INTRODUCTION TO MULTIDIRECTIONAL INSTABILITY
Multidirectional instability (MDI) of the shoulder is a complex clinical entity defined by symptomatic glenohumeral subluxation or dislocation in more than one direction—typically anterior, posterior, and inferior. Unlike traumatic, unidirectional instability (TUBS: Traumatic, Unidirectional, Bankart, Surgery), MDI is classically characterized by the AMBRI acronym (Atraumatic, Multidirectional, Bilateral, Rehabilitation, Inferior capsular shift). The underlying pathoanatomy involves a redundant joint capsule, a patulous inferior glenohumeral ligament (IGHL) complex, and often an enlarged rotator interval.
Historically, the gold standard for surgical intervention was the open inferior capsular shift, which involved incising the capsule and physically overlapping (shifting) one capsular leaf over the other to reduce overall volume. However, advancements in arthroscopic techniques have revolutionized the management of MDI. Capsular laxity producing unidirectional and multidirectional instability may now be successfully treated arthroscopically with plication or a shift procedure in one or more quadrants of the shoulder.
Extensive clinical outcome studies demonstrate that the results of arthroscopic capsular volume reduction are highly comparable with open techniques. Although the exact capsular reinforcement achieved by the open shifting of one leaf over the other is not perfectly replicated in a closed environment, arthroscopic plication effectively restores capsular tension and joint kinematics with significantly less surgical morbidity, reduced postoperative pain, and preservation of the subscapularis muscle.
Clinical Pearl: The primary indication for surgical intervention in MDI is persistent, symptomatic instability that has failed a rigorous, well-supervised conservative rehabilitation program lasting a minimum of 6 to 12 months. Surgery is rarely the first-line treatment for atraumatic MDI.
BIOMECHANICS AND PATHOANATOMY
Understanding the biomechanics of the glenohumeral joint is paramount for successful capsulolabral reconstruction. The stability of the shoulder relies on a delicate interplay between static stabilizers (the glenoid labrum, articular congruity, and the capsuloligamentous complex) and dynamic stabilizers (the rotator cuff and periscapular musculature).
In the MDI patient, the static stabilizers are inherently compromised. The IGHL complex, which acts as a hammock supporting the humeral head during abduction and rotation, is abnormally elongated. This redundancy increases the capsular volume, allowing the humeral head to translate excessively across the glenoid face. Furthermore, a widened rotator interval—the triangular space bordered by the supraspinatus superiorly, the subscapularis inferiorly, and the coracoid medially—contributes significantly to inferior and posterior instability.
PREOPERATIVE EVALUATION AND INDICATIONS
Clinical Examination
A thorough physical examination under anesthesia (EUA) is a critical first step in the operating room to confirm the diagnosis and dictate the extent of the capsular shift.
* Load and Shift Test: Assesses anterior and posterior translation. Translation to the glenoid rim is Grade 1; over the rim with spontaneous reduction is Grade 2; locking out over the rim is Grade 3.
* Sulcus Sign: Evaluates inferior laxity. A downward pull on the humerus creates a dimple (sulcus) beneath the acromion. A 2+ to 3+ sulcus sign (indicating 2 to 3 cm of inferior translation) is pathognomonic for significant inferior capsular redundancy and mandates a rotator interval closure.
Surgical Indications
Arthroscopic capsular plication is indicated for:
1. Symptomatic MDI failing prolonged physical therapy.
2. Inability to perform activities of daily living or sports due to apprehension or recurrent subluxation.
3. Concomitant intra-articular pathology (e.g., labral tears, SLAP lesions) exacerbating the instability.
ARTHROSCOPIC CAPSULAR PLICATION AND SHIFT
Patient Positioning and Setup
The procedure can be performed in either the beach-chair or lateral decubitus position. The lateral decubitus position is often preferred for MDI as longitudinal and lateral traction expands the glenohumeral joint, providing unparalleled visualization of the inferior capsule and axillary pouch.
Standard portals include:
* Standard Posterior Portal: Primary viewing portal.
* Anterosuperior Portal: Located in the rotator interval, used for instrumentation and fluid management.
* Anteroinferior Portal: Placed just above the subscapularis tendon for anchor placement and suture management.
* Accessory Posterior or Posteroinferior Portal (7 o'clock): Essential for posterior capsular plication and posterior labral repairs.
