INTRODUCTION TO MYELOMENINGOCELE SPINAL DEFORMITIES
The treatment of patients with myelomeningocele-associated spinal deformities, particularly kyphoscoliosis, represents one of the most formidable and technically demanding challenges in the realm of operative orthopaedics and spine surgery. Successful management requires a highly coordinated, multidisciplinary team effort, necessitating the seamless cooperation of consultants across several subspecialties, including pediatric orthopaedics, neurosurgery, urology, and plastic surgery.
These children invariably present with multiple, complex systemic dysfunctions that directly influence the natural history, preoperative optimization, and ultimate surgical treatment of their spinal deformity. The absence of posterior neural elements, combined with profound neuromuscular imbalance, creates a biomechanical environment highly conducive to rapid curve progression and hardware failure.

INCIDENCE, NATURAL HISTORY, AND PATHOMECHANICS
Scoliosis in children with myelomeningocele is rarely an isolated coronal plane deformity; it is frequently associated with severe lordotic or kyphotic deviations. These deformities are relentlessly progressive and, if left untreated, lead to significant functional disabilities, loss of sitting balance, cardiopulmonary compromise, and recurrent pressure ulcerations.
Epidemiological studies, notably by Banta et al., have demonstrated that the incidence of scoliosis increases proportionally with both advancing age and the cephalad level of the neurological deficit. Virtually all patients with a thoracolumbar-level spina bifida will develop a clinically significant spinal deformity by the age of 14 years.
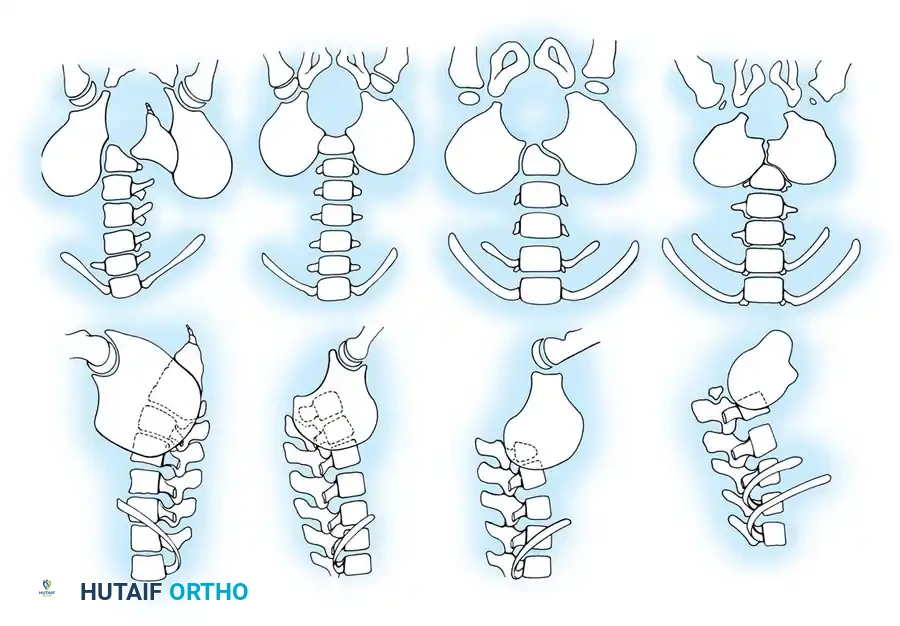
Raycroft and Curtis classically differentiated these deformities into two distinct etiologic categories: Congenital and Paralytic.
Congenital Scoliosis
Congenital scoliosis in the setting of myelomeningocele is driven by the structural disorganization of the developing vertebrae, leading to asymmetrical growth. This includes the classic spectrum of congenital anomalies:
* Hemivertebrae (fully segmented, semi-segmented, or incarcerated)
* Unilateral unsegmented bars
* Complex combinations of bars and hemivertebrae
Congenital curves account for approximately 15% to 20% of myelomeningocele patients presenting with scoliosis. Because the deformity is structural and osseous in origin, it is highly rigid and entirely refractory to orthotic management.
Paralytic (Developmental) Scoliosis
The vast majority of scoliotic curves in this population are paralytic. In these patients, the spine is structurally normal and straight at birth but gradually develops a progressive curvature secondary to profound neuromuscular imbalance, absent intrinsic spinal musculature, and gravity.
