Tibial Plateau Fractures: Comprehensive Classification and Surgical Management

Key Takeaway
Tibial plateau fractures represent complex intra-articular injuries requiring meticulous anatomical reduction and stable fixation. The Schatzker classification remains the gold standard for guiding surgical strategy, categorizing fractures from pure lateral cleavage to complex bicondylar dissociation. Successful management hinges on understanding the injury biomechanics, utilizing advanced imaging, selecting the optimal surgical approach, and executing precise osteosynthesis to restore joint congruity and mechanical alignment while respecting the delicate soft-tissue envelope.
INTRODUCTION TO TIBIAL PLATEAU FRACTURES
Tibial plateau fractures are formidable intra-articular injuries that challenge the orthopedic surgeon to restore joint congruity, axial alignment, and knee stability while meticulously managing a frequently compromised soft-tissue envelope. These fractures encompass a broad spectrum of pathology, ranging from low-energy, minimally displaced fractures in osteoporotic individuals to devastating, high-energy bicondylar injuries with extensive diaphyseal comminution.
The ultimate goal of operative intervention is to achieve a stable, well-aligned, and congruent joint that permits early range of motion, thereby minimizing the risk of post-traumatic osteoarthritis and arthrofibrosis. To achieve this, a profound understanding of fracture biomechanics, classification systems—specifically the Schatzker and the Hohl and Moore classifications—and contemporary surgical approaches is mandatory.
BIOMECHANICS AND MECHANISM OF INJURY
The morphology of a tibial plateau fracture is dictated by the magnitude and direction of the applied force, the position of the knee at the time of impact, and the underlying bone quality. The primary deforming forces are axial loading combined with either valgus or varus stress.
Because the lateral tibial plateau is convex and slightly higher than the concave medial plateau, and because the mechanical axis of the lower extremity naturally places a valgus vector across the knee, lateral plateau fractures are significantly more common than medial ones.
Clinical Pearl: Always assess the soft-tissue envelope and ligamentous stability. Tibial collateral ligament (TCL) and medial collateral ligament (MCL) injuries commonly occur in split and mixed fractures of the lateral plateau due to the valgus opening of the medial joint space.
The relationship of force to specific fracture patterns is highly predictable:
Baseline valgus force with the Tibial Collateral Ligament (TCL) intact.

Split fracture: Often resulting from a valgus force driving the lateral femoral condyle into the lateral plateau.

Local depression: Often caused by a compression force, frequently with the knee in extension.

Mixed (Split-Depression): A combination of compression and valgus forces.
Ultimate fracture by valgus: Severe lateral comminution with potential medial ligamentous rupture.

Total depression: Typically resulting from a massive, pure compression force. Proximal fibular fracture or proximal tibiofibular diastasis frequently occurs.
Bicondylar fracture: The result of high-energy axial compression combined with varus/valgus moments, splitting both condyles.
THE SCHATZKER CLASSIFICATION SYSTEM
The Schatzker classification is the most universally adopted system for categorizing tibial plateau fractures. It divides these injuries into six distinct types based on fracture pattern and pathoanatomy, directly guiding the surgical approach and fixation strategy. Types I through III typically represent lower-energy injuries isolated to the lateral plateau, whereas Types IV through VI represent high-energy, complex injuries.
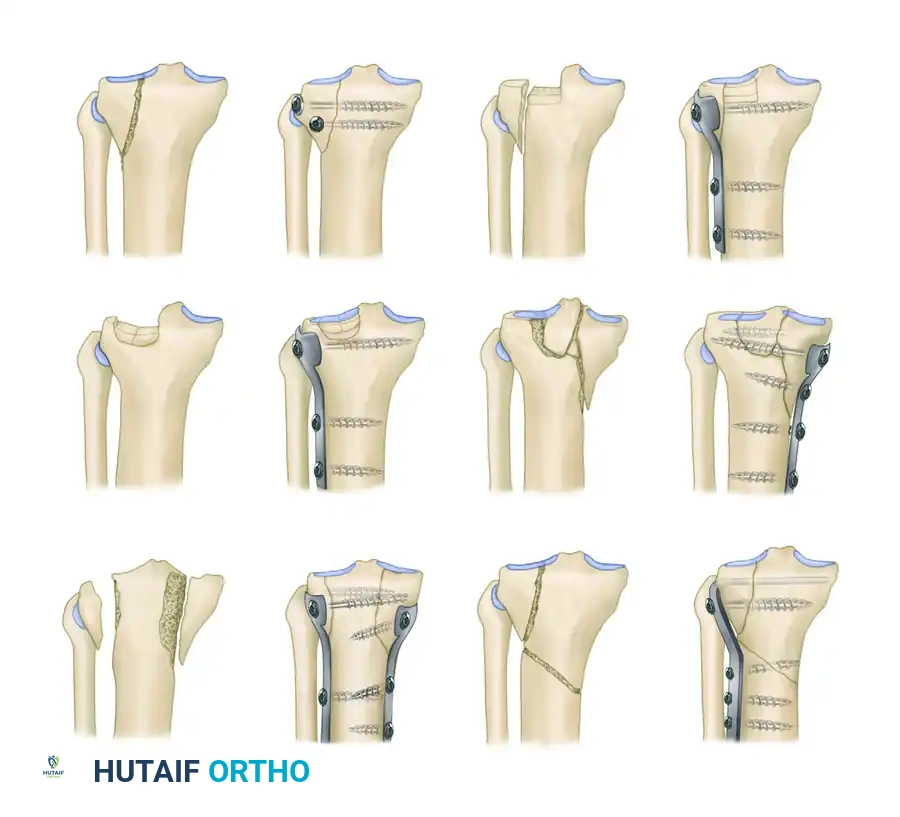
Surgical Diagram of the Schatzker Classification (Types I through VI).
