the hand a useless, flail appendage.
Under-correction is also common, particularly if the surgeon fails to recognize a fixed capsular contracture preoperatively and relies solely on tendon lengthening. In such cases, the spasticity often overpowers the lengthened tendons, leading to a rapid recurrence of the flexion deformity. Tendon transfer rupture or pull-out is a significant risk in the immediate postoperative period, especially if the patient experiences severe flexor spasms or dystonic posturing before the tendon weave has biologically incorporated.
Complex Regional Pain Syndrome (CRPS) and severe postoperative pain are notable risks, particularly following extensive fascial releases and nerve mobilizations. Meticulous surgical technique, avoidance of excessive traction on the median and ulnar nerves during fractional lengthening, and aggressive postoperative pain management are essential preventative measures. When complications arise, salvage management must be swift and pragmatic, often shifting from functional restoration to purely palliative or hygienic goals.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment Strategy |
|---|---|---|---|
| Over-lengthening / Loss of Grip | 5% - 10% | Aggressive complete tenotomies; Operating on dynamic spasticity in young children. | Prolonged flexor strengthening therapy; Rarely, surgical shortening or tenodesis. Often irreversible. |
| Recurrent Flexion Deformity | 15% - 25% | Unrecognized fixed capsular contracture; Under-tensioning of extensor transfers; Progressive neurological disease. | Revision fractional lengthening; Proximal row carpectomy (PRC); Total wrist arthrodesis for salvage. |
| Tendon Transfer Rupture | 2% - 5% | Severe postoperative muscle spasms; Non-compliance with cast immobilization; Poor Pulvertaft weave technique. | Immediate surgical re-exploration and revision of the tendon weave; Botulinum toxin to antagonist muscles. |
| Fixed Extension Contracture | 3% - 7% | Over-tensioning of the FCU to ECRL/ECRB transfer; Excessive flexor lengthening. | Aggressive dynamic flexion splinting; Surgical lengthening of the transferred tendon. |
| Wound Breakdown / Infection | 1% - 3% | Poor soft tissue handling; Tight subcutaneous tunnels compromising vascularity of the transferred muscle. | Local wound care; Oral or IV antibiotics; Rarely, surgical debridement and flap coverage. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of operative management in the spastic upper extremity relies as heavily on rigorous, structured postoperative rehabilitation as it does on meticulous surgical execution. The rehabilitation protocol is phased, progressive, and requires a highly specialized hand therapist experienced in neuro-orthopaedic conditions.
Phase I: Immobilization and Protection (Weeks 0 to 4)
Immediately postoperatively, the upper extremity is immobilized in a custom, well-padded long-arm bivalved cast or rigid orthosis. The positioning is critical to protect the tendon transfers and lengthenings without placing undue tension on the neurovascular structures. The elbow is typically positioned at 90° of flexion, the forearm in neutral to slight supination, the wrist in 30° to 40° of extension, the MCP joints in slight flexion, and the thumb in wide palmar abduction. During this phase, the primary goals are strict elevation to control edema, pain management, and the prevention of tendon transfer pull-out. No active or passive motion of the operated joints is permitted.

Phase II: Early Mobilization and Cortical Re-education (Weeks 4 to 8)
At four weeks, the rigid cast is removed, and a custom thermoplastic removable splint is fabricated in the identical protective position. The splint is worn full-time, removed only for supervised therapy sessions. This phase focuses on cortical re-education. The patient must be taught to fire the transferred muscle (e.g., the FCU) in its new functional role (wrist extension). This is an immense cognitive challenge, as the FCU is a native flexor. Therapists utilize biofeedback, functional electrical stimulation (FES) applied to the transferred muscle belly, and mirror visual feedback therapy to facilitate neuroplasticity and motor relearning. Active-assisted motion is initiated, strictly avoiding any passive stretching that could elongate the healing tendon weaves.
Phase III: Strengthening and Functional Integration (Weeks 8 to 12+)
By the eighth postoperative week, the tendon transfers have achieved sufficient tensile strength to withstand progressive loading. The protective splint is gradually weaned during the day, transitioning to a functional orthosis, though night splinting is often maintained for 6 to 12 months to prevent recurrence of myostatic contractures. Therapy shifts toward strengthening the transferred muscles, improving endurance, and integrating the newly reconstructed limb into bimanual activities of daily living. Constraint-induced movement therapy (CIMT)—where the unaffected limb is temporarily immobilized to force the use of the reconstructed limb—can be highly effective in overcoming residual learned nonuse and maximizing the functional outcome of the surgical reconstruction.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for the spastic upper extremity is deeply rooted in several decades of landmark orthopaedic literature. Seminal works by Green and Banks in the 1960s established the foundation for tendon transfers in cerebral palsy, specifically popularizing the FCU to ECRB/ECRL transfer to restore active wrist extension while simultaneously removing the primary deforming flexor force. Their long-term follow-up studies demonstrated that successful transfer relies entirely on the presence of selective motor control and adequate preoperative sensibility.
Zancolli's structural classification of the spastic wrist, published in the 1970s, remains the absolute gold standard for surgical decision-making. Zancolli elegantly demonstrated that differentiating between the ability to extend the fingers with the wrist flexed versus extended directly correlates with the degree of extrinsic flexor tightness, thereby dictating the precise level of aponeurotic lengthening required. Similarly, House's classification of the thumb-in-palm deformity provided a reproducible anatomical roadmap for addressing the complex interplay of intrinsic and extrinsic spasticity that destroys the first web space.
Contemporary clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) emphasize a multidisciplinary, stepwise approach. Current consensus dictates that surgical intervention for dynamic deformities should generally be delayed until the child reaches at least 5 to 6 years of age to allow for maximal neurological maturation and accurate assessment of voluntary motor control. Prior to this age, aggressive nonoperative management with BoNT-A and dynamic orthoses is the standard of care. Furthermore, modern literature heavily emphasizes the critical role of the hand therapist; studies by Waters and others have definitively shown that surgical outcomes are significantly inferior in patient cohorts lacking access to structured, specialized postoperative neuro-rehabilitation.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr.
---
