Introduction and Epidemiology
Femorotibial knee dislocation represents a catastrophic, limb-threatening orthopaedic emergency characterized by profound disruption of the osseous and soft-tissue stabilizers of the knee. By definition, a true knee dislocation involves the gross displacement of the tibia relative to the femur, necessitating the rupture of at least three of the four major ligamentous structures. Despite its severity, traumatic knee dislocation is considered an uncommon injury, historically representing less than 0.2% of all orthopaedic injuries. However, the true incidence is widely acknowledged to be underreported. Between 20% and 50% of knee dislocations spontaneously reduce prior to clinical presentation, leaving the unwary clinician with a seemingly aligned limb that harbors devastating internal derangement and critical neurovascular vulnerability.
The epidemiology of femorotibial dislocations exhibits a distinct bimodal distribution based on the mechanism of injury. Historically, the vast majority of these injuries were the result of high-energy trauma, such as motor vehicle collisions, motorcycle crashes, or severe industrial accidents. In these scenarios, the dislocation is frequently accompanied by polytrauma, open fractures, and significant soft tissue degloving. Conversely, there is a rapidly growing incidence of low-energy knee dislocations. These occur in athletic settings—such as football, rugby, or skiing—and increasingly among the morbidly obese population. In obese patients, ultra-low velocity trauma, such as a simple mechanical fall from a standing height, can generate massive rotational and translational forces sufficient to completely dislocate the femorotibial articulation.
Mechanism of Injury and Classification
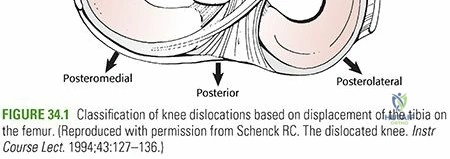
The mechanism of injury directly dictates the direction of the dislocation and the resulting pattern of ligamentous and neurovascular damage. The Kennedy classification categorizes knee dislocations based on the direction of tibial displacement relative to the femur:
* Anterior Dislocation: The most common pattern, typically resulting from forced hyperextension. This often occurs when a deceleration force is applied to the anterior tibia while the foot is planted. It produces maximal tension on the posterior elements, frequently resulting in intimal tearing of the popliteal artery.
* Posterior Dislocation: Classically associated with a "dashboard injury" during a motor vehicle collision, where an axial load is applied to the anterior tibia of a flexed knee. This mechanism drives the tibia posteriorly, predictably rupturing the posterior cruciate ligament (PCL) and frequently the anterior cruciate ligament (ACL), while putting the popliteal artery at risk for complete transection.
* Medial and Lateral Dislocations: These result from massive varus or valgus forces, respectively. They are highly associated with severe capsular avulsions, collateral ligament ruptures, and a significantly elevated risk of common peroneal nerve palsy, particularly in lateral dislocations.
* Rotational Dislocations: Posterolateral dislocations are notoriously irreducible due to the medial femoral condyle buttonholing through the medial joint capsule.

Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
The knee is a complex ginglymoid (hinge) joint comprising three distinct articulations: the patellofemoral, tibiofemoral, and proximal tibiofibular joints. The osseous geometry of the tibiofemoral joint provides minimal inherent stability. The convex femoral condyles articulate with the relatively flat tibial plateaus, creating a highly incongruent joint surface. Under normal cyclic loading, the knee joint may experience compressive forces up to five times body weight during a standard gait cycle. The normal physiologic range of motion extends from 0 degrees of extension to approximately 140 degrees of flexion, coupled with an obligatory 8 to 12 degrees of internal and external rotation through the flexion-extension arc (the "screw-home" mechanism). Because the bony architecture offers negligible resistance to translation, the dynamic and static stability of the knee is conferred almost entirely by the surrounding soft tissue envelope, including the ligaments, menisci, joint capsule, and musculotendinous units.