These are typically long, sweeping, C-shaped curves with the apex located in the thoracolumbar or lumbar spine.

Paralytic curves frequently extend distally into the lumbosacral junction, driving severe pelvic obliquity. Unlike idiopathic scoliosis, these curvatures initiate at a much younger age—often beginning between 3 to 4 years of age—and can reach severe, surgical magnitudes before the child's tenth birthday.
CLINICAL PEARL: When considering the timing of surgical intervention, the surgeon must account for future trunk growth and final trunk height. However, as Lindseth noted, children with myelomeningocele often exhibit stunted growth due to growth hormone deficiencies and tend to reach skeletal maturity earlier than their peers (often by 9 to 10 years in girls and 11 to 12 years in boys). This altered growth velocity must be factored into the decision to fuse.
COMPREHENSIVE CLINICAL EVALUATION
A meticulous, systems-based evaluation is the cornerstone of preoperative planning. The surgeon must investigate the following critical domains:
- Neurosurgical Status: Presence of hydrocephalus, patency of ventriculoperitoneal (VP) shunts, and signs of Arnold-Chiari malformation.
- Urological Function: Bowel and bladder continence, frequency of urinary tract infections, and reliance on indwelling catheters or clean intermittent catheterization (CIC).
- Allergy Profile: Strict assessment for latex allergies.
- Functional Status: Method of ambulation (community ambulator vs. household ambulator vs. non-ambulatory), sitting balance, and mental status.
- Integumentary System: Presence of decubitus ulcers, particularly over the ischial tuberosities or the gibbus deformity.
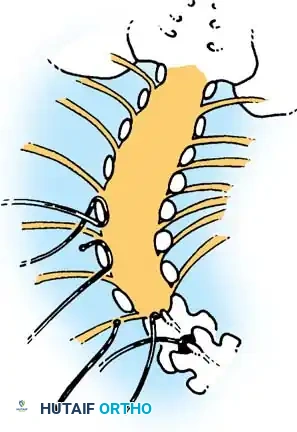
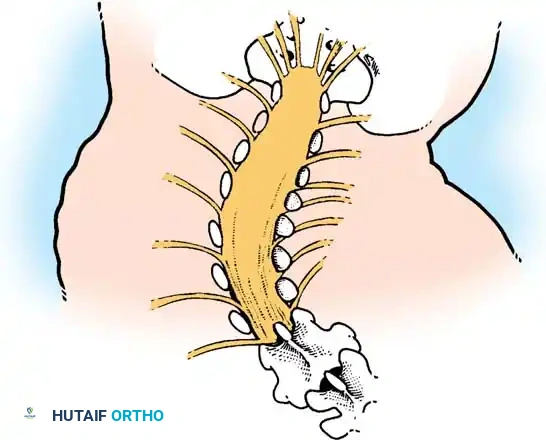
The Tethered Cord Paradigm
In patients with progressive paralytic scoliosis, the surgeon must maintain a high index of suspicion for intraspinal anomalies. Hydromyelia, a malfunctioning ventricular shunt, syringomyelia, or compression from an Arnold-Chiari syndrome can rapidly accelerate curve progression.
Lubicky astutely noted that almost all patients with myelomeningocele exhibit radiographic evidence of spinal cord tethering at the site of the primary sac closure.
SURGICAL WARNING: The mere presence of radiographic tethering on MRI does not automatically imply pathological traction on the cord. The surgeon must look for corroborating clinical signs of tethering, which include: new-onset back pain, increased lower extremity spasticity, rapid changes in muscle strength, deteriorating gait, acute changes in bowel/bladder function, or the sudden appearance of foot deformities (e.g., cavovarus).

Evaluating Pelvic Obliquity and Hip Contractures
Careful evaluation of pelvic obliquity is mandatory. Winter and Pinto emphasized the necessity of differentiating between spinal-driven pelvic obliquity and hip-driven pelvic obliquity. Because these patients are highly prone to developing severe contractures around the hips, a rigorous physical examination of the hip adductors, extensors, and flexors is required.
Lubicky highlighted a particularly treacherous clinical scenario: patients with myelomeningocele who present with severe extension contractures of the hips. In these individuals, the only way they can achieve an upright sitting posture is by hyper-flexing through their thoracolumbar spine.
