Introduction to Lateral Retinacular Release
Lateral retinacular release is a well-established orthopedic procedure aimed at decompressing the patellofemoral joint and correcting abnormal lateral patellar tracking. Historically utilized as a standalone treatment for recurrent patellar instability, contemporary evidence-based practice has refined its indications. Today, it is primarily indicated for Lateral Patellar Compression Syndrome (LPCS)—characterized by chronic lateral tilt, tight lateral retinacular structures, and anterior knee pain without frank dislocation—or as an adjunctive procedure during medial patellofemoral ligament (MPFL) reconstruction or tibial tubercle osteotomies.
The primary objective of the procedure is the restoration of the proper dynamics of the extensor mechanism. By systematically dividing the superficial oblique and deep transverse layers of the lateral retinaculum, the surgeon eliminates pathological lateral tethering, allowing the patella to centralize within the trochlear groove during knee flexion.
💡 Clinical Pearl: Patient Selection
A lateral retinacular release should never be performed as an isolated procedure for hypermobile patellar instability in the absence of a tight lateral retinaculum. Inappropriate application in patients with baseline ligamentous laxity or medial retinacular deficiency predictably leads to iatrogenic medial patellar subluxation.
Biomechanics and Pathoanatomy
Understanding the complex interplay of static and dynamic stabilizers of the patellofemoral joint is paramount. The patella acts as a fulcrum, increasing the mechanical advantage of the quadriceps muscle group.
Normal tracking relies on:
* Static Stabilizers: The geometry of the trochlear groove, the MPFL (providing 50-60% of restraint to lateral displacement at 0-20 degrees of flexion), and the lateral retinaculum.
* Dynamic Stabilizers: The balanced vector forces of the vastus medialis obliquus (VMO) and the vastus lateralis.
In patients with LPCS, adaptive shortening of the lateral retinaculum (specifically the epicondylopatellar and patellotibial bands) creates a persistent lateral tilt. This abnormal tilt increases contact pressures on the lateral patellar facet, leading to progressive chondromalacia and anterior knee pain.
Diagnostic Arthroscopy and Dynamic Assessment
Before committing to a lateral retinacular release, a complete and systematic arthroscopic examination of the knee must be performed to rule out other pathological entities and dynamically assess patellar tracking.
Portal Placement and Initial Viewing
View the patellofemoral joint using a standard 30-degree viewing arthroscope. The arthroscope can be introduced through either the inferior (anterolateral/anteromedial) or superior portals; both provide adequate visualization, though superior portals offer a superior vantage point for dynamic tracking.
- With the arthroscope in the standard anterolateral portal, advance it into the patellofemoral joint.
- Rotate the lens upward and downward alternately to comprehensively view the articular surfaces of the patella and the trochlear groove of the distal femur.
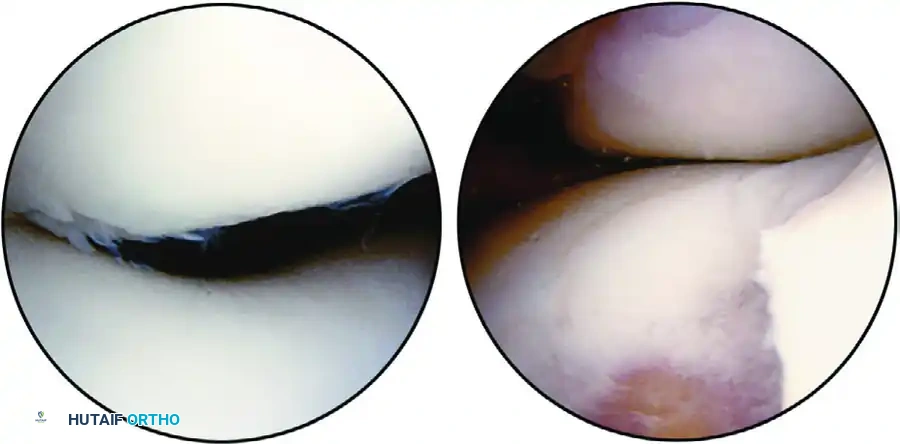
FIGURE 51-49 Patellofemoral articulation view from anterolateral portal. A, Lateral tracking of patella is evident as is grade II chondromalacia of lateral facet. B, Grade IV chondromalacia of trochlea with bare bone exposed. SEE TECHNIQUE 51-24.
Dynamic Tracking Assessment
Manually manipulate the patella with the thumb and index finger to ensure complete viewing of the entire articular surface. The tracking of the patella and the dynamics of the patellofemoral joint are optimally viewed from a superior portal.