Ligamentous Biomechanics
Significant soft tissue disruption is an absolute prerequisite for a femorotibial dislocation. The extent of ligamentous injury correlates directly with the degree of displacement; biomechanical studies demonstrate that macroscopic ligamentous failure occurs when displacement exceeds 10% to 25% of the resting length of the ligament.
In a typical multi-ligament knee injury (MLKI), the central pivot (ACL and PCL) is completely disrupted, accompanied by varying degrees of injury to the peripheral stabilizers (the medial collateral ligament complex and the posterolateral corner). The ACL serves as the primary restraint to anterior tibial translation, while the PCL prevents posterior translation. The medial collateral ligament (MCL) and posteromedial capsule resist valgus stress and external rotation. The posterolateral corner (PLC)—comprising the lateral collateral ligament (LCL), popliteus tendon, and popliteofibular ligament—acts as the primary restraint to varus stress and external tibial rotation.
Neurovascular Proximity and Vulnerability
The most critical anatomical feature in the context of knee dislocation is the precise routing of the popliteal neurovascular bundle. The popliteal artery courses posteriorly through the thigh and enters the popliteal fossa via a rigid fibrous tunnel at the adductor hiatus. It then travels directly posterior to the joint capsule, giving off five geniculate branches that provide collateral circulation. Distal to the joint line, the artery passes deep to the tendinous arch of the soleus muscle, entering another unyielding fibrous canal.
This anatomy creates two firm tethering points—proximally at the adductor hiatus and distally at the soleal arch. During a dislocation, the unyielding nature of these tethers leaves the popliteal vessels highly vulnerable to severe traction, tenting, intimal disruption, or complete transection. The collateral genicular circulation is insufficient to maintain limb viability if the main popliteal trunk is occluded. Furthermore, the common peroneal nerve wraps around the fibular neck, tethering it laterally and making it highly susceptible to stretch injuries, particularly during varus-producing or medial dislocations. Associated fractures of the tibial eminence, tibial tubercle, fibular head or neck, and capsular avulsions (e.g., Segond fractures) are common and must elevate the surgeon's index of suspicion for an underlying MLKI.
Indications and Contraindications
The management of a femorotibial dislocation is divided into acute damage control and delayed definitive reconstruction. Immediate intervention is dictated by the neurovascular status of the limb and the stability of the joint post-reduction.
| Clinical Scenario | Operative Indications | Non Operative Indications |
|---|---|---|
| Vascular Status | Hard signs of ischemia (absent pulses, expanding hematoma, pulsatile bleeding); ABI < 0.9 with positive CTA requiring bypass or repair. | Normal pulses, ABI > 0.9, negative CTA. |
| Joint Stability | Irreducible dislocation; gross instability post-reduction requiring spanning external fixation. | Stable concentric reduction achievable and maintainable in a knee immobilizer or hinged brace. |
| Soft Tissue | Open dislocation; impending compartment syndrome requiring fasciotomy. | Closed injury with manageable swelling; no signs of compartment syndrome. |
| Patient Factors | High-demand, medically stable patient fit for multi-ligament reconstruction. | Advanced age, severe medical comorbidities, low functional demand, or non-ambulatory status. |
| Definitive Treatment | Multi-ligament reconstruction (typically staged 2-3 weeks post-injury). | Prolonged bracing and physical therapy (rarely indicated except in unfit surgical candidates). |
Pre Operative Planning and Patient Positioning
Acute Clinical Evaluation and Vascular Assessment
Patients typically present with gross distortion of the knee architecture, profound swelling, and severe pain. However, if the knee has undergone spontaneous reduction, the limb may appear deceptively benign. Subtle signs such as mild abrasions, minimal effusion (due to capsular disruption allowing fluid extravasation), or subjective complaints of instability may be the only external indicators of a catastrophic injury.