If a surgeon were to perform a rigid spinal fusion on such a patient without first addressing the hips, sitting would become biomechanically impossible. The patient would be forced into a recumbent position, and massive mechanical stress would be transferred to the spinal instrumentation, inevitably leading to catastrophic hardware failure.
CLINICAL PEARL: Physiological hip flexion must be surgically restored (via soft tissue releases or proximal femoral osteotomies) before or concurrently with spinal instrumentation and fusion to ensure the patient can sit postoperatively.
The Latex Allergy Imperative
Emans et al. brought critical attention to the high prevalence of latex allergy in the myelomeningocele population. Due to repeated mucosal exposure to latex during daily intermittent catheterizations and multiple early childhood surgeries, these patients become highly sensitized to natural latex plant proteins.
This is an IgE-mediated, Type I immediate hypersensitivity reaction. Intraoperative anaphylaxis can occur rapidly and may be easily misdiagnosed as hypovolemic shock or an anesthetic complication.
SURGICAL WARNING: We strongly advocate treating all patients with myelomeningocele as if they have a documented latex allergy. A strict latex-free environment must be maintained from the preoperative holding area through the operating theater and into the recovery unit.

RADIOGRAPHIC EVALUATION
A comprehensive radiographic series is essential for three-dimensional deformity analysis.
* Standard Views: Upright (standing or sitting) and supine anteroposterior (AP) and lateral radiographs. Upright films reveal the true functional magnitude of the deformity under gravity, while supine films provide better bony detail of congenital anomalies.
* Flexibility Films: Supine right and left maximum side-bending films, or traction films, are utilized to assess curve rigidity and plan the levels of structural release.
* Pelvic Obliquity Assessment: Supine AP pelvis views obtained with the hips in a "relaxed" position (flexed and abducted/adducted to accommodate contractures). Alternatively, prone films with the legs hanging off the table can unmask true pelvic obliquity.
* Advanced Imaging: MRI is mandatory to evaluate for hydromyelia, tethered cord, diastematomyelia, and Arnold-Chiari malformations. Intravenous pyelography or renal ultrasound should be updated per urological recommendations to map ureteral anatomy prior to anterior spinal approaches.
NON-OPERATIVE MANAGEMENT: ORTHOTIC TREATMENT
While the natural history of paralytic curves in myelomeningocele is ultimately not altered by orthotic management, bracing serves a vital temporizing role. The primary goal of bracing is to delay surgical fusion until adequate spinal growth and thoracic volume have been achieved, thereby preventing early-onset scoliosis (EOS) complications such as thoracic insufficiency syndrome.
Bracing is exclusively indicated for flexible paralytic curves; it is entirely ineffective for rigid congenital deformities. A custom-molded, bivalved Thoracolumbosacral Orthosis (TLSO) is typically employed. It improves sitting balance and frees the patient's upper extremities for activities of daily living.
However, orthotic management in the insensate patient is fraught with peril. The skin must be inspected meticulously by caregivers multiple times a day. The slightest erythema or sign of pressure necrosis demands immediate cessation of brace wear and orthotic modification. If the curve progresses despite bracing, or if recurrent pressure sores make brace wear impossible, surgical intervention becomes mandatory.
OPERATIVE TREATMENT: STRATEGIES AND TECHNIQUES
Surgery on the myelomeningocele spine is a massive undertaking associated with a high complication profile. Hull, Mackel, Lindseth, and Sriram have all documented the unique surgical hurdles in this population:
1. Hostile Soft Tissue Envelope: The posterior approach is complicated by densely scarred, adherent soft tissues from prior neural tube closures, leading to lengthy and hemorrhagic exposures.
2. Rigid Deformities: The curves are often stiff, making coronal and sagittal correction difficult without aggressive osteotomies.
3. Osteopenic Bone: Poor bone mineral density provides suboptimal purchase for pedicle screws and hooks.
4. Absent Posterior Elements: The spina bifida defect means there is a lack of lamina and spinous processes, eliminating traditional posterior fusion beds and hook anchor points.
5. Poor Soft Tissue Coverage: The lateral displacement of the paraspinal musculature leaves prominent hardware vulnerable to skin breakdown.