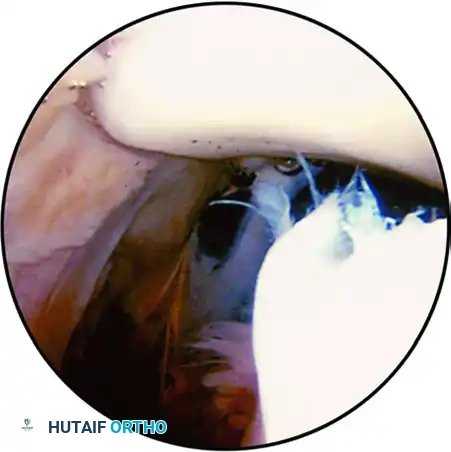
FIGURE 51-50 Patellofemoral joint view from superolateral portal; lateral subluxation of patella is evident. SEE TECHNIQUE 51-24.
⚠️ Surgical Warning: Interpreting Patellar Tracking
The patella naturally rides laterally with the knee in full extension. Observation of the patella in this extended position does not confirm that it is pathologically subluxable or riding laterally.
To accurately assess tracking:
* Slowly move the knee from full extension into 30 to 40 degrees of flexion.
* As the knee flexes, the patella should enter the trochlear groove and become congruous and centered.
* Pathological Finding: Persistent lateral tilt or overhang of the lateral facet over the edge of the lateral femoral condyle at 30 to 40 degrees of flexion strongly suggests a lateral tracking phenomenon requiring release.
Management of Chondromalacia
Note the various degrees of chondromalacia on the patellar and trochlear articular surfaces and record them accurately.

FIGURE 51-51 Grade III chondromalacia of patella involving central ridge and lateral facet. SEE TECHNIQUE 51-24.
If severe chondromalacic changes are present, trim and shave the articular surface where appropriate. However, extensive shaving of chondromalacic areas on the patellar or trochlear surface generally yields only short-term symptomatic relief.
* Chondroplasty Principle: Shaving should be kept to an absolute minimum, emphasizing the removal of only degenerative, fibrillated material that may cause mechanical catching.
Surgical Technique: Arthroscopic Lateral Retinacular Release
Once the diagnostic arthroscopy and necessary chondroplasty are complete, remove the arthroscopic instruments from the joint and evacuate the irrigating fluids to prepare for the release.
Step 1: Anatomic Landmark Identification
Attempt to palpate the inferior edge of the vastus lateralis tendon. Mark this junction at its insertion into the superior pole of the patella using an 18-gauge spinal needle.
* Note: If the tendinous edge cannot be definitively palpated due to patient habitus or swelling, simply insert the needle at the superolateral corner of the patella to serve as the proximal boundary of the release.
Step 2: Portal Re-establishment and Instrument Insertion
- Insert the arthroscope through the superolateral or the anteromedial portal to maintain a clear view of the lateral retinaculum.
- Initially, insert the electrocautery device (standard monopolar or modern radiofrequency ablation wand) into the anterolateral portal.
Step 3: Executing the Release
Under direct arthroscopic guidance, systematically divide the synovium and lateral retinaculum.
1. Begin at the superolateral corner of the patella (marked by the spinal needle).
2. Carry the release distally to the inferior extent of the lateral border of the patellar tendon.
3. Occasionally, the electrocautery instrument must be repositioned into a superomedial or superolateral portal to successfully complete the most inferior portion of the release.
4. The release can be extended proximally along the lateral border of the vastus lateralis tendon to ensure complete decompression.
🔪 Surgical Pitfall: The Superolateral Geniculate Artery
The superolateral geniculate artery traverses the lateral retinaculum near the superior pole of the patella. Meticulous hemostasis using electrocautery is mandatory when dividing this area to prevent massive postoperative hemarthrosis.
Surgical Technique: Percutaneous Method
If a percutaneous method is chosen over an entirely arthroscopic electrocautery release, the joint can be redistended with fluid or left deflated based on surgeon preference.
Step 1: Incision and Undermining
Make a 1-cm incision at the lateral border of the patella (alternatively, the standard anterolateral portal can be utilized). Using a hemostat or dissecting scissors, undermine the skin and subcutaneous tissue to separate it from the underlying retinaculum.
* Undermine along the entire lateral border of the patella.
* Extend distally along the lateral border of the patellar tendon.
* Extend proximally to the insertion of the vastus lateralis muscle into the superolateral pole of the patella.