Immediate closed reduction must be undertaken in the trauma bay without delaying for initial radiographs, especially if vascular compromise is suspected. Following reduction, the arterial supply becomes the paramount focus of the evaluation. A normal palpable pulse does not rule out an intimal tear that may subsequently thrombose. Therefore, objective measurement using the Ankle-Brachial Index (ABI) is mandatory. An ABI of less than 0.9, asymmetry in pulses, or any hard signs of vascular injury mandate immediate evaluation with CT Angiography (CTA) and urgent vascular surgery consultation. Ischemia time exceeding 6 to 8 hours is associated with amputation rates approaching 85%. Secondary consideration must be given to the neurologic status, specifically documenting common peroneal nerve function (ankle dorsiflexion, great toe extension, and sensation over the first dorsal webspace) prior to any intervention.
Ligamentous Examination and Imaging
Once the limb is perfused and stabilized, a comprehensive ligamentous examination is performed. Gross instability may only be fully realized after reduction, and muscle guarding can make acute assessment difficult.
* ACL: Lachman test at 30 degrees of flexion.
* PCL: Posterior drawer test at 90 degrees of flexion; posterior sag sign.
* LCL and PLC: Varus stress at 30 degrees and full extension; increased tibial external rotation at 30 degrees (Dial test); increased posterior tibial translation at 30 degrees.
* MCL: Valgus stress at 30 degrees and full extension.
Combined ligamentous injuries present with complex instability patterns. For example, combined LCL/PLC and cruciate injuries demonstrate increased varus in both full extension and at 30 degrees. Combined PLC and PCL injuries show increased tibial external rotation at both 30 and 90 degrees.
Standard orthogonal radiographs are obtained post-reduction to confirm concentric joint alignment and assess for associated fractures. Magnetic Resonance Imaging (MRI) is the gold standard for defining the exact soft-tissue injury pattern, typically obtained after acute stabilization once the patient is cleared for prolonged scanning. The Schenck Classification system is utilized to categorize the injury based on the MRI findings:
* KD I: Single cruciate injury with collateral involvement.
* KD II: ACL and PCL injury with intact collaterals.
* KD III: ACL, PCL, and one collateral ligament (KD III-M for medial, KD III-L for lateral).
* KD IV: Global disruption (ACL, PCL, MCL, LCL/PLC).
* KD V: Multi-ligament injury with periarticular fracture.
Patient Positioning and Operating Room Setup
For definitive reconstruction, the patient is positioned supine on a radiolucent operating table. A lateral thigh post or a specialized leg holder is utilized to allow full range of motion and valgus stress application. A non-sterile tourniquet is placed high on the proximal thigh. The contralateral leg is secured in well-padded lithotomy or flattened, depending on the need for autograft harvesting. Fluoroscopy must be readily available and positioned to easily enter the surgical field for tunnel trajectory confirmation.
Detailed Surgical Approach and Technique
Surgical management is generally divided into two phases: acute damage control and delayed definitive reconstruction.
Phase One Damage Control External Fixation
If the joint remains subluxated post-reduction, or if vascular repair has been performed, a spanning external fixator is applied to protect the vascular anastomosis and rest the soft tissues. Two 5.0 mm Schanz pins are placed in the anterior femur, and two are placed in the anteromedial tibia. The frame is constructed to hold the knee in 15 to 20 degrees of flexion, avoiding posterior subluxation of the tibia. The fixator is typically maintained for 2 to 3 weeks until the soft tissue envelope recovers, swelling subsides, and the patient is physiologically optimized for prolonged reconstructive surgery.
Phase Two Definitive Multi Ligament Reconstruction
Definitive reconstruction is generally preferred over primary repair, as repaired ligaments in the setting of massive trauma have an unacceptably high failure rate. Timing is critical; intervening between 2 to 3 weeks post-injury allows for capsular healing (preventing fluid extravasation during arthroscopy) while avoiding the severe arthrofibrosis associated with delayed treatment beyond 6 weeks.
