This article provides a detailed step-by-step guide to the minimally invasive anterolateral approach to the proximal humerus. The approach is used for the insertion of intramedullary nails for the treatment of acute humeral shaft fractures, pathologic humeral shaft fractures, and delayed union and nonunion of humeral shaft fractures.
Dr.Mohammad Hutaif
,
Emial
The minimally invasive approach to the proximal humerus is used for the insertion of intramedullary nails for the treatment of the following:
1. Acute humeral shaft fractures
2. Pathologic humeral shaft fractures
3. Delayed union and nonunion of humeral shaft fractures
The presence of the overlying acromion and the fact that the upper end of the humerus is covered entirely with articular cartilage mean that most nails are angled at their upper end and are inserted via the lateral cortex of the humerus. The entry point for an intermedullary nail into the humerus is determined radiographically, with a template of the required nail superimposed over a radiograph of the injured humerus. The entry point depends on the specific design of the nail. The most usual entry point is just lateral to the articular surface of the humeral head and just medial to the greater tuberosity (see
Fig.
1-50).
Position of the Patient
Place the patient in a supine position. Elevate the upper portion of the table to approximately 60 degrees
. Position the patient so that the shoulder lies over the edge of the table. Alternatively, use a specialized table that allows radiographic visualization of the shoulder in both anterior–posterior and lateral planes. Ensure that the cervical spine is adequately supported and that lateral flexion of the cervical spine is avoided to prevent a traction lesion of the brachial plexus.

Figure 1-46
Palpate the lateral border of the acromion and then make a 2-cm incision from that border down the lateral aspect of the arm.
Landmarks and Incision Landmark
The
acromion
is rectangular. Its bony dorsum and lateral border are easy to palpate on the outer aspect of the shoulder (see
Figs. 1-51
and
1-52).
Incision
Make a 2-cm incision from the outer aspect of the acromion down the lateral aspect of the arm (
Fig. 1-46
and see
Fig. 1-39).
Internervous Plane
This approach does not exploit an internervous plane. The dissection involves splitting the deltoid muscle.
Superficial and Deep Surgical Dissections
Insert a wire under image intensifier control through the skin incision, down through the substance of the deltoid muscle and rotator cuff to the correct insertion point on the humerus (
Fig.
1-47). This position has been determined on the preoperative x-ray plan. Confirm that the wire is in the correct position by the use of a C-arm image intensifier in both anterior–
posterior and lateral planes.

Figure 1-47 Insert a guidewire through the substance of the deltoid muscle under image intensifier control.

 Figure 1-48
Enlarge the track made by the wire using a point-ended scalpel. You will incise part of the deltoid and part of the supraspinatus tendon.
Figure 1-48
Enlarge the track made by the wire using a point-ended scalpel. You will incise part of the deltoid and part of the supraspinatus tendon.
Withdraw the wire and insert a point-ended scalpel blade, following the track of the wire using a C-arm image intensifier to confirm position (
Fig.
1-48
). Incise a small portion of the deltoid and make a small clean-edged incision through part of the supraspinatus tendon. Withdraw the blade and reinsert the wire. Enter the proximal end of the humerus using an awl or drill, depending on the nail to be used (
Figs.
1-49
and
1-50).
Dang Nerves
The
axillary nerve
lies approximately 7 cm below the tip of the acromion, running transversely on the deep aspect of the deltoid muscle.
The brachial artery and median nerve lie medial to the proximal humerus. They are also at risk during insertion of proximal locking bolts. This incision should, therefore, not risk damage to the axillary nerve (see
Fig.
1-39
). The nerve may, however, be damaged by proximal interlocking bolts inserted from lateral to medial (see
Fig.
1-50).
Tendons
Part of the
supraspinatus tendon and the overlying subacromial bursa
will be incised by this approach. A degree of damage to the rotator cuff is therefore inevitable in proximal humeral nailing using conventional nails (see
Fig.
1-39
). Damage to the rotator cuff is minimized by ensuring that any drills used are passed through protection sleeves. Formal repair of the supraspinatus tendon is important during closure of the surgical approach. Despite these maneuvers a significant degree of stiffness of the shoulder may occur postoperatively in a number of patients following antegrade humeral nailing.
36
How to Enlarge the Approach Extensile Measures
Distal Extension.
The approach can be extended to a formal lateral approach to the proximal humerus. This extension may be needed if closed reduction of proximal humeral fractures cannot be obtained (see
Fig. 1-39
).