Step-by-Step Surgical Technique
1. Diagnostic Arthroscopy and Tissue Preparation
A comprehensive diagnostic sweep is performed to assess capsular volume, labral integrity, and the presence of any avulsion lesions. To ensure robust tissue healing, the capsulolabral junction and the adjacent glenoid neck must be meticulously prepared. A motorized shaver and an arthroscopic rasp are used to decorticate the glenoid neck until a bleeding bone bed is achieved.
2. The Capsular Shift Procedure
The goal of the arthroscopic shift is to reduce capsular volume by advancing the redundant capsule superiorly and medially onto the labrum and glenoid. The capsule is shifted along the entire inferior glenohumeral ligament from the 3 o’clock to the 9 o’clock position.
- Using a suture-passing device (e.g., a Spectrum or a shuttle relay), the surgeon takes a substantial bite of the capsule approximately 1 to 1.5 cm inferior and lateral to the labrum.
- The suture is then passed through or around the intact labrum.
- When the knot is tied, the capsule is drawn superiorly (the "shift") and medially (the "plication"), effectively obliterating the redundant axillary pouch.
- This process is repeated sequentially, typically starting posteroinferiorly (at the 7 or 8 o'clock position) and advancing anteriorly to the 3 o'clock position.
Surgical Warning: When taking deep capsular bites at the 6 o'clock position (the axillary pouch), the surgeon must be acutely aware of the axillary nerve, which lies in close proximity (often within 2 to 5 mm) to the inferior capsule. Avoid plunging instruments blindly into the inferior recess.
3. Rotator Interval Closure
When anteroinferior instability with a 2+ to 3+ sulcus sign is present, a rotator interval closure is mandatory. This step addresses the superior capsular laxity that permits inferior translation.
* The capsule and superior glenohumeral ligament (SGHL) adjacent to the supraspinatus are approximated to the middle glenohumeral ligament (MGHL) and capsule adjacent to the subscapularis.
* This is typically performed using a non-absorbable suture passed in a U-shaped or mattress configuration.
* The knot is tied blindly outside the capsule or using an intra-articular knot-tying technique, effectively imbricating the interval and eliminating the sulcus sign.
POSTERIOR INSTABILITY AND LABRAL REPAIR
In many overhead athletes, such as pitchers, MDI is complicated by posterior labral detachment or posterior capsular redundancy. The posterior band of the IGHL is critical for resisting posterior translation during the follow-through phase of throwing.

FIGURE 52-27 A: Posterior labral detachment shown by easily passing a probe under the labrum and down the glenoid neck. This indicates a loss of the primary static posterior stabilizer.
To restore stability, the posterior labrum must be mobilized, the glenoid neck decorticated, and the labrum repaired using suture anchors.
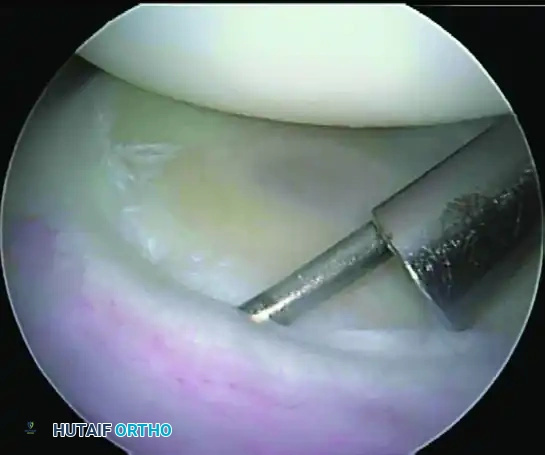
FIGURE 52-27 B: Finished suture anchor repair shows restored tension to the posterior band of the glenohumeral ligament. The capsular tissue is incorporated into the anchor repair to provide a simultaneous posterior capsular shift.
In elite throwing athletes, the posterior labral tissue can become highly attenuated or hypertrophied due to repetitive microtrauma.

FIGURE 52-28 A: Posterior labral tissue in a pitcher, demonstrating the typical fraying and detachment seen in the overhead athlete.
