INJURIES OF THE FLEXOR TENDONS
Injuries to the flexor tendons of the foot and ankle are relatively uncommon when compared to the high incidence of pathology affecting the posterior tibial tendon and the peroneal tendons. However, flexor hallucis longus (FHL) tendinitis, stenosing tenosynovitis, and acute ruptures represent a distinct and highly debilitating class of injuries. These pathologies are intrinsically linked to posterior ankle pain, particularly in high-demand populations such as classical ballet dancers, gymnasts, and elite athletes. The complex biomechanics of the FHL, combined with its tortuous anatomical course through multiple fibroosseous tunnels, predisposes it to friction, impingement, and eventual structural failure.
Extensive investigations by Hamilton et al., Kolettis et al., and Sammarco et al. have elucidated the pathophysiology of these conditions, shifting the paradigm from prolonged conservative frustration to highly successful, targeted surgical interventions.
Flexor Hallucis Longus Tendinitis and Posterior Impingement
Pathoanatomy and Biomechanics
The FHL tendon originates from the posterior fibula and interosseous membrane, descending through a retromalleolar groove bordered by the medial and lateral tubercles of the posterior talus. It then enters a rigid fibroosseous tunnel beneath the sustentaculum tali. In activities requiring extreme plantar flexion—such as the en pointe or demi-pointe positions in ballet—the FHL tendon undergoes immense tensile and compressive loads. This repetitive mechanical stress can lead to tenosynovitis, hypertrophy of the tendon, and the formation of intratendinous nodules. As the tendon hypertrophies, a size mismatch occurs between the tendon and the unyielding fibroosseous tunnel, resulting in stenosing tenovaginitis and functional tethering (hallux saltans).
Clinical Evaluation and Diagnosis
A meticulous physical examination is paramount to differentiate between posterior ankle compression syndrome (osseous impingement) and FHL tendinitis (soft-tissue tethering), though the two frequently coexist.
- Posterior Compression Syndrome: Typically involves an elongated trigonal process (Stieda process) or an enlarged, unfused os trigonum in the posterior aspect of the ankle. Pain is reliably reproduced with forced, passive plantar flexion of the ankle, which pinches the osseous structures between the posterior tibia and the calcaneus.
- FHL Tendinitis / Stenosing Tenosynovitis: Characterized by insidious pain localized posterior to the medial malleolus. It is frequently misdiagnosed as posterior tibial tendinitis. The FHL tendon can be palpated deep and posterior to the medial malleolus.
Clinical Pearl: The hallmark diagnostic maneuver for FHL tendinitis is the reproduction of pain with passive extension of the great toe while simultaneously applying manual compression over the posteromedial tendon sheath of the FHL at the posterior aspect of the ankle.
According to Hamilton et al., the diagnosis of osseous posterior compression syndrome can be confirmed via a diagnostic injection of local anesthetic. The injection is administered through a posterolateral approach directly into the region of the posterior process of the calcaneus. Complete relief of pain with forced plantar flexion confirms the osseous impingement component.
Imaging Modalities:
* Magnetic Resonance Imaging (MRI): Highly sensitive for soft-tissue pathology. MRI often demonstrates fluid distension within the FHL tendon sheath, tenosynovitis, and occasionally intratendinous degenerative tears or nodule formation.
* Radiographs: Plain lateral standing radiographs of the ankle are essential for evaluating the osseous anatomy. They help differentiate a painful, cystic os trigonum from isolated FHL tendinitis.
* Bone Scintigraphy (Technetium-99m): Occasionally utilized to differentiate the two entities; focal radiotracer uptake is highly suggestive of a symptomatic os trigonum or a fractured trigonal process rather than isolated tendinopathy.
Nonoperative Management
Conservative management is the first line of treatment but is notoriously recalcitrant in professional athletes. Modalities include:
* Strict rest and immobilization in a controlled ankle motion (CAM) boot.
* Modification of dance technique or sporting activity.
* Oral nonsteroidal anti-inflammatory drugs (NSAIDs).
* Judicious use of localized corticosteroid injections (injected into the sheath, never intratendinously, to avoid iatrogenic rupture).