Figure 1-49 Insert the wire into the proximal end of the humerus under image intensifier control.


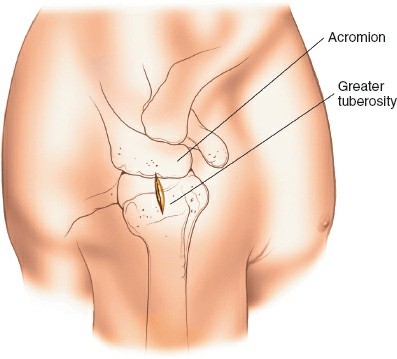
Figure 1-50 Lateral view of the shoulder, revealing insertion of the guidewire. The most common entry point is just lateral to the articular surface of the humeral head and just medial to the greater tuberosity.
Minimally Invasive Anterolateral Approach to the Proximal Humerus
Minimally Invasive Anterolateral Approach to the Proximal Humerus
What is the minimally invasive anterolateral approach to the proximal humerus used for?
- Acute humeral shaft fractures
- Pathologic humeral shaft fractures
- Delayed union and nonunion of humeral shaft fractures
What is the position of the patient for the minimally invasive anterolateral approach to the proximal humerus?
- Supine
What is the landmark for the minimally invasive anterolateral approach to the proximal humerus?
- Acromion
What is the incision for the minimally invasive anterolateral approach to the proximal humerus?
- 2 cm incision from the outer aspect of the acromion down the lateral aspect of the arm
What is the internervous plane for the minimally invasive anterolateral approach to the proximal humerus?
- Between the deltoid and the pectoralis major muscles
What is the first step in the minimally invasive anterolateral approach to the proximal humerus?
- Make a skin incision
What is the second step in the minimally invasive anterolateral approach to the proximal humerus?
- Dissect the deltoid muscle
What is the third step in the minimally invasive anterolateral approach to the proximal humerus?
-
Insert a wire through the skin incision
Figure 1-50
Lateral view of the shoulder, revealing insertion of the guidewire. The most common entry point is just lateral to the articular surface of the humeral head and just medial to the greater tuberosity.
Minimally Invasive Anterolateral Approach to the Proximal Humerus Minimally Invasive Anterolateral Approach to the Proximal Humerus What is the minimally invasive anterolateral approach to the proximal humerus used for? What is the position of the patient for the minimally invasive anterolateral approach to the proximal humerus? What is the landmark for the minimally invasive anterolateral approach to the proximal humerus? What is the incision for the minimally invasive anterolateral approach to the proximal humerus? What is the internervous plane for the minimally invasive anterolateral approach to the proximal humerus? What is the first step in the minimally invasive anterolateral approach to the proximal humerus? What is the second step in the minimally invasive anterolateral approach to the proximal humerus? What is the third step in the minimally invasive anterolateral approach to the proximal humerus? References
Court-Brown CM, Garg A, McQueen MM. The epidemiology of proximal humeral fractures. Acta Orthop Scand. 2001;72:365–371. Article PubMed CAS Google Scholar DeStatis Statistisches Bundesamt. Hospital statistics. Wiesbaden 2011; Available at: http://www.gbe-bund.de/oowa921-install/servlet/oowa/aw92/dboowasys921.xwdevkit/xwd_init?gbe.isgbetol/xs_start_neu/&p_aid=i&p_aid=36857213&nummer=702&p_sprache=D&p_indsp=522&p_aid=9442669;Download . Accessed June 14, 2012.