The Gold Standard: Combined Anterior and Posterior Arthrodesis
Because posterior fusion alone is associated with an unacceptably high rate of pseudarthrosis and hardware failure (due to the absent posterior elements and poor bone stock), the modern standard of care for severe paralytic curves is a combined anterior and posterior spinal fusion.
Osebold et al. demonstrated that combining an anterior release and interbody fusion with a posterior instrumented arthrodesis reduced the pseudarthrosis rate from 45% (posterior alone) to 23%. Contemporary techniques utilizing rigid pedicle screw constructs and structural interbody cages have lowered this rate even further.
The Anterior Approach
The anterior approach allows for aggressive release of the contracted anterior longitudinal ligament and annulus fibrosus, maximizing curve flexibility. It also provides a massive, vascularized surface area for interbody arthrodesis.
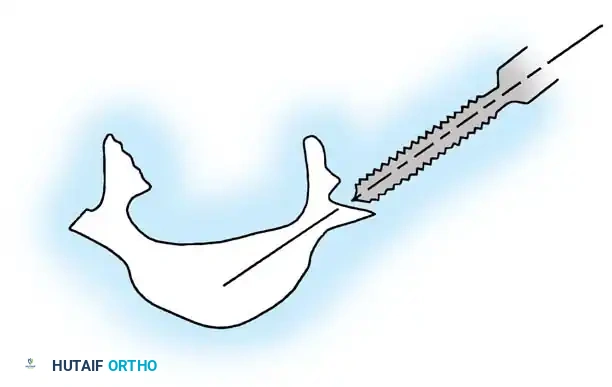
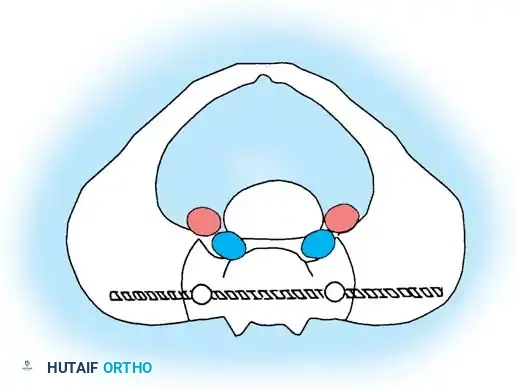
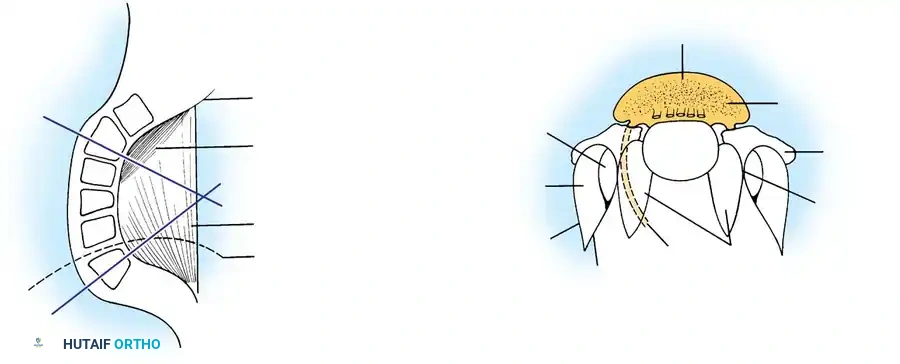
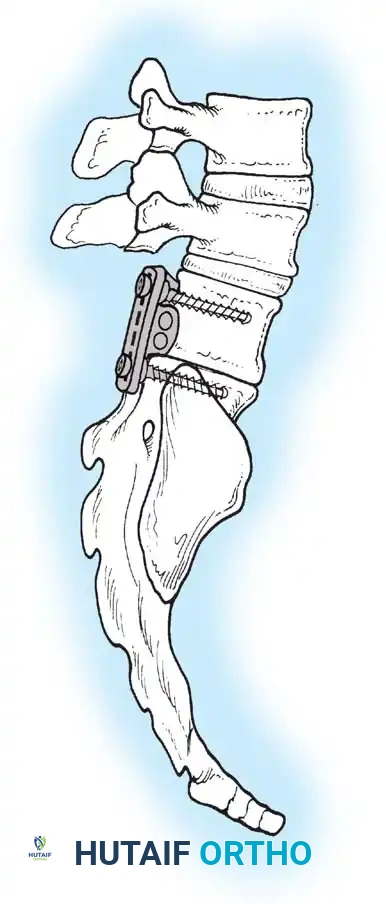
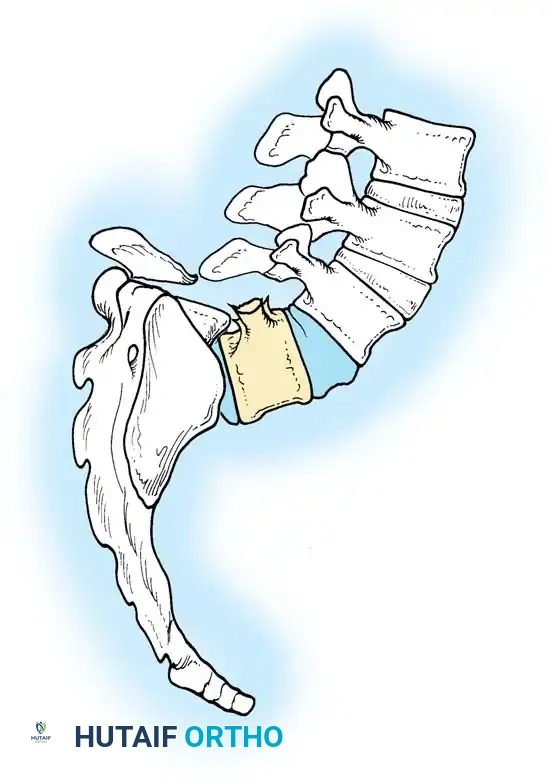