Graft Selection and Preparation
Given the necessity to reconstruct multiple ligaments simultaneously, allograft tissue (e.g., Achilles tendon, tibialis anterior, or hamstring allografts) is heavily utilized to minimize donor-site morbidity and reduce operative time. Autograft (such as bone-patellar tendon-bone or quadriceps tendon) may be selectively used for the ACL in high-demand athletes. Grafts are prepared on the back table, tubularized, and pre-tensioned while the surgical approaches are performed.

Step by Step Reconstruction Sequence
The generally accepted sequence of reconstruction addresses the central pivot first, followed by the peripheral stabilizers: PCL → ACL → Lateral/PLC → Medial/MCL.
- Diagnostic Arthroscopy and Preparation: Standard anterolateral and anteromedial portals are established. The joint is cleared of hematoma and debris. Meniscal pathology is addressed via repair or partial resection. The anatomic footprints of the ACL and PCL are identified and debrided, preserving any viable remnant for proprioception.
- PCL Reconstruction: The PCL can be reconstructed via a transtibial endoscopic approach or an open tibial inlay technique. For the transtibial approach, a posteromedial portal is essential to protect the neurovascular bundle. A guide pin is placed at the PCL footprint on the posterior tibia, approximately 1 cm distal to the joint line. A reamer is passed, and the femoral tunnel is drilled inside-out at the anterolateral aspect of the medial femoral condyle. The graft is passed and secured.
- ACL Reconstruction: The tibial tunnel is drilled at the center of the ACL footprint, posterior to the anterior horn of the lateral meniscus. The femoral tunnel is drilled independently through an accessory anteromedial portal to ensure anatomic placement on the medial wall of the lateral femoral condyle.
- Lateral and Posterolateral Corner (PLC) Reconstruction: An open lateral approach is utilized. The internervous plane between the iliotibial (IT) band and the biceps femoris is developed. The common peroneal nerve is identified posterior to the biceps femoris and meticulously neurolysed and protected. The fibular head and the lateral femoral epicondyle are exposed. An anatomic reconstruction (e.g., the LaPrade technique) involves drilling a fibular tunnel, a tibial tunnel, and two femoral tunnels to reconstruct the LCL, popliteofibular ligament, and popliteus tendon using a bifurcated allograft.
- Medial Collateral Ligament (MCL) Reconstruction: An open medial approach is performed. The sartorius fascia is incised to expose the superficial MCL footprint. Femoral and tibial tunnels are created at the anatomic origins and insertions to reconstruct the superficial MCL and the posterior oblique ligament (POL).
- Fixation Sequence: Once all grafts are passed, fixation is performed in a specific sequence to restore anatomic alignment. The PCL is fixed first at 90 degrees of flexion with an anterior drawer force applied. The ACL is fixed next at full extension. The PLC is fixed at 30 degrees of flexion with a valgus and internal rotation force. Finally, the MCL is fixed at 30 degrees of flexion with a varus and internal rotation force.
Complications and Management
The management of femorotibial dislocations is fraught with severe complications, both from the initial trauma and the complex surgical interventions.
