Bone and Joint Management in Replantation Surgery
Key Takeaway
Effective bone and joint management is the foundation of successful limb and digit replantation. This guide details critical techniques, including precise bone shortening to enable tension-free neurovascular anastomoses, and rigid skeletal fixation using Kirschner wires, intraosseous loops, or plates. By mastering these evidence-based protocols, orthopedic surgeons can optimize functional recovery, minimize nonunion rates, and ensure the viability of replanted extremities across varying levels of amputation.
PRINCIPLES OF SKELETAL MANAGEMENT IN REPLANTATION
The management of bones and joints during replantation surgery dictates the functional outcome and survival of the amputated part. Establishing a rigid, stable skeletal framework is the mandatory first step following meticulous débridement. Without absolute skeletal stability, subsequent microvascular anastomoses and neurorrhaphies are subjected to catastrophic shear forces, leading to thrombosis and replant failure.
The overarching goals of skeletal management in replantation include:
* Rapid and Rigid Fixation: To protect delicate microvascular repairs.
* Anatomic Alignment: Restoring axial and rotational alignment to optimize tendon excursion and joint kinematics.
* Strategic Bone Shortening: To allow tension-free repair of soft tissues, nerves, and vessels.
* Preservation of Biology: Minimizing periosteal stripping to ensure bone healing.
Surgical Warning: The periosteum must be stripped minimally. Excessive periosteal elevation devascularizes the bone ends, significantly increasing the risk of nonunion, infection, and hardware failure.
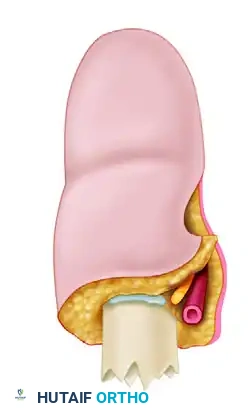
THE BIOMECHANICS AND RATIONALE OF BONE SHORTENING
Bone shortening is a cornerstone principle in replantation surgery. It serves multiple critical functions:
1. Tension-Free Anastomosis: It permits tension-free vascular anastomoses and nerve repairs, which is the single most important factor in preventing microvascular thrombosis.
2. Defect Reduction: Initial bone shortening reduces the size of the soft tissue defect, allowing for primary closure without the immediate need for complex flaps.
3. Maximal Débridement: It allows for aggressive, maximal soft tissue débridement, effectively converting a jagged, contaminated crush injury into a clean, "guillotine-type" injury.
If interpositional vein grafts are utilized, the absolute need for bone shortening is minimized. However, relying on vein grafts introduces the risk of two anastomotic sites per vessel rather than one, inherently decreasing the overall patency rate. Furthermore, harvesting the vein and performing additional anastomoses significantly prolongs ischemia time. Vein grafting is generally reserved for scenarios where amputation has occurred near an undamaged joint, and shortening would destroy the articular surface.
The Thumb Exception: Preserving Length
While shortening is highly beneficial in the fingers, shortening of an amputated thumb must be kept to an absolute minimum. The thumb contributes to approximately 40% to 50% of overall hand function, and its length is critical for effective opposition and pinch kinematics.
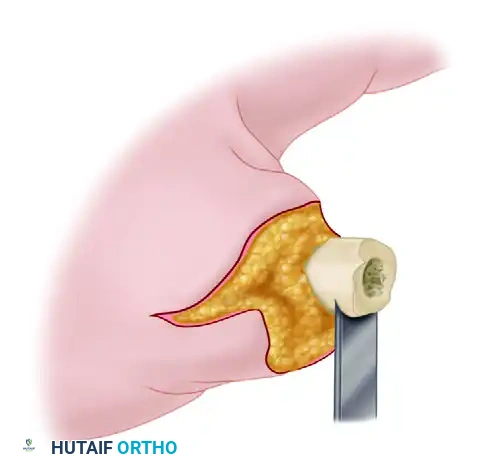
Clinical Pearl: When shortening the thumb proximal phalanx, use an oscillating saw under continuous saline irrigation to remove bone in meticulous 2- to 3-mm increments until satisfactory, tension-free shortening is achieved.
In the lesser digits, shortening of 1 cm usually allows for tension-free vessel anastomosis without excessively impairing hand function. However, shortening a digit much more than 1 to 1.5 cm frequently impairs the biomechanical advantage of the intrinsic muscles and limits the functional arc of motion.
DIGITAL AND METACARPAL FIXATION TECHNIQUES
Bone fixation in digits and metacarpals must balance the need for rigidity with the constraints of time and soft-tissue envelope volume. While plates and screws offer rigid internal fixation, they are often too time-consuming and bulky for distal replantations. Therefore, Kirschner wires (K-wires) and intraosseous wiring remain the workhorses of digital replantation.