For lower lumbar and lumbosacral curves, an anterior transperitoneal or retroperitoneal approach is utilized.
As illustrated above, an anterior approach for the resection of the L4-L5 disc, the L5 vertebral body, and the L5-S1 disc can be achieved through a transverse incision across the rectus abdominis. The great vessels (aorta, inferior vena cava, and the iliac bifurcations) must be meticulously identified and mobilized laterally. The structural resection is performed directly between the bifurcation of the great vessels.

Following the anterior release and interbody grafting (often utilizing structural allograft or titanium cages packed with autograft/allograft), the patient is staged for the posterior procedure.

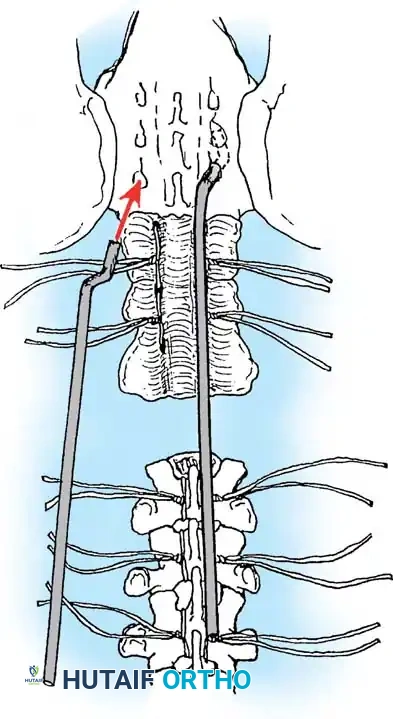
Posterior Instrumentation Techniques
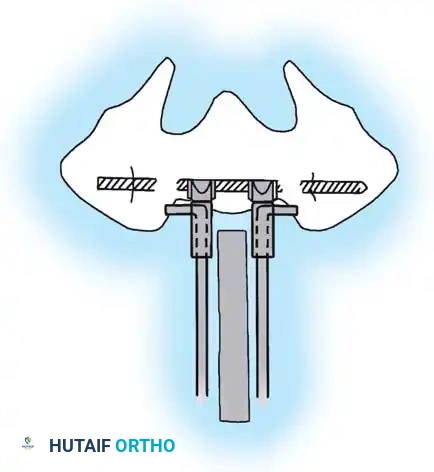
The posterior approach requires meticulous subperiosteal dissection. The surgeon must navigate the transition zone between the normal cephalad lamina and the dysplastic, bifid elements caudally. The dural sac is often exposed and highly vulnerable just deep to the scarred fascia.