Duralde XA, Leddy LR. The results of ORIF of displaced unstable proximal humeral fractures using a locking plate. J Shoulder Elbow Surg. 2010;19:480–488. Article PubMed Google Scholar Fankhauser F, Boldin C, Schippinger G, Haunschmid C, Szyszkowitz R. A new locking plate for unstable fractures of the proximal humerus. Clin Orthop Relat Res. 2005;430:176–181. Article PubMed Google Scholar Gardner MJ, Griffith MH, Dines JS, Briggs SM, Weiland AJ, Lorich DG. The extended anterolateral acromial approach allows minimally invasive access to the proximal humerus. Clin Orthop Relat Res. 2005;434:123–129. Article PubMed Google Scholar Handoll HH, Ollivere BJ, Rollins KE. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev. 2012;12:CD000434. Google Scholar Acklin YP, Stoffel K, Sommer C. A prospective analysis of the functional and radiological outcomes of minimally invasive plating in proximal humerus fractures. Injury. 2013;44:456–460. Article PubMed Google Scholar Björkenheim JM, Pajarinen J, Savolainen V. Internal fixation of proximal humeral fractures with a locking compression plate: a retrospective evaluation of 72 patients followed for a minimum of 1 year. Acta Orthop Scand. 2004;75:741–745. Article PubMed Google Scholar Constant CR. [Assessment of shoulder function] [in German]. Orthopade. 1991;20:289–294. PubMed CAS Google Scholar Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;214:160–164. PubMed Google Scholar Hepp P, Theopold J, Voigt C, Engel T, Josten C, Lill H. The surgical approach for locking plate osteosynthesis of displaced proximal humeral fractures influences the functional outcome. J Shoulder Elbow Surg. 2008;17:21–28.
Röderer G, Abouelsoud M, Gebhard F, Böckers TM, Kinzl L. Minimally invasive application of the non-contact-bridging (NCB) plate to the proximal humerus: an anatomical study. J Orthop Trauma. 2007;21:621–627. Article PubMed Google Scholar Röderer G, Erhardt J, Kuster M, Vegt P, Bahrs C, Kinzl L, Gebhard F. Second generation locked plating of proximal humerus fractures—a prospective multicentre observational study. Int Orthop. 2011;35:425–432. Article PubMed Central PubMed Google Scholar Ruchholtz S, Hauk C, Lewan U, Franz D, Kühne C, Zettl R. Minimally invasive polyaxial locking plate fixation of proximal humeral fractures: a prospective study. J Trauma. 2011;71:1737–1744. Article PubMed Google Scholar Südkamp N, Bayer J, Hepp P, Voigt C, Oestern H, Kääb M, Luo C, Plecko M, Wendt K, Köstler W, Konrad G. Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Results of a prospective, multicenter, observational study. J Bone Joint Surg Am. 2009;91:1320–1328. Article PubMed Google Scholar Voigt C, Geisler A, Hepp P, Schulz AP, Lill H. Are polyaxially locked screws advantageous in the plate osteosynthesis of proximal humeral fractures in the elderly? A prospective randomized clinical observational study. J Orthop Trauma. 2011;25:596–602. Article PubMed Google Scholar Warriner AH, Patkar NM, Curtis JR, Delzell E, Gary L, Kilgore M, Saag K. Which fractures are most attributable to osteoporosis? J Clin Epidemiol. 2011;64:46–53. Article PubMed Google Scholar Wu CH, Ma CH, Yeh JJ, Yen CY, Yu SW, Tu YK. Locked plating for proximal humeral fractures: differences between the deltopectoral and deltoid-splitting approaches. J Trauma. 2011;71:1364–1370 Article PubMed Google Scholar Article PubMed Google Scholar Kim SH, Szabo RM, Marder RA. Epidemiology of humerus fractures in the United States: nationwide emergency department sample, 2008. Arthritis Care Res (Hoboken). 2012;64:407–414.
Article PubMed Google Scholar Königshausen M, Kübler L, Godry H, Citak M, Schildhauer TA, Seybold D. Clinical outcome and complications using a polyaxial locking plate in the treatment of displaced proximal humerus fractures. A reliable system? Injury. 2012;43:223–231. Article PubMed Google Scholar Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179–186. Article PubMed CAS Google Scholar Neer CS. Displaced proximal humeral fractures. I. Classification and evaluation. J Bone Joint Surg Am. 1970;52:1077–1089. PubMed Google Scholar