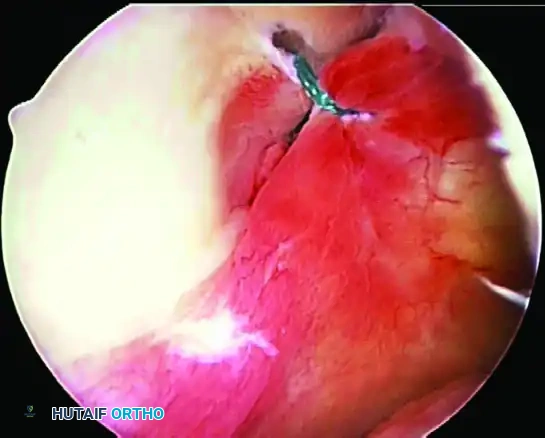
FIGURE 52-28 B: Finished repair using suture anchors to ensure firm fixation. The anchors are placed precisely on the articular margin to recreate the labral bumper effect.
HUMERAL AND GLENOID AVULSION OF THE INFERIOR GLENOHUMERAL LIGAMENT (HAGL AND GAGL)
While capsular mid-substance laxity is the hallmark of MDI, surgeons must maintain a high index of suspicion for avulsion injuries of the IGHL complex. Failure to recognize and repair a HAGL or GAGL lesion is a primary cause of recurrent instability following an otherwise successful capsular plication.
HAGL Lesions (Humeral Avulsion of the Glenohumeral Ligament)
A HAGL lesion occurs when the IGHL is avulsed from its anatomical insertion on the anatomical neck of the humerus. This creates a massive defect in the capsular hammock, allowing profound inferior and anterior (or posterior) translation.
Surgical Management of HAGL Lesions:
* Anterior HAGL Lesions: These are often technically demanding to repair arthroscopically due to the acute angle of approach to the inferior humeral neck. Therefore, anterior lesions can be most easily repaired with a mini-open technique. This involves a limited deltopectoral approach, identifying the lower border of the subscapularis, and repairing the avulsed capsule directly to the humeral neck using suture anchors.
* Posterior HAGL Lesions: Posterior lesions can be effectively repaired arthroscopically using dual posterior portals. A posteroinferior portal (7 o'clock) is established to allow the correct trajectory for anchor placement into the posterior humeral neck.
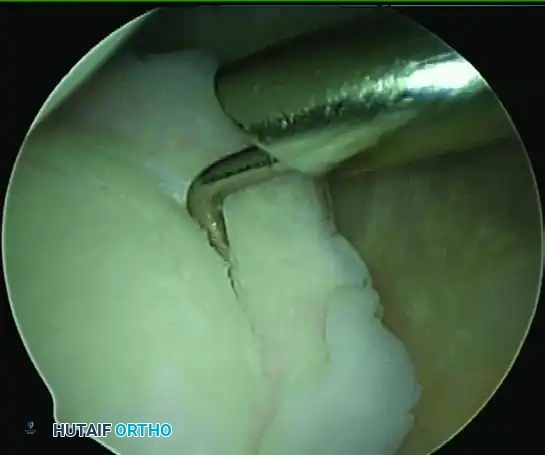
FIGURE 52-28 C: Posterior HAGL lesion repaired with a suture anchor in the humeral neck and side-to-side capsular sutures.
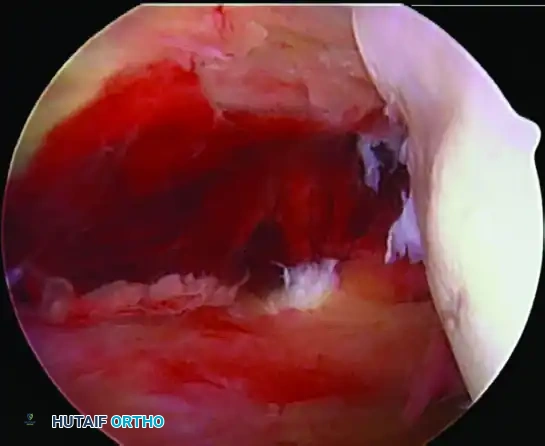
FIGURE 52-28 D: Further visualization of the posterior HAGL lesion repaired with a suture anchor in the humeral neck and side-to-side capsular sutures, demonstrating the restoration of the posterior capsular sling.
GAGL Lesions (Glenoid Avulsion of the Glenohumeral Ligament)
A GAGL lesion is less common than a Bankart lesion. In a GAGL, the labrum remains firmly attached to the glenoid bone, but the anterior inferior glenohumeral ligament is avulsed directly from the labrum itself.