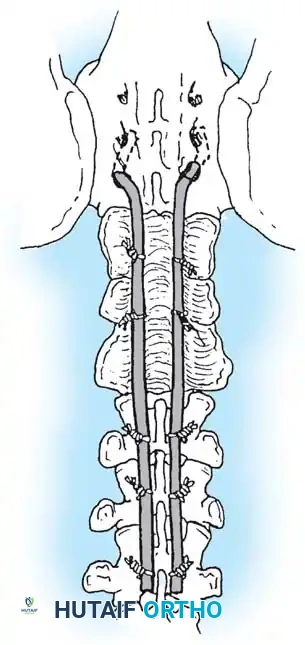
Pedicle screw fixation is the anchor of choice, providing three-column control even in the absence of posterior elements. Free-hand techniques are often supplemented with intraoperative fluoroscopy or robotic navigation due to the highly dysmorphic pedicle anatomy.
Copious amounts of bone graft (autograft from the iliac crest, combined with allograft and osteoinductive biologics) are laid into the lateral gutters and over the decorticated transverse processes to ensure a robust fusion mass.
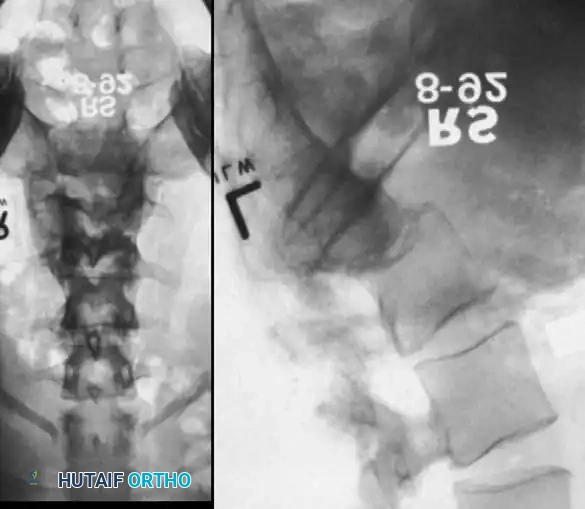
Severe Lumbosacral Deformity: The L5 Vertebrectomy
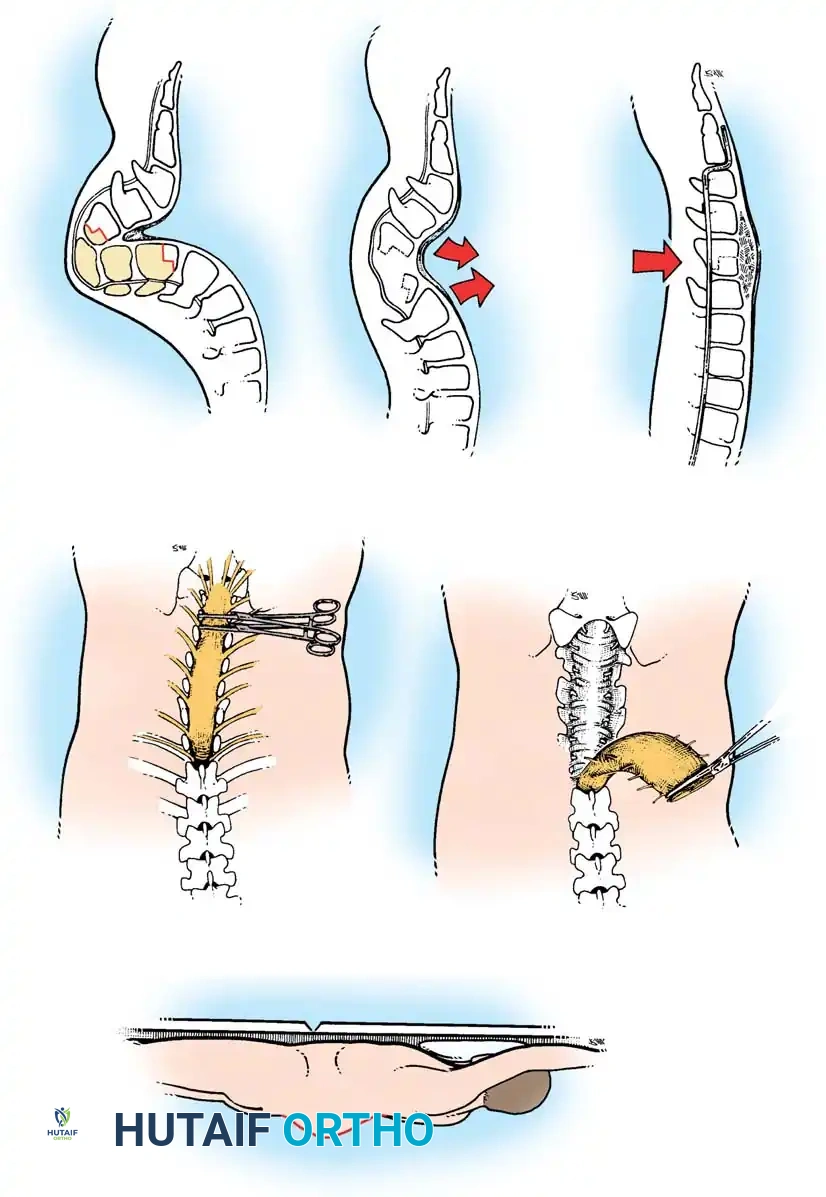
In cases of extreme lumbosacral kyphosis or spondyloptosis associated with myelomeningocele, a standard fusion is insufficient to restore sagittal balance. Gaines described a powerful two-stage L5 vertebrectomy technique to address this.
