THE MCLAUGHLIN PROCEDURE FOR POSTERIOR SHOULDER INSTABILITY
Posterior shoulder dislocations account for a small fraction of all glenohumeral dislocations but are frequently associated with significant osseous defects of the anterior humeral head, known as reverse Hill-Sachs lesions. When these impaction fractures are large, they engage the posterior glenoid rim during internal rotation, flexion, and adduction, leading to recurrent posterior instability.
To address this, Harrison McLaughlin originally described the transfer of the subscapularis tendon directly into the anterior defect to prevent glenoid engagement. This concept was later refined by Neer and Foster, who recognized the biomechanical and biological advantages of transferring the subscapularis tendon along with its bony insertion on the lesser tuberosity.
Indications and Biomechanics
The primary indication for the McLaughlin procedure (and its modifications) is recurrent posterior shoulder instability driven by an engaging reverse Hill-Sachs lesion that involves 20% to 25% of the articular surface.
Clinical Pearl: Defects involving less than 20% of the articular surface may often be managed non-operatively or with arthroscopic soft-tissue stabilization (e.g., reverse remplissage). Defects exceeding 40% to 50% typically require structural allograft reconstruction (e.g., femoral head or proximal humerus allograft) or prosthetic arthroplasty, as a tuberosity transfer will not restore sufficient articular congruity.
By transferring the lesser tuberosity into the defect, the surgeon achieves two critical biomechanical objectives:
1. Defect Filling: The osseous void is physically occupied, preventing the posterior glenoid rim from dropping into the defect during provocative maneuvers.
2. Dynamic Sling Effect: The rerouted subscapularis acts as a dynamic tether, limiting excessive internal rotation and providing an anterior restraint that stabilizes the humeral head against the glenoid.
Surgical Approach and Technique (Neer-Foster Modification)
The procedure is performed with the patient in the beach-chair position, ensuring the arm can be freely manipulated.
- Incision and Approach: A standard deltopectoral approach is utilized. The cephalic vein is identified and retracted laterally with the deltoid to preserve its drainage. The clavipectoral fascia is incised, and the conjoined tendon is retracted medially.
- Nerve Identification: The axillary nerve must be palpated and protected inferior to the subscapularis border. The musculocutaneous nerve is protected medially.
- Osteotomy: The boundaries of the lesser tuberosity are defined. An osteotome or oscillating saw is used to perform a vertical osteotomy, freeing the lesser tuberosity with the attached subscapularis tendon.
- Defect Preparation: The reverse Hill-Sachs lesion is identified on the anteromedial humeral head. The defect is debrided of fibrous tissue, and the base is decorticated to bleeding cancellous bone to promote osteointegration.
- Transfer and Fixation: The lesser tuberosity is mobilized and impacted into the prepared defect. It is secured using two fully threaded cancellous bone screws with washers.
- Closure: The rotator interval is closed, and the deltopectoral interval is approximated.
Postoperative Rehabilitation
Postoperative immobilization is critical to protect the bony transfer. The arm is placed in a neutral to slightly externally rotated orthosis (10 to 20 degrees of external rotation) for 6 weeks. Passive range of motion (ROM) emphasizing external rotation and elevation begins at 2 weeks, strictly avoiding internal rotation behind the back. Active ROM and progressive strengthening commence at 6 weeks, following radiographic confirmation of tuberosity union.
ARTHROSCOPIC ADVANCES IN SHOULDER INSTABILITY
Arthroscopic repair of shoulder instability represents an area of exponential growth and continuous technical refinement. As instrumentation and surgical acumen have evolved, arthroscopic outcomes have improved dramatically, now matching—and in cases of isolated capsulolabral pathology, surpassing—the results of traditional open techniques.
For posterior instability, arthroscopic posterior labral repair combined with a "reverse remplissage" (arthroscopic tenodesis of the subscapularis into the reverse Hill-Sachs defect) has become a viable, minimally invasive alternative to the open McLaughlin procedure for moderate-sized defects. Arthroscopic management minimizes subscapularis morbidity, reduces postoperative stiffness, and allows for concurrent management of intra-articular pathology.
ELBOW DISLOCATION AND COMPLEX INSTABILITY
Acute dislocation of the elbow is a high-energy traumatic event, accounting for approximately 28% of all elbow injuries. The elbow is the second most commonly dislocated major joint in adults, following the shoulder. Because of the profound soft tissue disruption required to dislocate the highly congruent ulnohumeral joint, residual loss of motion (stiffness) is the most common complication.
Recurrent dislocation of the elbow is exceedingly rare. In a landmark series of 110 elbow dislocations by Linscheid and Wheeler, only two cases of recurrent dislocation were identified. However, while frank recurrent dislocation is rare, the persistence of subtle posterolateral rotatory instability (PLRI) or medial (valgus) instability is far more common. When symptomatic, these micro-instability patterns cause significant functional impairment and require surgical reconstruction.