Surgical Management of GAGL Lesions:
The glenoid avulsion of the anterior inferior glenohumeral ligament must be meticulously visualized. Because the labrum is usually stable, the surgical objective is to repair the capsule back to the intact labrum.
1. Tissue Penetration: The glenoid avulsion of the glenohumeral ligament is repaired back to a stable labrum using a Spectrum suture passer (or similar curved tissue penetrator) to pass a No. 1 PDS (polydioxanone) suture through the avulsed capsule.
2. Suture Management: The suture is then passed through the stable labral tissue.
3. Fixation: Repair the capsule to the labrum utilizing a technique similar to the standard plication procedure. The knots are tied to securely approximate the ligamentous tissue to the labral footprint, restoring the tension of the IGHL complex.
Clinical Pearl: When repairing a GAGL lesion, ensure that the capsular bite is taken far enough laterally to eliminate redundancy, effectively combining the GAGL repair with an anterior capsular shift.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of arthroscopic management for MDI and HAGL/GAGL lesions is heavily dependent on strict adherence to a phased postoperative rehabilitation protocol. Because the primary pathology is generalized tissue laxity, the rehabilitation must be more conservative than that for a standard traumatic Bankart repair.
Phase I: Maximum Protection (Weeks 0 to 6)
- Immobilization: The patient is placed in a shoulder immobilizer or sling with an abduction pillow for 4 to 6 weeks.
- Range of Motion (ROM): Passive ROM is initiated early but strictly limited. Forward flexion is limited to 90 degrees. External rotation is restricted to neutral (0 degrees) to protect the anterior capsular shift and rotator interval closure.
- Exercises: Pendulum exercises, elbow/wrist/hand active ROM, and submaximal isometric exercises for the deltoid and periscapular muscles.
Phase II: Moderate Protection and Active Motion (Weeks 6 to 12)
- Sling Weaning: The sling is discontinued at 6 weeks.
- ROM Progression: Active-assisted and active ROM exercises are initiated. The goal is to achieve full forward flexion by 10 weeks. External rotation is gradually progressed by 10 to 15 degrees per week.
- Strengthening: Isotonic strengthening of the rotator cuff and scapular stabilizers (rhomboids, serratus anterior, trapezius) begins. Emphasis is placed on closed-kinetic-chain exercises to promote dynamic joint stability and proprioception.
Phase III: Advanced Strengthening (Months 3 to 5)
- ROM: Full, symmetric ROM should be achieved by month 3. If mild stiffness persists, it is generally tolerated and even preferred in the MDI population to prevent recurrent laxity.
- Strengthening: Progression to advanced resistive exercises, plyometrics, and proprioceptive neuromuscular facilitation (PNF) patterns.
Phase IV: Return to Sport/Activity (Months 6 to 9)
- Criteria for Return: Pain-free full ROM, normal scapulohumeral rhythm, and isokinetic strength testing demonstrating at least 90% strength compared to the contralateral shoulder.
- Sport-Specific Training: Interval throwing programs for overhead athletes, or specific functional drills for contact athletes, are initiated. Return to competitive play is typically permitted between 6 and 9 months postoperatively, depending on the patient's progress and the demands of their specific sport.
COMPLICATIONS AND PITFALLS
While arthroscopic management of MDI is highly successful, complications can arise:
* Recurrent Instability: The most common complication, often due to unrecognized HAGL lesions, inadequate capsular shift, or failure of the patient to comply with postoperative restrictions.
* Over-constraint and Stiffness: Taking excessively large capsular bites or over-tightening the rotator interval can lead to severe loss of external rotation. A delicate balance must be struck between eliminating laxity and preserving functional motion.
* Nerve Injury: The axillary nerve is at highest risk during the 6 o'clock capsular plication. The musculocutaneous nerve is at risk during anterior portal placement and mini-open anterior HAGL repairs.
* Chondrolysis: Historically associated with intra-articular pain pumps or prominent knot stacks abrading the articular cartilage. The use of knotless anchors and avoiding intra-articular local anesthetic infusions has largely mitigated this risk.
By adhering to strict biomechanical principles, ensuring meticulous tissue preparation, and executing a precise, quadrant-by-quadrant capsular shift, the orthopedic surgeon can achieve excellent, reproducible outcomes in the complex management of multidirectional shoulder instability.