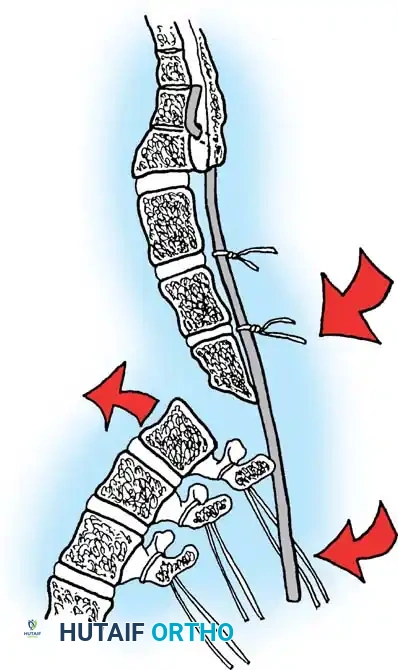
Stage 1 (Anterior): The L5 vertebral body and adjacent discs are completely excised via an anterior approach, decompressing the anterior neural elements and mobilizing the spine.
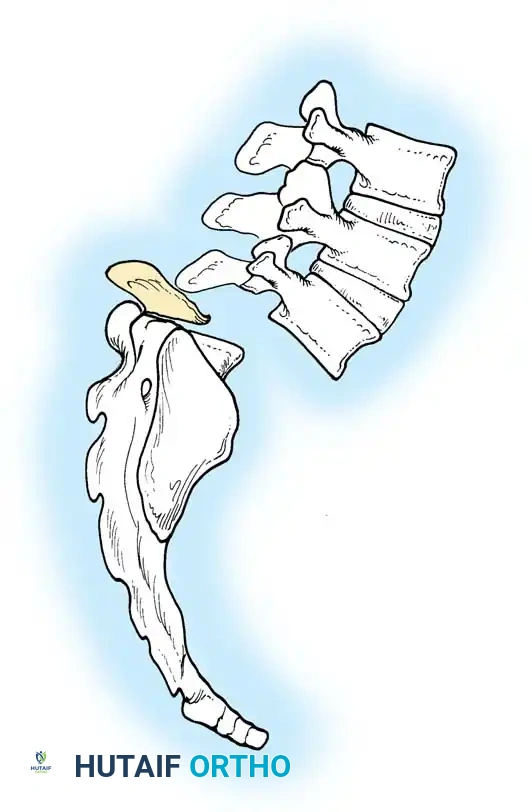
Stage 2 (Posterior): The patient is flipped prone. The L4 vertebra is then reduced directly onto the sacrum (S1), effectively shortening the spine, correcting the kyphosis, and allowing for rigid posterior pedicle screw fixation from the lumbar spine to the pelvis.
SELECTION OF FUSION LEVELS
Determining the proximal and distal extent of the fusion is a critical biomechanical decision. The general rule is to fuse from "neutral vertebra to neutral vertebra," ensuring the end vertebrae of the scoliotic curve are centered within the stable zone of Harrington.
A common pitfall in paralytic curves is fusing too short, particularly at the proximal end, which inevitably leads to adjacent segment failure and "adding-on" of the deformity. When in doubt, a longer fusion construct is biomechanically safer.