Indications for Surgical Intervention
The literature demonstrates a high failure rate for conservative treatment in elite performers. Hamilton et al. and Sammarco et al. found that nonoperative management was uniformly unsuccessful in returning professional dancers to their previous level of performance. In Sammarco’s cohort of 31 FHL injuries, 27 required surgical release. Following surgical decompression, good or excellent results were achieved in 88% of patients.
Similarly, Kolettis et al. reported considerable pain improvement in 100% of their surgical cohort. Michelson and Dunn noted that while conservative management succeeded in 64% of the general population, all patients who eventually required surgical release of the posterior ankle fibroosseous tunnel achieved satisfactory outcomes.
Surgical Warning: Hamilton et al. strongly recommend a medial approach when addressing combined FHL tendinitis and posterior osseous impingement. The lateral approach should be strictly reserved for isolated posterior osseous impingement without FHL tendinopathy, as the fibroosseous tunnel cannot be safely or completely released from the lateral side without risking neurovascular injury.
Surgical Technique: Release of Fibroosseous Tunnel (Hamilton et al.)
The Medial Approach (For Combined Tendinitis and Impingement)
- Positioning and Incision: Place the patient supine with the leg externally rotated. Make a 4-cm curvilinear incision posterior to the medial malleolus at the level of the superior border of the calcaneus. The incision should follow the anatomical course of the underlying posterior tibial neurovascular bundle.
- Neurovascular Protection: Carefully dissect through the subcutaneous tissues. Identify the posterior tibial neurovascular bundle and retract it posteriorly using a blunt retractor (e.g., a Ragnell or mini-Hohmann).
- Tunnel Identification and Release: Identify the underlying FHL fibroosseous tunnel. Confirm the tendon by having an assistant passively flex and extend the great toe. Incise the retinaculum and release the tunnel from proximal to distal, extending down to the level of the sustentaculum tali. Débride any hypertrophic tenosynovium.
-
Handling Tendon Nodules:

Fig. 85-39 A, Flexor hallucis longus constricted at entrance of fibroosseous tunnel. Tendon is completely free with ankle and great toe in neutral. Flexor digitorum longus anterior to flexor hallucis longus.
Fig. 85-39 B, Large nodule within fibroosseous tunnel. Despite size of nodule, there is free excursion of tendon after release of tunnel.Nodules on or within the FHL tendon are generally not excised. Once the unyielding fibroosseous tunnel has been completely released, the excursion of the tendon is no longer restricted, and the nodule will pass freely without triggering hallux saltans.
5. Intraoperative Dynamic Assessment: Evaluate for functional hallux rigidus intraoperatively. Passively dorsiflex the ankle and extend the great toe to ensure complete release and unimpeded excursion of the tendon.
6. Osseous Decompression: Retract the released FHL tendon posteriorly along with the neurovascular bundle. Identify and excise the os trigonum or hypertrophic trigonal process located on the lateral side of the entrance to the fibroosseous tunnel.
7. Final Impingement Check: Examine the ankle in full, forced plantar flexion. Palpate the posterior compartment to ensure no residual bone-on-bone or soft-tissue impingement remains.
8. Closure: The ankle must be held in a neutral position (0 degrees of flexion/extension) during skin closure to ensure proper skin tension and alignment, preventing postoperative wound contractures.
The Lateral Approach (For Isolated Posterior Impingement)
- Positioning: Because dancers often have increased external rotation of the lower extremities, the patient should be placed in a true lateral decubitus position to allow adequate visualization of the posterolateral ankle.
- Incision: Make a curvilinear incision at the posterolateral aspect of the ankle mortise, directly in line with the posterior border of the peroneal tendons.
- Nerve Protection: Perform meticulous superficial dissection to identify and protect the sural nerve, which is highly vulnerable in this approach.
- Capsulotomy and Excision: Perform a posterior capsulotomy with the ankle held in slight dorsiflexion. Identify the lateral tubercle of the posterior talus or the os trigonum, which lies lateral to the FHL tunnel. Excise the offending osseous structure.
- Decompression Assessment: Assess for adequate osseous decompression by forcefully plantar flexing the foot and palpating for any residual impingement. Débride any loose bodies, calcaneal protuberances, or osteophytes from the posterior tibial plafond as necessary.