SURGICAL ANATOMY OF THE ELBOW
Elbow stability relies on a complex interplay between static osseous congruity, static ligamentous restraints, and dynamic muscular stabilizers. The primary static stabilizers are the ulnohumeral articulation, the medial collateral ligament (MCL) complex, and the lateral collateral ligament (LCL) complex.
The Lateral Collateral Ligament Complex
The LCL complex originates from the lateral epicondyle and is the primary restraint to varus and posterolateral rotatory stress. It consists of four components: the radial collateral ligament, the annular ligament, the accessory lateral collateral ligament, and the lateral ulnar collateral ligament (LUCL).
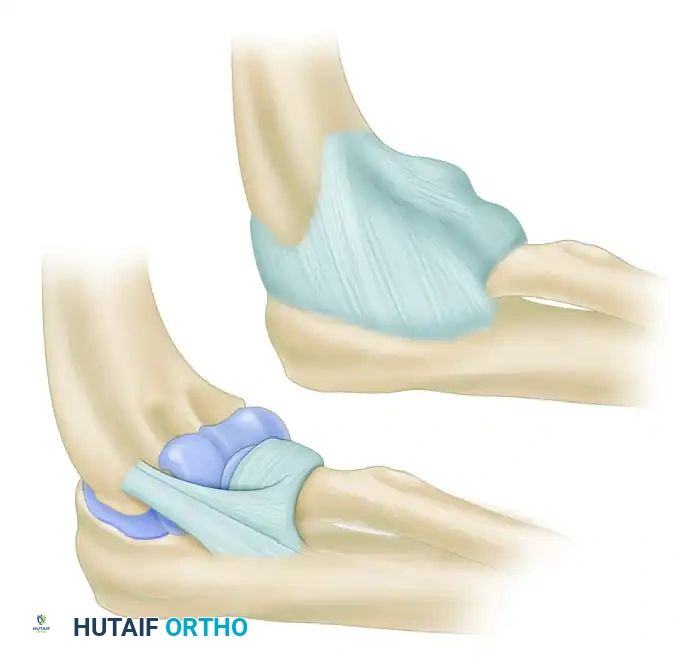
The LUCL is the most critical structure for posterolateral stability. It arises from the lateral epicondyle, blends with the fibers of the annular ligament, and courses distally and posteriorly to insert on the supinator crest of the proximal ulna.
Surgical Warning: The LUCL acts as a hammock supporting the radial head. It remains taut in both flexion and extension. Disruption of the LUCL allows the radial head to subluxate posteriorly relative to the capitellum, resulting in the classic pivot-shift phenomenon of posterolateral rotatory instability (PLRI).
Biomechanically, the LCL complex contributes only 14% of the varus stability of the elbow with the joint in full extension, and only 9% with the joint in 90 degrees of flexion. The vast majority of varus stability is conferred by the osseous architecture of the ulnohumeral joint and the anterior capsule.
The Medial Collateral Ligament Complex
The MCL complex is a robust, well-developed structure that serves as the primary restraint to valgus stress. It is divided into three distinct bundles: the anterior oblique, posterior oblique, and transverse oblique ligaments.

- Anterior Bundle (AMCL): The anterior bundle is the most important stabilizer of the elbow against valgus stress. It originates from the anteroinferior surface of the medial epicondyle and inserts on the sublime tubercle of the anteromedial coronoid process. It is functionally divided into two nonisometric bands:
- Anterior Band: Taut from 0 to 60 degrees of flexion.
- Posterior Band: Taut from 60 to 120 degrees of flexion.
- Posterior Bundle: Originates from the medial epicondyle and inserts on the medial margin of the semilunar notch. It forms the floor of the cubital tunnel and is taut in flexion beyond 90 degrees.
- Transverse Bundle (Cooper's Ligament): Originates and inserts on the ulna (olecranon to coronoid). It does not cross the elbow joint and contributes little to no significant stability.
In full extension, valgus stability is divided equally among the MCL, the anterior capsule, and the bony articulation. However, at 90 degrees of flexion, the anterior capsule is lax, and the AMCL becomes the dominant restraint, providing 55% of the resistance to valgus stress.
PATHOPHYSIOLOGY OF ELBOW INSTABILITY
Elbow instability exists on a spectrum and may be classified as congenital, traumatic, or attritional. The primary stabilizers (AMCL and LUCL) work in concert with secondary stabilizers (capsule, radiocapitellar joint, dynamic muscle-tendon units). Insufficiency in any of these structures alters joint kinematics, leading to increased stress on the remaining stabilizers, capsular contracture, chondromalacia, and osteophyte formation.
