Introduction to Minimally Invasive Plating of Tibial Pilon Fractures
The management of tibial pilon fractures remains one of the most formidable challenges in orthopedic trauma surgery. Historically, traditional open reduction and internal fixation (ORIF) through extensile approaches yielded high rates of wound dehiscence, deep infection, and subsequent osteomyelitis due to the tenuous soft tissue envelope surrounding the distal tibia.
To circumvent these catastrophic complications, Minimally Invasive Plate Osteosynthesis (MIPO) has emerged as a gold-standard alternative. Minimally invasive plating techniques have been significantly enhanced by the widespread development of precontoured locking-plate technology. Modern implants, particularly those featuring outriggers and radiolucent targeting guides, allow for precise proximal fixation without the need for extensive soft tissue stripping.
This comprehensive guide details the evidence-based, staged approach to tibial pilon fractures, emphasizing biomechanical principles, meticulous soft tissue management, and advanced percutaneous surgical techniques.
Biomechanics and Preoperative Planning
The fundamental philosophy of MIPO in pilon fractures relies on the concept of relative stability for the diaphyseal/metaphyseal component and absolute stability for the articular block. By utilizing a bridge plating construct, the surgeon preserves the extraperiosteal vascular network, thereby promoting secondary bone healing via callus formation in the comminuted metaphyseal region.
The "Span, Scan, and Plan" Protocol
High-energy pilon fractures are universally associated with severe soft tissue compromise. Immediate definitive fixation is contraindicated. Instead, a staged protocol is mandatory:
1. Span: Immediate application of a joint-spanning external fixator to restore length, alignment, and rotation via ligamentotaxis.
2. Scan: Post-spanning computed tomography (CT) to delineate the articular fracture pattern (e.g., Chaput, Volkmann, and medial malleolar fragments).
3. Plan: Delayed definitive reconstruction (MIPO) once the soft tissue envelope has recovered (typically 10 to 21 days post-injury).
💡 Clinical Pearl: Soft Tissue Assessment
Definitive Stage 2 reconstruction should only proceed when the soft tissues permit. The presence of the "wrinkle sign," resolution of fracture blisters, and decreased edema are critical clinical indicators that the limb is ready for surgical intervention.
STAGE 1: Initial Damage Control and External Fixation
The primary objective of Stage 1 is to stabilize the skeletal architecture, protect the soft tissues from further sheer stress, and restore the lateral column if appropriate.

Figure 54-17 A: Initial presentation of a closed, highly comminuted fracture involving the tibial pilon and fibula.
Step-by-Step Surgical Technique: Stage 1
- Patient Positioning: Place the patient supine on a radiolucent operating table. Ensure the C-arm fluoroscope can freely image the entire tibia, ankle, and foot in both AP and lateral planes.
- Preparation: Administer prophylactic intravenous antibiotics preoperatively. Apply a pneumatic thigh tourniquet (to be used only if necessary for the fibular approach).
- Fibular Management (Optional but Recommended):
- We do not routinely perform open reduction of the fibular component during the initial setting if the soft tissue is critically compromised; length can be maintained through the external fixator alone.
- However, if the lateral soft tissue envelope allows, make a standard posterolateral incision. Reduce the fibular fracture and fix it with a one-third tubular plate. This reestablishes the lateral column and aids in indirect reduction of the tibial block.
- Close the fibular wound meticulously with 3-0 nylon without tension.
- External Fixator Application:
- Construct a rigid, triangular external fixator spanning the ankle joint.
- Place two 5.0-mm Schanz pins proximally in the anteromedial aspect of the tibial diaphysis (safe zone).
- Place one centrally threaded transfixation pin through the calcaneal tuberosity, avoiding the neurovascular bundle medially.
- Reduction via Ligamentotaxis: Apply longitudinal traction. Using ligamentotaxis and the reestablished lateral column (if fixed), the pilon fracture is temporarily reduced. Lock the frame.


Figure 54-17 B and C: Application of a uniplanar spanning external fixation and fibular ORIF facilitates indirect reduction of the distal tibial comminution.
STAGE 2: Definitive Minimally Invasive Plate Osteosynthesis (MIPO)
Definitive reconstruction is undertaken once the soft tissue envelope has adequately healed. The goal is anatomic restoration of the articular surface followed by stable, biologically friendly fixation of the metadiaphysis.
Step-by-Step Surgical Technique: Stage 2
- Positioning and Setup: Place the patient supine on a radiolucent table. Apply a thigh tourniquet. Prep and drape the limb, including the external fixator.
- Articular Reduction:
- If preoperative CT planning indicates that purely percutaneous plating is impossible due to impacted articular fragments, perform a limited anterior arthrotomy.
