Incision and Drainage of a Felon: Advanced Surgical Techniques and Protocols
Key Takeaway
A felon is a closed-space infection of the distal digital pulp, characterized by severe throbbing pain and swelling. Surgical management requires precise incision and drainage to decompress the pulp space and prevent ischemic necrosis or osteomyelitis. The approach—whether a volar midline or a lateral longitudinal incision—depends on the abscess location. Meticulous blunt dissection is essential to disrupt the fibrous septa while preserving the digital neurovascular bundles.
Introduction to Digital Felons
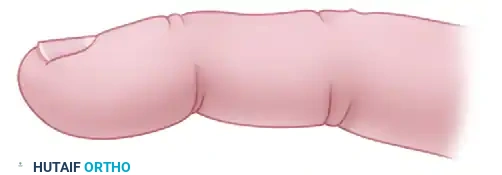
A felon is a highly localized, exquisitely painful abscess located within the subcutaneous tissues of the distal digital pulp of a finger or thumb. Recognized as a true surgical emergency in hand orthopaedics, a felon represents a micro-compartment syndrome of the distal phalanx. The unique microanatomy of the digital pulp makes it particularly susceptible to rapid pressure accumulation, leading to severe throbbing pain, microvascular compromise, and, if left untreated, devastating complications such as ischemic necrosis of the pulp, osteomyelitis of the distal phalanx, or purulent flexor tenosynovitis.
The primary pathogen responsible for a felon is typically Staphylococcus aureus, often introduced via a minor penetrating trauma, such as a splinter, thorn, or needle stick. However, in immunocompromised patients, diabetics, or those with specific occupational exposures, atypical organisms including Gram-negative bacilli or mixed flora may be cultured.
Successful management of a felon hinges on prompt clinical recognition, accurate differentiation from other digital infections (such as herpetic whitlow or paronychia), and precise surgical decompression. The surgical approach must be meticulously planned to ensure adequate drainage while strictly avoiding iatrogenic injury to the terminal arborizations of the digital nerves and arteries.
Surgical Anatomy and Biomechanics of the Distal Pulp
To master the surgical management of a felon, the orthopaedic surgeon must possess an intimate understanding of the distal digital pulp's anatomy.
The distal pulp is not a single, homogenous subcutaneous space. Instead, it is a highly specialized, shock-absorbing structure divided into 15 to 20 discrete micro-compartments. These compartments are formed by dense, inelastic fibrous septa (the septa of Legueu and Juvara) that extend vertically from the periosteum of the distal phalanx to the deep dermis of the volar skin.
Pathophysiology of the Micro-Compartment Syndrome
When bacteria are inoculated into one of these closed spaces, the resulting inflammatory exudate and edema have no avenue for expansion. The inelastic fibrous septa restrict swelling, causing a rapid exponential rise in interstitial pressure.
- Microvascular Ischemia: As pulp pressure exceeds capillary perfusion pressure, local tissue ischemia ensues, accelerating tissue necrosis and abscess formation.
- Osteomyelitis Risk: Because the fibrous septa anchor directly to the periosteum of the distal phalanx, the infection can easily track proximally along these septa, leading to periostitis and subsequent osteomyelitis of the tuft.
- Vascular Anatomy: The digital arteries bifurcate near the distal interphalangeal (DIP) joint. The terminal branches run distally within the pulp space. Excessive pressure or careless sharp surgical dissection can compromise these vessels, leading to catastrophic fingertip sloughing.
Clinical Pearl: The diaphyseal blood supply to the distal phalanx runs directly through the pulp space. Consequently, a neglected felon frequently results in osteomyelitis or avascular necrosis of the distal phalangeal diaphysis, while the epiphyseal base (supplied by branches proximal to the pulp space) is typically spared.
Clinical Evaluation and Differential Diagnosis
Patients typically present with a history of minor trauma followed by 2-3 days of escalating, throbbing pain that is often severe enough to disrupt sleep. The distal pulp will be tense, erythematous, and exquisitely tender. As the abscess coalesces, a discrete area of fluctuance or visible pointing (often volarward) may become apparent.
The Critical Differential: Herpetic Whitlow
Before proceeding with any surgical intervention, the surgeon must definitively rule out herpetic whitlow.
🚨 Surgical Warning: Incision and drainage of a herpetic whitlow is strictly contraindicated. Surgical intervention in the presence of the Herpes Simplex Virus (HSV) can lead to viral dissemination, severe secondary bacterial superinfection, and delayed healing.
Differentiating Factors:
* Herpetic Whitlow: Presents with grouped, clear or cloudy vesicles on an erythematous base. The pain often precedes the swelling, and the pulp is usually less tense than in a felon.