| Complication | Incidence | Pathophysiology and Salvage Management |
|---|---|---|
| Vascular Injury / Amputation | 5% to 15% (Amputation up to 85% if delayed) | Intimal tearing or transection of the popliteal artery. Requires emergent vascular bypass. If ischemia exceeds 8 hours, prophylactic fasciotomies are mandatory. Salvage for failed revascularization is above-knee amputation. |
| Common Peroneal Nerve Palsy | 10% to 40% | Stretch injury during varus/lateral dislocation. Often irreversible. Management includes acute neurolysis during PLC reconstruction. Salvage involves a rigid AFO or posterior tibial tendon transfer for foot drop. |
| Arthrofibrosis | 20% to 50% | The most common postoperative complication due to massive capsular scarring. Management relies on aggressive early ROM. Salvage includes arthroscopic lysis of adhesions and manipulation under anesthesia (MUA). |
| Compartment Syndrome | 5% to 10% | Secondary to ischemia-reperfusion injury or massive soft tissue trauma. Requires emergent four-compartment fasciotomy of the leg. |
| Graft Failure / Recurrent Instability | 10% to 20% | Results from unrecognized peripheral corner injuries, premature weight-bearing, or biologic failure. Requires revision reconstruction with allograft and potential osteotomy (e.g., HTO) to correct mechanical axis deviation. |
| Deep Infection | 2% to 5% | Associated with prolonged operative times and massive allograft burden. Requires emergent arthroscopic or open irrigation and debridement, targeted IV antibiotics, and potential graft removal if infection cannot be suppressed. |
Post Operative Rehabilitation Protocols
Rehabilitation following multi-ligament knee reconstruction is a delicate balance between protecting the healing grafts and preventing devastating arthrofibrosis. Protocols must be individualized based on the specific ligaments reconstructed.
- Phase 1: Maximum Protection (Weeks 0 to 6)
The patient is placed in a hinged knee brace locked in full extension. Weight-bearing is strictly non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) to protect the intra-articular and extra-articular grafts. Passive range of motion (PROM) is initiated early, typically restricted from 0 to 90 degrees. Prone ROM exercises are favored if the PCL was reconstructed to prevent posterior tibial sag. - Phase 2: Progressive Mobilization (Weeks 6 to 12)
The brace is unlocked to allow full ROM. Weight-bearing is progressively advanced to full weight-bearing by 8 to 10 weeks. Active-assisted range of motion is introduced, focusing on quadriceps activation and patellar mobilization. Closed kinetic chain exercises are initiated, but isolated hamstring curls are avoided if the PCL or PLC was reconstructed to prevent posterior sheer forces. - Phase 3: Strengthening and Proprioception (Months 3 to 6)
The brace is discontinued for daily activities. Rehabilitation focuses on progressive resistance training, core stability, and proprioceptive drills. Straight-line jogging may be introduced toward the end of this phase if quadriceps strength is at least 70% of the contralateral limb. - Phase 4: Return to Activity (Months 6 to 12+)
Advanced agility, plyometrics, and sport-specific drills are incorporated. Return to full sports or heavy labor is generally not permitted until 9 to 12 months postoperatively, contingent upon symmetrical ROM, stable ligamentous exam, and >90% limb symmetry index on functional hop testing and isokinetic strength evaluation.
Summary of Key Literature and Guidelines
The evolution of management for femorotibial dislocations has been shaped by several foundational studies and evolving clinical guidelines. Historically, non-operative management or simple immobilization was utilized, leading to uniformly poor functional outcomes and stiff, unstable joints.
The shift toward operative management was heavily influenced by the work of Schenck and others, who demonstrated superior outcomes with anatomic reconstruction. A landmark systematic review by Levy et al. clearly established that early definitive reconstruction (within 3 weeks) yields superior range of motion, functional scores, and stability compared to delayed reconstruction or primary repair. Furthermore, the use of spanning external fixation for damage control in the setting of vascular injury or gross instability has been validated by Stannard et al., who demonstrated a significant reduction in vascular repair failure and improved soft tissue outcomes.
Current guidelines from the Western Trauma Association mandate strict protocols for vascular screening. The routine use of the Ankle-Brachial Index (ABI) has largely replaced mandatory conventional angiography for all knee dislocations. An ABI > 0.9 with a normal physical exam has a nearly 100% negative predictive value for clinically significant arterial injury, sparing the patient unnecessary invasive imaging. However, any deviation in the ABI or physical exam mandates immediate CT Angiography.
In summary, femorotibial knee dislocation remains a highly complex orthopaedic emergency. Successful management relies on a high index of suspicion, rapid identification and treatment of vascular compromise, meticulous preoperative planning, and precise, staged surgical reconstruction followed by rigorous rehabilitation.
Clinical & Radiographic Imaging