- This limited approach allows for direct visualization of the joint surface, elevation of depressed fragments, bone grafting of metaphyseal voids, and application of a small anterior provisional plate or independent lag screws.
- Alternatively, an anterolateral surgical approach may be performed for articular reduction, followed by submuscular fixation. A medially based large distractor can facilitate this reduction.
- Plate Estimation and Contouring:
- If percutaneous plating is feasible, estimate the required length of the plate based on preoperative radiographs and fluoroscopy. The plate must span the comminuted segment adequately to provide a long working length.
- Place the selected plate on the skin and verify its position and length under fluoroscopy.
- Contour the plate to match the complex anatomy of the anteromedial distal tibia. Use plate benders to achieve the necessary bend and twist. Re-check the anticipated position fluoroscopically.
- Incision and Tunneling:
- Make one small anteromedial incision at the distal end of the anticipated plate position (often incorporating the medial malleolus) and a second small incision at the proximal end.
- Create an extraperiosteal subcutaneous tunnel connecting these two incisions. This is achieved by advancing a long Kelly clamp or specialized tunneling instrument from distal to proximal (or vice versa), staying strictly on the bone to avoid neurovascular injury (specifically the saphenous nerve and vein).


Figure 54-17 D and E: After healing of soft tissues, the patient returns for definitive fixation. The precontoured plate is inserted through a limited distal incision and advanced proximally via an extraperiosteal tunnel.
- Plate Insertion:
- Tie a strong, heavy suture (e.g., Ethibond No. 5) through the most proximal hole of the plate.
- Pass the Kelly clamp through the proximal incision, down the tunnel, and grasp the suture. Pull the plate smoothly through the subcutaneous extraperiosteal tunnel under continuous radiographic control.
- Fixation Sequence:
- Once the plate is optimally positioned, fix it distally and proximally through the small stab incisions using 3.5-mm cortical low-profile screws.
- Locking screws should be utilized if a bridge plate construct is deemed necessary, particularly in osteoporotic bone or highly comminuted patterns.
- Place a nonlocking lag screw through the midportion of the plate if fracture morphology allows. Because the plate is flexible, tightening this nonlocking screw will draw the bone to the plate, achieving excellent bone-plate contact.
- Finalization:
- Obtain final orthogonal radiographic views to confirm anatomic articular reduction, restoration of mechanical axis, and hardware placement.
- Remove the external fixator.
- Deflate the tourniquet, achieve meticulous hemostasis, and close the wounds over closed-suction drains in a standard layered fashion.

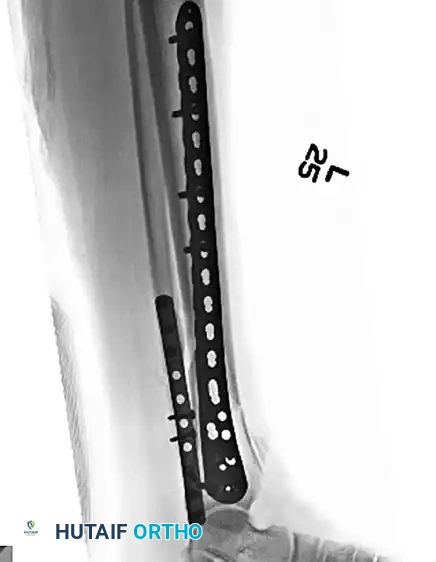
Figure 54-17 F and G: Final postoperative AP and Lateral radiographs demonstrating excellent restoration of the articular surface and stable bridge plating of the metadiaphysis.
🚨 Surgical Warning: Soft Tissue Bridging
Care must be applied to ensure adequate soft tissue bridging if a separate incision is necessary to treat the fibula. The skin bridge between a lateral fibular incision and an anterolateral or anteromedial tibial incision must be at least 7 cm to prevent catastrophic skin necrosis.
Surgical Approaches to the Distal Tibia
The choice of surgical approach is dictated by the fracture pattern (location of the primary articular comminution) and the condition of the soft tissue envelope.
The Anterolateral Approach
Described extensively in trauma literature, the anterolateral approach provides excellent visualization of the Chaput fragment and the central articular surface. It utilizes the internervous plane between the superficial peroneal nerve and the deep peroneal nerve. When the anterolateral approach is employed, a separate incision is occasionally needed to place a percutaneous small medial plate if the fracture pattern demands dual-column fixation.
The Posterolateral Approach
Alternatives to the traditional anterior approaches have been advocated to reduce the incidence of soft tissue complications. Konrath and Hopkins reported the use of a posterolateral approach, utilizing the interval between the peroneal tendons and the flexor hallucis longus (FHL).
Advantages:
* It is possible to stabilize both the tibia and the fibula through the same single incision.
* A thicker soft tissue envelope overlies the posterior plate (covered by the FHL muscle belly), which was theoretically thought to decrease problems with wound healing and deep infection.