Traumatic Dislocation (The Horii Circle)
O'Driscoll et al. described a predictable, sequential pattern of soft tissue disruption during traumatic elbow dislocation, known as the Horii circle. The typical mechanism involves a fall on an outstretched, slightly flexed extremity, imparting an axial load, valgus stress, and external rotatory force (internal rotation of the humerus on a fixed, pronated forearm).
Soft tissue disruption progresses in a circular fashion from lateral to medial:
* Stage 1: Disruption of the LUCL, resulting in PLRI. The elbow subluxates but does not fully dislocate.
* Stage 2: Disruption progresses anteriorly and posteriorly through the capsule. The coronoid perches on the trochlea.
* Stage 3: Disruption of the medial structures.
* Stage 3A: The posterior band of the MCL is torn, but the anterior band remains intact. The elbow dislocates but is stable to valgus stress in flexion.
* Stage 3B: The entire MCL complex is torn. The elbow is grossly unstable.
* Stage 3C: The entire distal humerus is stripped of soft tissues.
In a long-term follow-up study of simple elbow dislocations, Anakwe et al. demonstrated that 60% of patients suffered residual stiffness (primarily loss of terminal extension) and chronic pain, while only 8% exhibited functional instability. However, when dislocations are associated with fractures of the radial head or coronoid (the "terrible triad"), the loss of secondary osseous stabilizers drastically increases the risk of recurrent instability and severe arthrosis.
Attritional Valgus Instability in the Overhead Athlete
Valgus instability resulting from attritional microtrauma to the AMCL is the most common form of recurrent elbow instability, predominantly affecting overhead throwing athletes (e.g., baseball pitchers, javelin throwers).
During the late cocking and early acceleration phases of throwing, the elbow experiences extreme valgus torque. Biomechanical studies indicate that up to 60 Newtons (N) of force is applied to the AMCL during a fastball pitch. This force closely approaches the ultimate tensile failure point of the native ligament.
Pitcher fatigue, poor kinetic chain mechanics, or sheer repetitive overuse leads to microtearing of the anterior bundle. As the primary stabilizer fails, secondary stabilizers are overloaded. This results in:
1. Radiocapitellar Compression: Chondromalacia and loose body formation in the lateral compartment.
2. Valgus Extension Overload (VEO): The olecranon is forcefully wedged into the posteromedial olecranon fossa, leading to reactive osteophyte formation, loose bodies, and fixed flexion contractures.
3. Ulnar Neuritis: Traction, scarring, or osteophyte impingement compromises the ulnar nerve within the cubital tunnel.
CLINICAL EVALUATION AND PROVOCATIVE TESTING
A meticulous clinical examination is paramount. The elbow is inspected for carrying angle and resting posture. Bony landmarks are palpated for localized tenderness. Tenderness 2 to 3 cm distal to the olecranon tip in a throwing athlete may indicate an olecranon stress fracture rather than ligamentous pathology.
Assessing Medial (Valgus) Instability
Active and passive ROM must be recorded. Valgus stress is applied to the elbow with the forearm in both supinated and pronated positions, with the elbow unlocked in approximately 30 degrees of flexion to disengage the olecranon from its fossa. The examiner must quantify the amount of medial opening, assess the firmness of the end point, and note the reproduction of medial pain.
- Moving Valgus Stress Test (O'Driscoll): The patient's shoulder is abducted to 90 degrees and externally rotated. The examiner applies a constant valgus torque to the elbow while rapidly flexing and extending the joint. Reproduction of medial pain between 70 and 120 degrees of flexion is highly sensitive and specific for AMCL insufficiency.
- Valgus Extension Overload Test: A valgus stress is maintained while the elbow is passively forced into terminal extension. Reproduction of pain along the posteromedial aspect of the olecranon indicates posteromedial impingement secondary to chronic valgus instability.
Assessing Posterolateral Rotatory Instability (PLRI)
Diagnosis of PLRI requires demonstration of radial head subluxation.
- Lateral Pivot-Shift Test: The patient is placed supine with the arm overhead. The examiner applies an axial load, valgus stress, and supination force to the forearm while slowly flexing the elbow from a fully extended position. In a positive test, the radial head subluxates posterolaterally, creating a visible dimple proximal to the radial head. As flexion reaches approximately 40 degrees, the triceps and capsule abruptly pull the radial head back into the joint, creating a palpable and visible "clunk."
Clinical Pearl: The pivot-shift test is often difficult to perform in the awake patient due to muscular guarding. The "Chair Test" or "Push-up Test," where the patient attempts to rise from a chair with the forearms supinated and elbows extended, can reliably reproduce apprehension and lateral pain, serving as an excellent surrogate marker for LUCL deficiency in the clinic.