Type I: Pure Cleavage
A typical wedge-shaped, uncomminuted fragment is split off and displaced laterally and downward.
* Pathoanatomy: This fracture is common in younger patients without osteoporotic bone. The dense cancellous bone resists depression, resulting in a pure split.
* Treatment: If displaced, it can be fixed with two transverse cancellous lag screws. If the fragment is large or highly unstable, a small antiglide or buttress plate is recommended to prevent shear displacement.
Type II: Cleavage Combined with Depression
A lateral wedge is split off, but in addition, the articular surface is depressed into the metaphyseal cancellous bone.
* Pathoanatomy: This is the most common tibial plateau fracture, typically seen in patients in their fourth decade or older with early osteoporotic changes. The lateral femoral condyle acts as a hammer, driving the articular cartilage into the metaphysis.
* Treatment: Requires elevation of the depressed articular segment, bone grafting (autograft, allograft, or synthetic bone void filler) of the resulting metaphyseal defect, and stabilization with a lateral buttress plate and subchondral raft screws.
Type III: Pure Central Depression
The articular surface is depressed into the intact lateral metaphyseal rim.
* Pathoanatomy: Occurs almost exclusively in older individuals with severe osteoporosis. The lateral rim remains intact, but the central articular cartilage is crushed downward.
* Treatment: If the depression is significant (typically >5 mm) or causes mechanical axis deviation, it requires a cortical window for elevation, bone grafting, and raft screw fixation.
Type IV: Medial Plateau Fracture
A fracture of the medial tibial condyle, which may be a split or a comminuted depression.
* Pathoanatomy: This is a high-energy injury resulting from varus and axial compression. Because the medial plateau is denser and stronger than the lateral plateau, it requires significant force to fracture.
* Surgical Warning: Type IV fractures carry a high association with popliteal artery injuries, peroneal nerve damage, and severe ligamentous disruption (knee dislocation equivalent).
* Treatment: Requires a posteromedial approach and rigid buttress plating.
Type V: Bicondylar Fracture
Fracture of both the medial and lateral tibial condyles, often with an inverted "Y" pattern leaving the tibial eminence separated from the diaphysis.
* Pathoanatomy: High-energy axial loading. Both condyles are fractured, but the metaphysis remains in continuity with the diaphysis.
* Treatment: Requires dual plating (medial and lateral) or a combination of lateral plating and a medial external fixator to restore the mechanical axis and joint congruity.
Type VI: Plateau Fracture with Metaphyseal-Diaphyseal Dissociation
A transverse or oblique fracture of the proximal tibia is present in addition to a fracture of one or both tibial condyles and articular surfaces.
* Pathoanatomy: The most severe high-energy injury. The dissociation of the diaphysis and metaphysis makes this fracture highly unstable and entirely unsuitable for treatment in traction.
* Treatment: Most should be treated with robust buttress plates and cancellous screws, one on either side if both condyles are fractured. Pin and wire circular fixators (e.g., Ilizarov or Taylor Spatial Frame) have also been strongly advocated for the fixation of these difficult fractures, particularly when the soft tissue envelope precludes extensive dual incisions.
THE HOHL AND MOORE CLASSIFICATION
While the Schatzker system is ubiquitous, the classification of intra-articular proximal tibial fractures originally proposed by Hohl and later modified by Moore and Hohl is also commonly used and provides critical insights, particularly regarding fracture-dislocations.