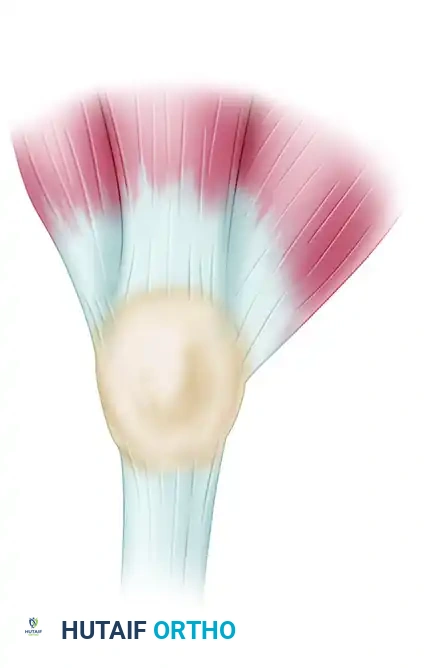
FIGURE 51-52 Line of deep incision for lateral patellar release of right knee. SEE TECHNIQUE 51-24.
Step 2: Scissor Release
- Place one tine of a curved Mayo scissors into the retinacular and capsular defect created by the portal/incision.
- Push the scissors superiorly along the lateral edge of the patella up to the vastus lateralis. At this point, turn the scissors slightly to follow the lateral border of the vastus lateralis for a short distance, cutting the retinacular fibers.
- Repeat this maneuver distally, advancing the scissors along the lateral border of the patella and the patellar tendon down to the level of the lateral tibial plateau.
Intraoperative Verification of Release
Regardless of whether the arthroscopic or percutaneous technique is utilized, the adequacy of the release must be physically verified.
- Remove all instruments (and scissors) from the knee.
- Place the knee in full extension.
- Grasp the patella firmly between the thumb and index finger.
- Attempt to tilt the patella 90 degrees to the plane of the trochlear surface (the "patellar tilt test").
If the patella cannot be easily tilted to 90 degrees, carefully inspect the release arthroscopically. Identify any remaining tethering bands (often the deep transverse retinacular fibers) and carry the release further if necessary. If the lateral release is complete but instability or maltracking persists, consider the necessity of a medial plication.
Adjunctive Procedures
Arthroscopic Medial Parapatellar Plication
Arthroscopic plication of the medial retinaculum is occasionally described for patellar instability to balance the extensor mechanism after a lateral release.
The Halbrecht Technique:
* Uses a 17-gauge Tuohy epidural needle to pass a No. 1 polydioxanone (PDS) suture near the medial edge of the patella.
* The edge of the suture is retrieved out of a superolateral portal.
* The needle is backed up slightly to remain under the subcutaneous tissue and advanced posteriorly about 2 cm.
* The needle is passed back through the retinaculum, and the resulting loop of the suture is pulled out superiorly, taking both tails out superiorly.
* After the passage of four to five sutures, they are tied arthroscopically through the anteromedial portal.
Author's Perspective: While arthroscopic plication is feasible, we generally do not perform this specific percutaneous procedure. We believe that the same technique can be performed more adequately, with superior imbrication and the use of robust nonabsorbable sutures, through a small, direct medial parapatellar incision.
Management of Localized Nodular Synovitis
During the systematic diagnostic arthroscopy preceding the lateral release, surgeons may encounter incidental pathology, such as localized nodular synovitis.
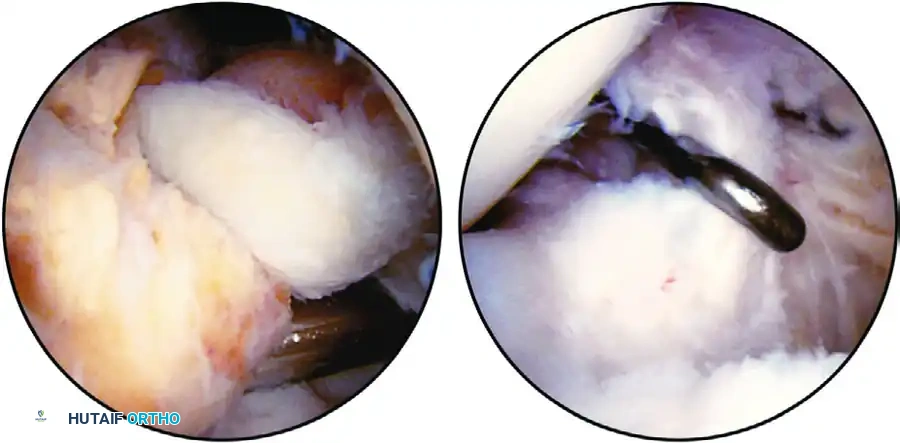
FIGURE 51-53 A, Localized nodular synovitis of posteromedial compartment of knee. B, Arthroscopic excision of localized nodular synovitis with arthroscope in posteromedial portal and probe through intercondylar notch to palpate posterior cruciate ligament. Synovial attachment of nodular synovitis is just superior and posterior to probe. SEE TECHNIQUE 51-25.
