Surgical Management of Thumb Hypoplasia and Aplasia: Advanced Reconstructive Techniques
Key Takeaway
Congenital thumb hypoplasia and aplasia present complex reconstructive challenges. Surgical management depends on the severity of the deformity, ranging from tendon transfers like the Blair and Omer flexor pollicis longus rerouting for abducted thumbs, to index finger pollicization for complete aplasia. This guide details the biomechanical principles, step-by-step surgical techniques, and postoperative protocols required to restore prehensile function, pinch strength, and hand aesthetics in pediatric patients.
INTRODUCTION TO CONGENITAL THUMB ANOMALIES
Congenital hypoplasia and aplasia of the thumb represent a spectrum of longitudinal radial ray deficiencies that profoundly impact global hand function. The thumb contributes approximately 40% to 50% of total hand function, serving as the critical opposing post for power grip, precision pinch, and fine motor manipulation.
Surgical intervention is dictated by the severity of the hypoplasia, classically categorized by the Blauth classification. While mild hypoplasia (Grade I) may require no intervention, moderate hypoplasia (Grades II and III) often presents with thenar muscle absence, metacarpophalangeal (MCP) joint instability, and aberrant extrinsic tendon anatomy—specifically the flexor pollicis longus (FPL). Severe manifestations, such as the floating thumb (Grade IV) or complete aplasia (Grade V), necessitate complex reconstructive salvage procedures, including index finger recession or formal pollicization.
This masterclass details the operative management of these complex deformities, focusing on the Blair and Omer rerouting technique for the aberrant FPL, the management of the floating thumb, the Flatt recession of the index finger, and the principles of index pollicization.
REROUTING OF THE FLEXOR POLLICIS LONGUS (BLAIR AND OMER)
Pathoanatomy and Biomechanical Rationale
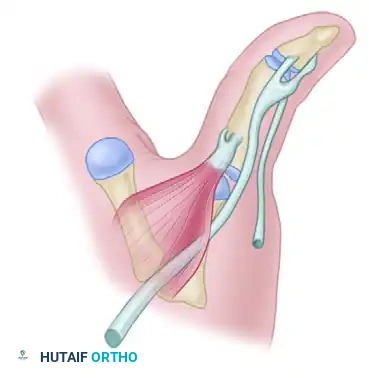
In patients with Grade II or Grade III thumb hypoplasia, a classic deformity known as pollex abductus may be present. This is characterized by a fixed abduction and extension posture of the thumb. The primary anatomical culprit is an anomalous tendinous connection between the flexor pollicis longus (FPL) and the extensor pollicis longus (EPL).
Instead of inserting solely into the base of the distal phalanx to provide robust interphalangeal (IP) flexion, an aberrant slip of the FPL courses over the radial border of the thumb to merge with the EPL. Biomechanically, when the FPL contracts, it paradoxically acts as an abductor and extensor of the thumb, exacerbating the deformity and negating effective pinch.
The Blair and Omer technique is designed to correct this vector mismatch. By releasing the anomalous slip, rerouting the FPL ulnarward, and utilizing the abductor pollicis brevis (APB) as a stabilizing sling, the surgeon restores the physiological flexion vector and centralizes the tendon over the MCP joint.
💡 Clinical Pearl: The Anomalous Slip
Always suspect an anomalous FPL-to-EPL slip in a hypoplastic thumb that rests in fixed abduction and lacks active IP joint flexion. Failure to identify and sharply release this slip will result in persistent postoperative deformity and functional failure of any concurrent opposition transfers.
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia is required for pediatric patients.
- Positioning: Supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is applied. Exsanguination is performed via elevation or an Esmarch bandage prior to inflation.
- Magnification: Surgical loupes (2.5x to 3.5x) are mandatory for meticulous identification of digital nerves and aberrant tendinous slips.
Surgical Technique: Step-by-Step
1. Surgical Approach and Exposure
Make a zigzag palmar incision along the volar aspect of the thumb. This incision should extend from the distal phalanx, crossing the IP and MCP joints obliquely to prevent flexion contractures, and terminate in the proximal thenar crease. Carefully elevate the skin flaps.
2. Neurovascular Protection
Identify the radial and ulnar digital nerves of the thumb early in the dissection. In hypoplastic digits, neurovascular bundles are frequently displaced or anomalous. Retract and protect them with vessel loops throughout the procedure.
3. Identification and Release of the Aberrant FPL Slip
Explore the flexor sheath and identify the FPL tendon. Trace it distally. You will typically encounter the abnormal tendinous slip passing over the radial border of the thumb, bridging the space between the MCP and IP joints, and inserting into the EPL.
* Sharply release this abnormal insertion from the EPL.
* Preserve the length of this anomalous slip, as it may be utilized later for ligamentous reconstruction.