The classification distinguishes between five primary fracture patterns and five fracture-dislocation patterns (with fracture-dislocations occurring one-seventh as frequently as fractures). Hohl observed that this classification serves as an intermediate step in the evolution of a system that separates the myriad ligamentous and soft tissue injuries that, along with the bony injury, determine the ultimate clinical outcome.
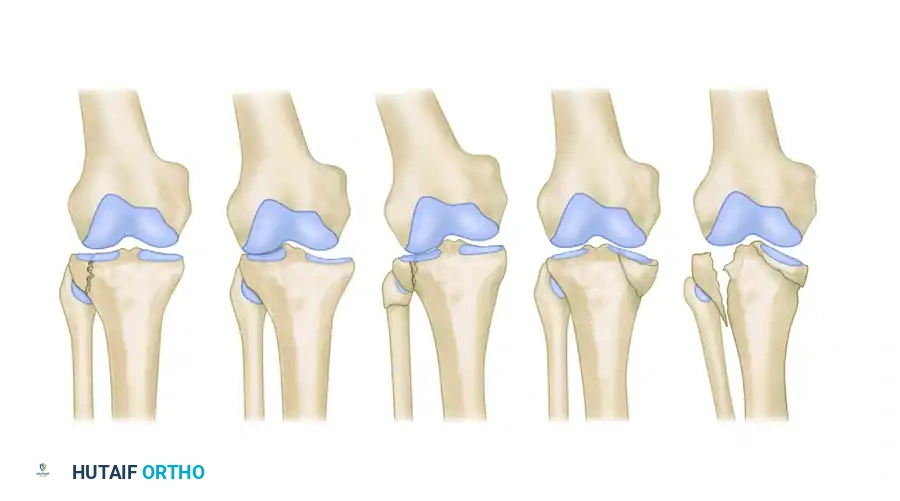
Classification of tibial plateau fractures as described by Hohl and Moore: type 1, minimally displaced; type 2, local compression; type 3, split compression; type 4, total condyle; and type 5, bicondylar.
Hohl and Moore Fracture Patterns
- Type 1 (Minimally Displaced): Fractures with less than 4 mm of depression or displacement. Often amenable to conservative management or percutaneous fixation.
- Type 2 (Local Compression): Analogous to a central depression without a peripheral split.
- Type 3 (Split Compression): Analogous to the Schatzker Type II, featuring both a cleavage plane and articular depression.
- Type 4 (Total Condyle): Involves the entire medial or lateral condyle, often with a fracture line exiting through the opposite intercondylar eminence.
- Type 5 (Bicondylar): Involves both condyles with varying degrees of comminution.
Surgical Pitfall: Involvement with level I trauma centers has shown that several extremely high-energy fractures—frequently open—defy conventional classification and treatment methods. These usually include bicondylar comminution combined with extensive shaft comminution, requiring highly individualized, damage-control orthopedic strategies.
PREOPERATIVE EVALUATION AND IMAGING
A meticulous preoperative assessment is the cornerstone of successful management.
Clinical Examination
- Soft Tissue Envelope: Assess for fracture blisters, abrasions, and open wounds. The presence of severe swelling or hemorrhagic blisters dictates a delay in definitive internal fixation.
- Neurovascular Status: The popliteal artery is tethered at the adductor hiatus and the soleal arch, making it highly vulnerable in Type IV, V, and VI fractures. Ankle-brachial indices (ABI) should be measured; an ABI < 0.9 mandates a CT angiogram.
- Compartment Syndrome: High-energy proximal tibia fractures carry a high risk of acute compartment syndrome. Serial examinations are mandatory.
Imaging Protocol
- Orthogonal Radiographs: AP, lateral, and oblique views of the knee. Traction views can help delineate fracture fragments.
- Computed Tomography (CT): A CT scan with 2D sagittal/coronal reformations and 3D reconstructions is the gold standard. It is essential for mapping the fracture lines, identifying the location of depressed articular fragments, and planning surgical approaches and plate trajectories.
- Magnetic Resonance Imaging (MRI): While not routinely used acutely for bony planning, MRI is invaluable for identifying associated meniscal tears (up to 50% incidence) and cruciate/collateral ligament ruptures.
SURGICAL MANAGEMENT: PRINCIPLES AND APPROACHES
Timing of Surgery and Damage Control
For high-energy fractures (Schatzker IV-VI) with severe soft-tissue compromise, a "damage control" approach is standard. A spanning knee external fixator is applied acutely to restore length, alignment, and rotation while allowing the soft tissues to recover. Definitive open reduction and internal fixation (ORIF) is delayed for 10 to 21 days until the "wrinkle sign" appears, indicating the resolution of edema.