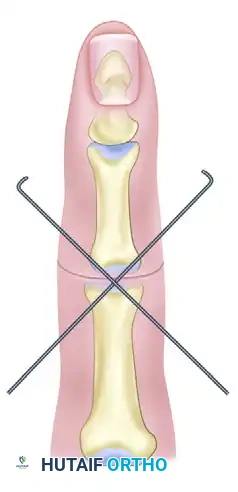
Kirschner Wire Fixation
Fixation is most commonly achieved using either two parallel medullary axial K-wires or a single axial K-wire supplemented by an oblique K-wire. The oblique wire is critical to control rotational forces, which a single axial wire cannot resist.
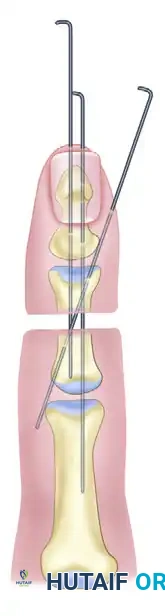
- Parallel K-wires: Provide excellent bending stability but require sufficient bone width.
- Axial + Oblique K-wires: Ideal for narrower phalanges. The oblique wire should cross the fracture site and engage the opposite cortex.
- Joint Preservation: Wires should be placed to allow joint motion whenever possible. Transarticular pinning should be avoided unless necessary for stability in very proximal or highly comminuted fractures.
Care must be taken to maintain precise axial alignment and rotational control, especially when dealing with multiple digital amputations where cascading errors can lead to overlapping digits during flexion.
Intraosseous Wiring Techniques
When the amputation occurs near an undamaged joint, standard longitudinal K-wires may violate the articular surface. In these instances, wire loops passed through transverse drill holes provide excellent compression and stability.
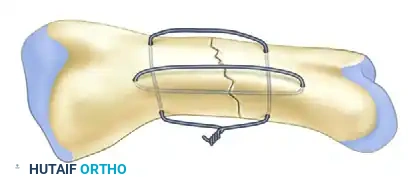
Intraosseous wiring (often performed as a 90-90 wiring technique or a single loop with a stabilizing K-wire) offers a low-profile construct that does not interfere with tendon gliding.
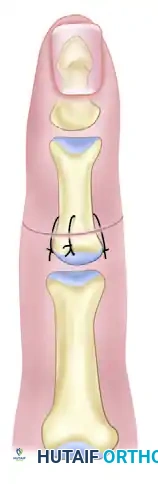
Evidence-Based Practice: Whitney et al. evaluated clinical results comparing single K-wires, crossed K-wires, and intraosseous wires (with and without K-wire support). Although initial results showed similar early angulation deformities across all groups, intraosseous wires were found to have the lowest nonunion and complication rates.
Periosteal repair should be performed whenever feasible. Suturing the periosteum with 4-0 or 5-0 absorbable suture after bone fixation enhances the biological environment for osteogenesis and provides a smooth gliding surface for the extensor mechanism.
MANAGEMENT OF ARTICULAR AMPUTATIONS
Amputations that directly damage the digital joints present a unique reconstructive challenge. The surgeon must decide between primary arthrodesis and joint arthroplasty based on the mechanism of injury, the level of contamination, and the patient's occupational requirements.
Primary Arthrodesis
Amputations involving severe crush or avulsion injuries to the articular surfaces are usually treated by primary arthrodesis. The damaged articular cartilage is resected to healthy, bleeding subchondral bone. Fixation is typically achieved with crossed K-wires or intraosseous wiring.
- Positioning: The distal interphalangeal (DIP) joint is typically fused at 10° to 15° of flexion, the proximal interphalangeal (PIP) joint at 30° to 40° of flexion, and the metacarpophalangeal (MCP) joint at 25° to 35° of flexion.
- Technique: Flat cuts provide maximal contact area, while cup-and-cone reaming allows for fine-tuning of the fusion angle prior to definitive fixation.
Primary Arthroplasty (Silastic Implants)
In highly selected cases, joint motion can be preserved by the primary insertion of a silicone (Silastic) implant.