Distal Fixation: To the Pelvis or Not?
Historically, all paralytic curves in myelomeningocele were fused down to the pelvis because the deficient posterior lumbar elements made isolated lumbar fixation impossible. However, modern pedicle screw biomechanics have nuanced this approach.
- Ambulatory Patients: Mazur and Müller demonstrated that fusing the spine to the pelvis in community ambulators severely restricts their pelvic rotation, thereby diminishing or entirely eliminating their ability to walk. Therefore, in ambulatory patients, the fusion should be stopped short of the pelvis (e.g., at L5) if a stable, balanced construct can be achieved. This preserves lumbosacral motion, allowing the patient to compensate for mild hip flexion contractures.
- Non-Ambulatory Patients: In wheelchair-bound patients, the rules change. Unless the lumbar curve can be rigidly corrected to less than 20 degrees and the pelvic obliquity to less than 15 degrees, the scoliosis will continue to progress if the lumbosacral junction is left unfused. Therefore, rigid pelvic fixation (utilizing iliac screws or S2-alar-iliac [S2AI] screws) is mandatory to level the pelvis and ensure a stable sitting foundation.

Attention to sagittal contour is paramount. Even in a non-ambulatory patient, the maintenance of physiological lumbar lordosis is critical to position the head over the pelvis and prevent forward collapse.

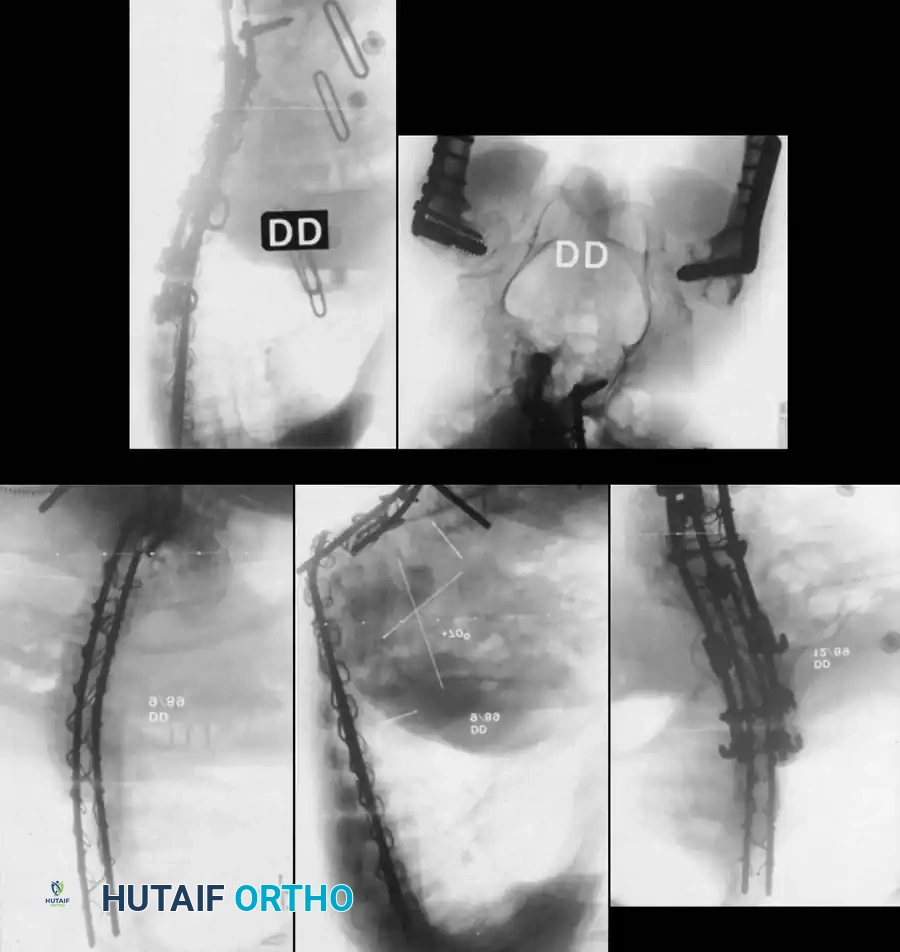
POSTOPERATIVE PROTO
Associated Surgical & Radiographic Imaging