Patient Positioning
- The patient is placed supine on a radiolucent operating table.
- A bump is placed under the ipsilateral hip to correct natural external rotation.
- A sterile tourniquet is applied to the proximal thigh.
- The leg must be freely drapable to allow intraoperative manipulation and varus/valgus stressing.
Surgical Approaches
1. Anterolateral Approach
- Indications: Schatzker Types I, II, III, and the lateral component of Types V and VI.
- Technique: An S-shaped or straight incision is made centered over Gerdy's tubercle. The iliotibial band is incised, and the origin of the extensor digitorum longus is elevated off the proximal tibia. A submeniscal arthrotomy is performed to directly visualize the articular reduction.
2. Posteromedial Approach
- Indications: Schatzker Type IV and the medial component of Types V and VI.
- Technique: A longitudinal incision is made along the posteromedial border of the tibia. The interval is developed between the medial head of the gastrocnemius (retracted posteriorly) and the pes anserinus (retracted anteriorly). This allows direct access to the posteromedial apex of the fracture, which is critical for preventing varus collapse.
3. Dual Incisions
- Indications: Bicondylar fractures requiring bilateral buttressing.
- Technique: Combines the anterolateral and posteromedial approaches. A minimum skin bridge of 7 cm must be maintained between the incisions to prevent catastrophic skin necrosis.
STEP-BY-STEP SURGICAL TECHNIQUE
Fixation of Cleavage and Depression Fractures (Schatzker II)
- Exposure: Perform the anterolateral approach and submeniscal arthrotomy. Place a stay suture in the anterior horn of the lateral meniscus to retract it superiorly.
- Windowing: Open the lateral cleavage fracture like a book to expose the centrally depressed articular fragments.
- Elevation: Use a bone tamp from below to carefully elevate the depressed articular cartilage to match the contour of the femoral condyle.
- Bone Grafting: Pack the resulting metaphyseal void tightly with autograft (e.g., from the iliac crest), allograft, or a structural calcium phosphate cement to support the elevated cartilage.
- Rafting: Place 3.5 mm or 4.0 mm subchondral "raft" screws parallel to the joint line to support the articular surface.
- Buttress Plating: Apply a pre-contoured lateral proximal tibial locking plate. The plate acts as a buttress to prevent the lateral cleavage fragment from sliding distally.
Fixation of Bicondylar Fractures (Schatzker V and VI)
- Medial Column First: The medial column is typically the non-comminuted, primary weight-bearing axis. Reduce the posteromedial fragment anatomically and stabilize it with an under-contoured posteromedial antiglide/buttress plate.
- Lateral Column Second: Once the medial column is restored, address the lateral side. Elevate the joint surface, graft the defect, and apply a lateral locking plate.
- Diaphyseal Dissociation: For Schatzker VI fractures, the plates must span the metaphyseal-diaphyseal junction. Long locking plates are slid submuscularly down the shaft using minimally invasive percutaneous osteosynthesis (MIPO) techniques to preserve the periosteal blood supply.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of tibial plateau fracture surgery relies heavily on strict adherence to a phased rehabilitation protocol.
- Phase I (0-6 weeks): The patient is strictly non-weight-bearing (NWB) or touch-down weight-bearing (TDWB). Early passive and active-assisted range of motion (ROM) is initiated immediately, often utilizing a continuous passive motion (CPM) machine to prevent arthrofibrosis and nourish the articular cartilage.
- Phase II (6-12 weeks): Progressive partial weight-bearing is initiated based on radiographic evidence of callus formation and clinical stability. Strengthening of the quadriceps and hamstrings begins.
- Phase III (12+ weeks): Progression to full weight-bearing. Advanced proprioceptive and functional training is introduced.
COMPLICATIONS
Despite meticulous surgical technique, complications remain prevalent due to the severity of these injuries:
1. Infection and Wound Dehiscence: High-energy fractures with compromised soft tissues are at high risk. Deep infections may require serial debridements, hardware removal, and flap coverage.
2. Post-Traumatic Osteoarthritis: The risk correlates with the degree of initial articular comminution, residual step-off (>2 mm), and meniscal loss.
3. Joint Stiffness: Arthrofibrosis is common if early ROM is not instituted. Manipulation under anesthesia or arthroscopic lysis of adhesions may be required.
4. Hardware Prominence: Lateral plates can cause iliotibial band friction, while medial plates can irritate the pes anserinus, occasionally necessitating hardware removal after complete bony union.
You Might Also Like