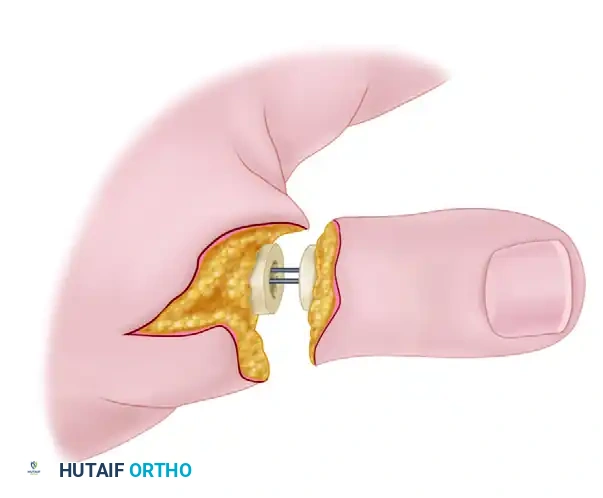
This method is strictly reserved as a primary procedure for amputations that are:
1. Sharp and clean (guillotine-type).
2. Devoid of significant crush or contamination.
3. Occurring in patients whose occupational or functional requirements are best satisfied by having mobile joints (e.g., musicians, typists).
Pitfall: Placing a Silastic implant in a contaminated or severely crushed wound guarantees infection and subsequent implant extrusion. When in doubt, primary arthrodesis or temporary placement of an antibiotic cement spacer is the safer oncologic and functional choice.
MANAGEMENT OF PROXIMAL AMPUTATIONS (CARPUS, FOREARM, AND ARM)
The management of the skeleton in more proximal amputations is highly varied. It requires advanced skill in the handling of medullary fixation devices, bone plates, and screws, as the biomechanical forces in the forearm and arm are exponentially greater than in the digits. Ischemia time becomes a critical limiting factor in major limb replantation, often dictating the choice of fixation.
Carpal Level Amputations
If the amputation level is through the carpus, shortening is easily achieved, and wrist motion can often be partially preserved by the excision of the damaged carpal bones (e.g., proximal row carpectomy). Temporary fixation is achieved with heavy transarticular Steinmann pins to stabilize the radiocarpal or midcarpal joints while the soft tissues heal.
Forearm Amputations
Amputations through the forearm and arm usually require shortening of 2 to 5 cm to allow tension-free vessel anastomoses and nerve repairs.
- Distal Radial Metaphysis: Time constraints frequently dictate modifications to standard internal fixation principles. Distal radial metaphyseal amputations are usually fixed rapidly with crossed Steinmann pins. Plates and screws are used less often due to the time required for application and the bulk of the hardware under a potentially compromised soft-tissue envelope. Intraosseous wiring of the radius has also been used occasionally with success in highly comminuted patterns.
- Diaphyseal Forearm: Amputations more proximally in the forearm are fixed with plates and screws on both bones if ischemia time permits. If time is critical, intramedullary fixation with Rush rods or Steinmann pins in both bones is utilized. Hybrid combinations are also highly effective, such as rigid plate and screw fixation for the radius (to restore the radial bow and pronosupination axis) combined with rapid intramedullary fixation for the ulna.
Elbow and Humerus Amputations
- Olecranon and Elbow: Medullary screws combined with tension-band wire loops are the standard for olecranon amputations. If the elbow joint is severely comminuted, an attempt must be made to salvage sufficient bone stock (even if fused temporarily) to allow for subsequent total elbow arthroplasty once the soft tissue envelope has matured.
- Humerus: Amputations through the humerus are ideally fixed with dynamic compression plates and screws to provide absolute stability. However, complex fracture configurations and strict time considerations regarding muscle ischemia may require the rapid deployment of interfragmentary Steinmann pins or intramedullary rods to establish immediate continuity before proceeding to vascular shunting or repair.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of the skeletal framework in replantation is inextricably linked to the survival of the microvascular repairs.
Immobilization and Splinting
Immediately postoperatively, the limb is placed in a bulky, non-compressive dressing and a custom-molded plaster or fiberglass splint.
* For digital replants, the wrist is typically splinted in slight extension, MCP joints in 70° to 90° of flexion, and IP joints in full extension (intrinsic-plus position) to prevent collateral ligament contracture, unless this places undue tension on the repairs.
* The limb is elevated continuously to promote venous drainage and minimize edema, which can cause compartment syndrome and secondary venous congestion.
Monitoring and Mobilization
- Bone Healing: Radiographic evaluation is performed at 2 weeks, 6 weeks, and 12 weeks. K-wires are typically removed between 4 to 6 weeks in the clinic once clinical and radiographic signs of early union are present.
- Rehabilitation: Early protected mobilization is initiated as soon as the skeletal fixation and tendon repairs allow, often within the first 3 to 5 days using dynamic splinting protocols (e.g., Kleinert or modified Duran protocols). The presence of rigid internal fixation (such as intraosseous wiring) allows for more confident early mobilization compared to single K-wire constructs.
By adhering to these rigorous, evidence-based principles of bone and joint management, the orthopedic surgeon provides the essential mechanical foundation required for the survival and ultimate functional success of the replanted extremity.
You Might Also Like