Postoperative Rehabilitation Protocol
- 0-1 Week: Apply a bulky, sterile compression dressing and a posterior splint. The patient is allowed weight-bearing as tolerated (WBAT) with the assistance of crutches.
- 1 Week: The surgical dressing is removed. Active range of motion (AROM) of the ankle and great toe is initiated immediately as pain tolerance permits to prevent tendon adhesions.
- 2 Weeks: Formal physical therapy commences. This includes progressive active and passive range-of-motion exercises, intrinsic foot strengthening, and proprioceptive training. Swimming or deep-water running is highly encouraged once the surgical wound is completely epithelialized.
- Return to Play: The patient progresses to higher levels of sport-specific or dance-specific activity under the strict supervision of a specialized physical therapist. An average of 6 months should be expected for full recovery and return to elite performance levels.
Flexor Hallucis Longus Tear
Indications and Controversies
Acute ruptures of the FHL are rare and typically occur proximal to the metatarsophalangeal (MTP) joint. If the tendon is torn such that the repair site will not glide smoothly through the complex plantar pulley system, primary repair may be justified. However, surgical exposure on the plantar surface of the forefoot, proximal to the MTP joint, is anatomically demanding.
Surgical Pitfall: We generally do not recommend repairing the FHL tendon within the pulley system of the hallux. If the flexor hallucis brevis (FHB) remains intact in the forefoot-midfoot area, the patient will retain adequate push-off strength, and primary repair of the FHL is likely unnecessary for functional recovery.
If the surgeon and patient elect to proceed with primary repair (e.g., in an elite athlete requiring maximal distal phalangeal flexion), the approach described by Floyd, Heckman, and Rockwood is recommended.
Surgical Technique: Plantar Approach for FHL Repair
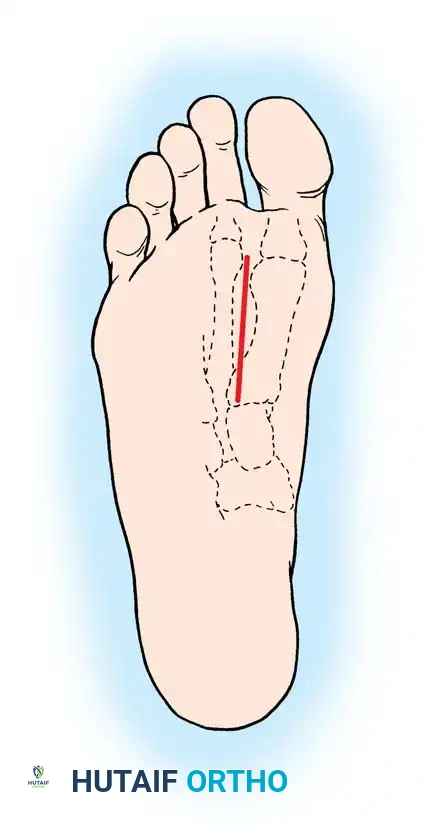
Fig. 85-40 Incision on plantar surface of foot for repair of flexor hallucis longus.
- Incision: Begin with a plantar longitudinal incision on the sole of the foot, positioned between the first and second metatarsals, just lateral and distal to the fibular sesamoid. Extend this incision proximally for 4 to 5 cm.
- Superficial Dissection: Bluntly dissect and remove the fibrous connections between the slips of the plantar fascia extending to the first and second toes.
-
Neurovascular Isolation:

Fig. 85-41 1, Medial proper branch of medial plantar nerve to tibial side of hallux; 2, common digital branch of medial plantar nerve to first web; 3, flexor hallucis longus tendon.Using small, blunt-tipped dissecting scissors (e.g., tenotomy scissors), carefully expose the common digital nerve and its accompanying vessels leading to the first web space. Gently retract these neurovascular structures laterally and distally to protect them throughout the procedure.