If identified, these lesions should be excised arthroscopically using a motorized shaver or radiofrequency wand to prevent mechanical symptoms or recurrent effusions.
Hemostasis and Closure
Postoperative hemarthrosis is the most common complication following a lateral retinacular release. Meticulous preventative measures are required.
- Pressure Pad Application: Place a thick sponge pad over the superolateral aspect of the distal thigh, just proximal to the patellar tendon. This serves as a localized pressure pad over the cut superolateral geniculate vessels. This simple maneuver has drastically reduced the incidence of troublesome postoperative hemarthrosis.
- Drainage: A closed-suction drain can be placed intraarticularly. If utilized, it is typically removed after several hours or on postoperative day one, depending on the volume of output.
- Close the portals using standard non-absorbable sutures or surgical strips.
Postoperative Care and Rehabilitation Protocol
The rehabilitation protocol following a lateral retinacular release must balance the need for hemostasis with the prevention of retinacular readherence.
- Initial Immobilization (0-48 Hours): The knee is maintained in an immobile, fully extended position for the first 48 hours. A bulky compressive dressing and a knee immobilizer or hinged brace locked in extension are utilized.
- Early Range of Motion (Post-Op Day 2+): Gentle range-of-motion (ROM) exercises are initiated after 48 hours.
- Critical Rule: Immobilization of the knee in extension for longer than 72 hours is strictly contraindicated. Prolonged immobilization allows the raw edges of the lateral retinacular release to adhere via scar tissue, rendering the surgical release completely ineffective. Early ROM mechanically spreads the release, ensuring the gap heals with lengthened, compliant tissue.
- Strengthening: Quadriceps isometric exercises and stiff-leg raises are encouraged immediately to prevent vastus medialis atrophy.
- Weight Bearing: Weight bearing is allowed as tolerated (WBAT) with crutches, weaning off assistive devices as quadriceps control returns and the effusion subsides.
By adhering strictly to these surgical principles, precise anatomical landmarks, and rigorous postoperative protocols, the orthopedic surgeon can effectively utilize the lateral retinacular release to restore patellofemoral kinematics and alleviate chronic lateral compartment compression.
📚 Medical References
- lateral retinacular release in mechanical patellofemoral disorders, Knee Surg Sports Traumatol Arthrosc 10:177, 2002.
- Christoforakis JJ, Sanchez-Ballester J, Hant N, et al: Synovial shelves of the knee: association with chondral lesions, Knee Surg Sports Traumatol Arthros 14:1292, 2006.
- Demirag B, Ozturk C, Karakayali M: Symptomatic infrapatellar plica, Knee Surg Sports Traumatol Arthrosc 14:156, 2006.
- Dorchak JD, Barrack RL, Kneisl JS, et al: Arthroscopic treatment of symptomatic synovial plica of the knee: long-term followup, Am J Sports Med 19:503, 1991.
- Dupont JY: Synovial plicae of the knee. Controversies and review, Clin Sports Med 16:87, 1997.
- Ewing JW: Plica: pathologic or not? J Am Acad Orthop Surg 1:117, 1993.
- Flanagan JP, Trakru S, Meyer M, et al: Arthroscopic excision of symptomatic medial plica. A study of 118 knees with 1-4 year follow-up, Acta Orthop Scand 65:408, 1994.
- Garcia-Valtuille R, Abascal F, Cerezal L, et al: Anatomy and MR imaging appearances of synovial plicae of the knee, Radiographics 22:775, 2002.
- Irha E, Vrdoljak J: Medial synovial plica syndrome of the knee: a diagnostic pitfall in adolescent athletes, J Pediatr Orthop B 12:44, 2003.
- Johnson DP, Eastwood DM, Witherow PJ: Symptomatic synovial plicae of the knee, J Bone Joint Surg 75A:1485, 1993.
- Kim SJ, Choe WS: Arthroscopic fi ndings of the synovial plicae of the knee, Arthroscopy 13:33, 1997.
- O’Dwyer KJ, Peace PK: The plica syndrome, Injury 19:350, 1988.
- Ogata S, Uhthoff HK: The development of synovial plicae in human knee joints: an embryologic study, Arthroscopy 6:315, 1990.
- Patel D: Plica as a cause of anterior knee pain, Orthop Clin North Am 17:273, 1986.
- Tindel NL, Nisonson B: The plica syndrome, Orthop Clin North Am 23:613, 1992.
- White SH: Bucket handle tear of medial plica, Knee 9:253, 2002.
- Yilmaz C, Golpinar A, Vurucu A, et al: Retinacular band excision improves outcome in treatment of plica syndrome, Int Orthop 29:291, 2005.
- Articular Cartilage Injuries,