Disadvantages:
* Poor exposure of the anterior ankle joint, severely limiting its utility in fractures with anterior comminution.
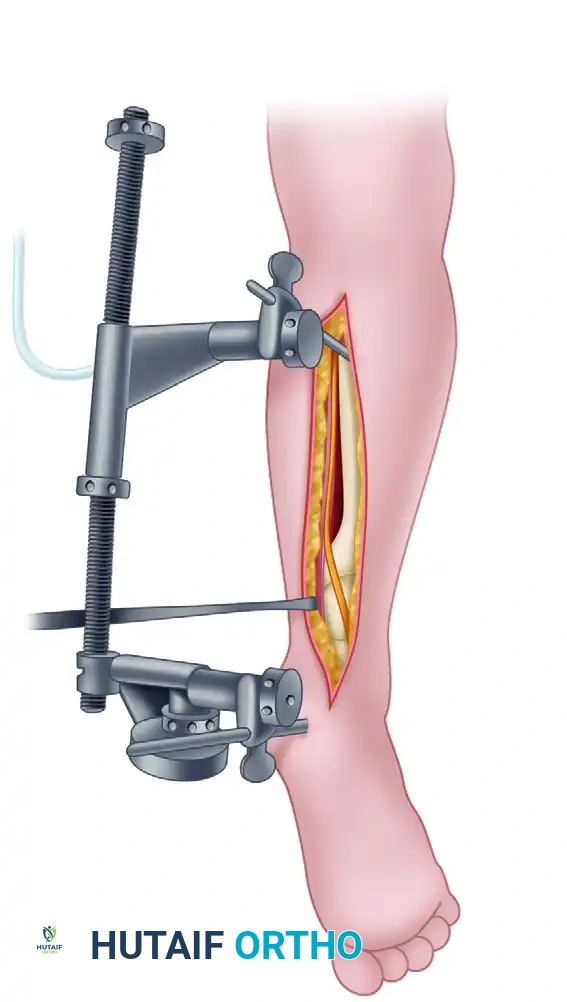
Figure 54-18: The Posterior approach. A femoral distractor has been applied to aid in visualization, and the sural nerve is meticulously dissected free and protected.
Clinical Evidence on the Posterolateral Approach:
Bhattacharyya et al. critically examined the complications associated with the posterolateral approach for pilon fractures in a cohort of 19 patients. The results challenged the assumption of superior soft tissue safety:
* Complications occurred in 9 of the 19 patients.
* Six patients (31%) experienced wound problems (three superficial infections, three deep infections).
* Four patients (21%) developed nonunions (two aseptic, two infected).
* Three patients ultimately required ankle arthrodesis, and one patient healed with a 3-mm articular step-off.
The authors concluded that the posterolateral approach did not reduce the incidence of wound complications compared with other standard approaches. Therefore, this surgical approach is recommended only for pilon fractures in which the articular displacement and comminution are predominantly located posteriorly, or when an anterior approach is strictly contraindicated due to localized anterior soft tissue compromise.
Postoperative Care and Rehabilitation
The postoperative protocol is critical to ensuring both soft tissue survival and optimal functional recovery.
- Immediate Postoperative Phase: The limb is immobilized in a bulky cotton dressing with a rigid posterior plaster splint, maintaining the ankle in a strictly neutral (90-degree) position to prevent equinus contracture.
- Drain Management: Closed suction drains, if utilized, are typically removed on postoperative day 1 or 2, depending on output.
- Mobilization: Depending on the rigidity of the fixation and the status of the soft tissues, splint immobilization is discontinued as soon as wound healing permits (usually 2 weeks).
- Range of Motion: Passive and active range of motion (ROM) exercises of the ankle and subtalar joints are initiated immediately upon splint removal to prevent arthrofibrosis.
- Wound Care: Sutures or staples are removed between 2 to 3 weeks postoperatively, contingent upon complete epithelialization.
- Weight Bearing: The patient is kept strictly non-weight bearing (NWB) on the operative extremity. Full weight bearing is not permitted until robust bony healing is confirmed radiographically, which usually occurs by 12 weeks postoperatively. Progressive partial weight bearing may be initiated between 8 to 10 weeks if bridging callus is evident.
Conclusion
Minimally invasive plating of tibial pilon fractures represents a sophisticated evolution in orthopedic trauma surgery. By respecting the delicate soft tissue envelope through a staged protocol and utilizing extraperiosteal MIPO techniques, surgeons can achieve the dual goals of anatomic articular restoration and biologic diaphyseal fixation. Mastery of preoperative planning, precise fluoroscopic anatomy, and meticulous handling of the soft tissues are paramount to minimizing complications and maximizing patient outcomes in these severe injuries.