* Felon: Presents with a tense, indurated, and highly pressurized pulp space. Vesicles are absent unless secondary to severe epidermal blistering from underlying necrosis.
Preoperative Preparation
Anesthesia
Adequate anesthesia is paramount, as the distal pulp is densely innervated. A digital block using 1% or 2% Lidocaine without epinephrine, or Bupivacaine for prolonged postoperative analgesia, is the standard of care. The block should be administered at the level of the proximal phalanx or metacarpal head to avoid introducing additional volume and pressure into the already compromised distal digit.
Positioning and Hemostasis
The patient is positioned supine with the affected hand extended on a radiolucent hand table. A digital tourniquet (such as a sterile Penrose drain clamped at the base of the finger) or a pneumatic forearm tourniquet is utilized to provide a bloodless surgical field. This is critical for identifying the digital nerves and ensuring all fibrous septa are adequately visualized and released.
Surgical Approaches: Incision and Drainage
The choice of surgical incision is dictated entirely by the location and pointing of the abscess. The overarching goals are to provide dependent drainage, decompress the micro-compartments by dividing the fibrous septa, and avoid painful scarring on the tactile surface of the digit.
1. The Volar Midline Approach (For Volar-Pointing Abscesses)
When the abscess points directly volarward, often causing localized ischemia or frank necrosis of the overlying skin, a volar approach is indicated.
- Necrotic Presentation: If the overlying skin is already necrotic, the abscess is drained by sharply excising the necrotic skin ellipse. This provides immediate decompression and removes non-viable tissue that would otherwise serve as a nidus for ongoing infection.
- Non-Necrotic Volar Pointing: When the abscess is located in the distal pulp area and points volarward toward the whorl of the fingerprint, it is best drained via a vertical midline incision.
Technique:
1. Begin the incision distal to the distal interphalangeal (DIP) skin crease.
2. Place the incision precisely in the midline of the volar pad.
3. This precise midline placement is critical to avoid the lateral arborizing branches of the digital nerve.
4. A midline scar in the whorl of the fingerprint generally heals with minimal functional impairment or painful scarring, provided it does not cross the DIP flexion crease.

FIGURE 78-5: Midline vertical incision for drainage of an abscess pointing volarward in the distal pulp of the finger. Note the precise midline placement to avoid lateral nerve branches.
2. The Lateral Longitudinal Approach (For Deep or Multi-Septated Abscesses)
If the abscess is deep, diffuse, and heavily partitioned by the fibrous septa without a clear volar pointing, a lateral longitudinal incision is the gold standard. This approach keeps the scar entirely away from the highly tactile volar contact area of the finger.
Technique:
1. Incision Placement: The incision must be highly accurate. Make the incision on the ulnar aspect of digits II, III, and IV, and the radial aspect of the thumb and digit V (to avoid the primary pinch contact surfaces).
2. Dorsal Orientation: The incision must be placed dorsal to the tactile surface of the finger.
3. Nail Margin Proximity: Keep the incision not more than 3 mm from the distal free edge of the nail.
Lateral view demonstrating the planned incision line. The approach must remain posterior to the digital artery and nerve to prevent iatrogenic injury.
Pitfall: If the lateral incision is placed too far volar (palmar), the terminal ends of the digital nerve will be painfully transected, resulting in a debilitating, painful neuroma on the gripping surface of the digit.
- The J-Shaped Modification: A unilateral longitudinal incision can be extended distally along the hyponychium to form a "J-shaped" incision if broader exposure is required. A J-shaped incision is generally sufficient for even complex felons.
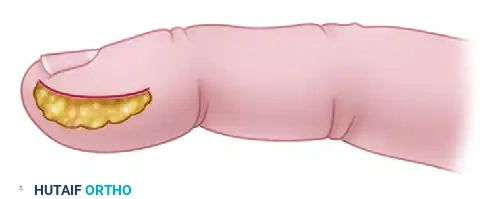
FIGURE 78-6: The J-shaped lateral incision. This provides excellent exposure of the deep pulp space while sparing the volar tactile pad.
🚨 Surgical Warning: The Fishmouth Incision
Historically, a "fishmouth" incision (a continuous U-shaped incision around the entire fingertip connecting both lateral sides) was advocated. This is now universally condemned. A fishmouth incision is notoriously slow to heal, devascularizes the volar pad, and frequently results in an unstable, highly painful, and functionally devastating scar.
3. Deep Dissection and Septal Release
Once the skin is incised, the most critical step of the procedure begins: the disruption of the fibrous septa.