4. Deep Exposure:
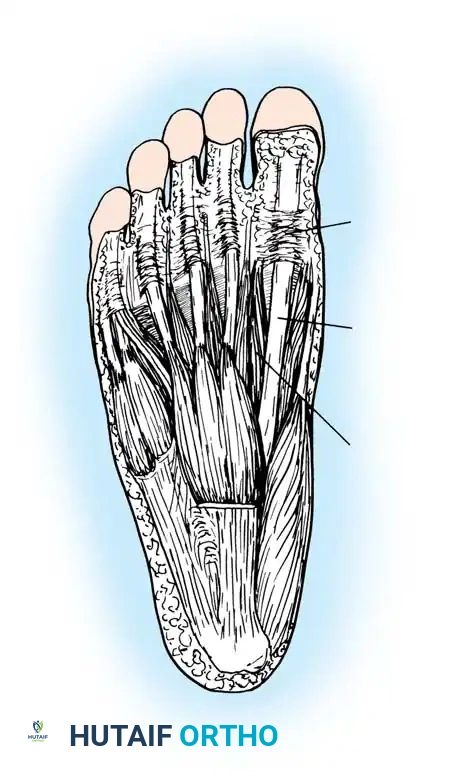
Fig. 85-42 1, Pulley of flexor hallucis longus at first metatarsophalangeal joint; 2, flexor hallucis longus; 3, lateral head of flexor hallucis brevis.Identify and expose the lateral head of the flexor hallucis brevis (FHB) tendon. Develop the internervous/intermuscular plane between the two muscle bellies of the FHB throughout the length of the surgical wound.
5. Tendon Retrieval: Acutely flex the great toe to deliver the distal tendon stump into the surgical field. The proximal stump often retracts but is usually tethered by the Master Knot of Henry (the cross-connection with the flexor digitorum longus). Use a tendon passer or a curved hemostat to probe proximally along the tendon sheath with the ankle held in equinus. Dark hematoma or organized scar tissue will often guide the surgeon to the retracted proximal stump.
6. Tenorrhaphy: Once both tendon ends are mobilized into the wound, maintain the ankle in plantar flexion. Pass a straight needle through the skin, through the proximal FHL tendon, and out the contralateral skin to temporarily anchor it. Flex the great toe to relieve tension, and perform a primary end-to-end repair using a double right-angle (e.g., Krackow or modified Kessler) stitch with 2-0 nonabsorbable suture on a tapered, atraumatic needle.
* Crucial Step: Do not "accordion" or bunch the tendon any more than is strictly necessary to achieve secure approximation. Excessive bunching will prevent the tendon from gliding through the pulley system.
7. Closure: Close the plantar skin with 2-0 or 3-0 nylon. Simple interrupted sutures are preferred, though vertical mattress sutures are acceptable if the skin edges tend to invert.
8. Immobilization: Apply a bulky soft-tissue dressing and place the patient in a short leg cast. The ankle should be immobilized in mild equinus, with the hallux held in a neutral position. The cast must extend distal to the toes to protect the repair.
Postoperative Management for FHL Repair
- 0-3 Weeks: The patient is strictly non-weight-bearing (NWB) with the ankle immobilized in mild equinus.
- 3-6 Weeks: The initial cast is removed. The foot is brought to a neutral position at the ankle, and a new short leg walking cast (extending past the toes) is applied. Weight-bearing to tolerance (WBAT) is permitted. Sutures are removed at this stage.
- 6+ Weeks: The walking cast is discontinued. Active toe flexion is initiated. The patient should perform isolated interphalangeal and metatarsophalangeal joint flexion exercises while manually blocking the adjacent joint. If the repair was performed 2 cm or more proximal to the MTP joint, the patient should eventually recover independent interphalangeal joint flexion.
Flexor Digitorum Longus Tendon
Management Principles
The flexor digitorum longus (FDL) tendon plays a secondary role in digital flexion, heavily assisted by the quadratus plantae and the intrinsic musculature of the foot. Consequently, primary repair of an isolated injury to the FDL in the toes or the midfoot is generally not indicated, as the functional deficit is negligible and the risk of postoperative tethering and stiffness outweighs the benefits.
However, surgical exploration and repair are indicated in the setting of a massive, deep plantar laceration near the midfoot-hindfoot junction. If the laceration occurs proximal to the junction of the quadratus plantae and the FDL, and the FHL is concomitantly lacerated (which is almost universally associated with medial or lateral plantar nerve transection), then the FDL should be repaired in conjunction with the primary neurovascular and FHL reconstruction to restore global plantar function.