- Avoid Sharp Dissection Deep in the Pulp: Do not plunge a scalpel deep into the pulp space. Sharp dissection risks severing the digital artery or the terminal nerve branches.
- Blunt Septal Disruption: Introduce the tip of small, curved tenotomy scissors or a fine mosquito hemostat into the incision.
- Spreading Technique: Gently spread the instrument longitudinally to bluntly disrupt the fibrous septa. You will feel the septa give way. This action connects the isolated micro-compartments, converting a multi-loculated abscess into a single cavity for effective drainage.
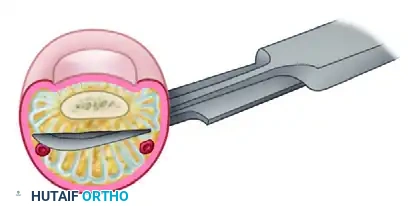
Cross-sectional anatomy demonstrating the blunt division of all fibrous septa. Note that the dissection remains posterior to the digital artery and nerve bundles (shown in red and yellow).
- Debridement: Evacuate all purulent material. Send a swab or tissue sample for aerobic and anaerobic culture and sensitivity. Gently debride any frankly necrotic fat, but be conservative to preserve pulp volume.
4. Irrigation and Packing
- Copious Irrigation: Irrigate the decompressed pulp space copiously with sterile normal saline. The use of a syringe with a blunt angiocatheter can help flush out deep loculations.
- Wound Packing: The wound must not be allowed to close prematurely, as this will lead to immediate re-accumulation of the abscess. Pack the cavity loosely with a small wick of iodoform gauze or a sterile plain gauze strip. The packing should be sufficient to keep the wound edges apart but not so tight that it recreates a compartment syndrome or causes pressure necrosis.
Postoperative Care and Rehabilitation
The postoperative management of a felon is as critical as the surgical decompression itself.
Immediate Postoperative Phase (0-48 Hours)
- Immobilization: The affected digit, and often the adjacent digit, should be immobilized in a bulky, soft dressing and a volar splint in a safe position (intrinsic plus) to provide rest to the inflamed tissues.
- Elevation: Strict elevation of the hand above the level of the heart is mandatory to minimize postoperative edema, reduce throbbing pain, and optimize microvascular perfusion.
- Packing Removal: The initial surgical bandage and the gauze packing are typically removed at approximately 48 hours postoperatively. This is often done in the clinic setting.
Subacute Phase and Wound Healing
- Hydrotherapy / Soaks: Once the packing is removed, the patient is instructed to begin warm saline or dilute chlorhexidine soaks 2 to 3 times daily. This promotes continuous drainage, mechanically debrides fibrinous exudate, and prevents premature closure of the skin edges.
- Secondary Intention: The wound is left open to heal by secondary intention. Suturing a felon drainage site is strictly contraindicated.
- Rehabilitation: Active range-of-motion (ROM) exercises of the DIP, PIP, and MCP joints are initiated immediately after the packing is removed to prevent tendon adhesions and joint stiffness. Edema control (e.g., Coban wrapping once drainage ceases) and gradual reincorporation of the finger into activities of daily living are heavily emphasized.
Antimicrobial Therapy
While surgical drainage is the definitive treatment, adjunctive antibiotic therapy is required to treat the surrounding cellulitis and eradicate residual bacteria.
- Empiric Therapy: Empiric antibiotic treatment with first-generation cephalosporins (e.g., Cephalexin) is usually sufficient for community-acquired, methicillin-susceptible Staphylococcus aureus (MSSA).
- MRSA Coverage: In regions with high rates of community-acquired Methicillin-resistant Staphylococcus aureus (MRSA), or in patients with a history of MRSA, empiric coverage should be broadened to include Trimethoprim-Sulfamethoxazole, Clindamycin, or Doxycycline.
- Culture-Directed Therapy: Changes in antibiotic therapy must be made promptly on the basis of the results of intraoperative culture and sensitivity studies.
Special Populations: Diabetics and the Immunosuppressed
Infections in patients with poorly controlled diabetes mellitus, peripheral vascular disease, or systemic immunosuppression present a formidable clinical challenge.
In these populations, the microvascular reserve is already compromised. A felon can rapidly progress to extensive gangrene or deep space infections of the hand. These patients require aggressive surgical debridement, broad-spectrum intravenous antibiotics, and tight glycemic control. Despite optimal management, infections in these vulnerable cohorts may be exceedingly difficult to control, and terminal amputation of the digit may ultimately be the required end result to prevent systemic sepsis. Close, frequent outpatient follow-up is mandatory until the wound is completely epithelialized.
You Might Also Like