4. Release of the Abductor Pollicis Brevis (APB)
Identify the insertion of the APB on the radial aspect of the proximal phalanx and the extensor hood. Release the APB insertion sharply to mobilize the muscle belly and prepare the bed for FPL rerouting.
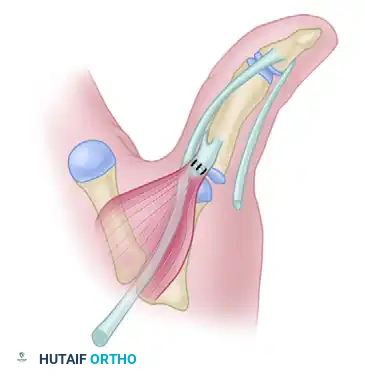
5. Rerouting the FPL Tendon
Transfer the mobilized FPL tendon ulnarward, passing it under the released APB tendon. This maneuver shifts the flexion vector from a radial/abducting force to a centralized, true volar flexion force.
6. Addressing Joint Contractures and Instability
Assess the MCP joint. If the abduction deformity of the thumb MCP joint cannot be passively corrected after the tendon rerouting, perform a fractional or complete release of the tight radial collateral ligament (RCL).
Conversely, assess the ulnar collateral ligament (UCL). Hypoplastic thumbs frequently exhibit profound UCL laxity. If UCL laxity is present, take the previously preserved abnormal tendon slip of the FPL, route it across the ulnar aspect of the MCP joint, and suture it to the periosteum or base of the proximal phalanx to reinforce the deficient UCL.
7. Reattachment of the APB (The Sling Construction)
Suture the APB tendon back into its normal anatomical insertion on the radial base of the proximal phalanx. By securing the APB over the rerouted FPL, you construct a dynamic soft-tissue sling. This sling centralizes the FPL, prevents radial subluxation during active flexion, and stabilizes the MCP joint.

8. Closure
Deflate the tourniquet, achieve meticulous hemostasis with bipolar electrocautery, and suture the skin with simple interrupted absorbable sutures (e.g., 5-0 or 6-0 chromic gut or fast-absorbing plain gut in pediatric patients).
Postoperative Care and Rehabilitation
- Immobilization: Apply a modified thumb spica cast. The cast must extend beyond the IP joint dorsally to prevent hyperextension, but it should stop proximal to the MCP joint on the volar side.
- Biomechanical Rationale of the Cast: This specific cast design prevents hyperextension and abduction of the thumb (protecting the RCL release and UCL reconstruction) while simultaneously allowing active MCP flexion and FPL tendon excursion to prevent adhesions.
- Duration: The cast is maintained for exactly 6 weeks.
- Therapy: Upon cast removal at 6 weeks, unlimited motion of the hand is permitted. Occupational therapy is initiated to encourage integration of the thumb into prehensile activities and to re-educate the rerouted flexion vector.
THE FLOATING THUMB (POUCE FLOTTANT) DEFORMITY
The "floating thumb" (Blauth Grade IV) represents a severe manifestation of radial longitudinal deficiency. Anatomically, the thumb is completely devoid of proximal skeletal support (absent metacarpal and absent or rudimentary trapezium/trapezoid). The digit is attached to the radial border of the hand merely by a narrow, non-functional skin bridge containing a tenuous neurovascular supply. Extrinsic and intrinsic musculature is entirely absent.

🚨 Surgical Warning: Reconstruction vs. Ablation
Attempting to reconstruct a Grade IV floating thumb via bone grafting and complex tendon transfers is historically fraught with failure. The resulting digit is inevitably stiff, insensate, and bypassed by the child during functional tasks. The gold standard of care for a floating thumb is amputation of the rudimentary appendage followed by index finger pollicization.
FLATT RECESSION OF THE INDEX FINGER
While pollicization is the standard of care for thumb aplasia in infants, the clinical scenario changes when evaluating an older child or adolescent who has already established a strong, compensatory lateral pinch between the index and long fingers.
In these older patients, cortical plasticity has diminished. If a standard pollicization is performed, the patient may ignore the newly pollicized digit and continue attempting to pinch between the long and ring fingers—a highly inefficient pattern. For these specific cases, the Flatt Recession of the index finger is the preferred alternative.
Biomechanical Rationale
The Flatt procedure does not attempt to create a fully opposable thumb. Instead, it shortens (recesses) the index finger, rotates it, and abducts it to widen the first web space. This makes the index finger resemble a thumb aesthetically and optimizes it as a robust, static post against which the long finger can achieve a powerful lateral pinch.
Surgical Technique: Step-by-Step
1. Incisions and Soft Tissue Release
Two separate incisions are required:
* Distal Incision: Placed in the web space between the index and long fingers. Through this incision, identify and sharply divide the intermetacarpal ligament to allow independent mobilization of the index ray.
* Proximal Incision: Placed dorsally over the base of the index metacarpal to expose the bone for osteotomy.
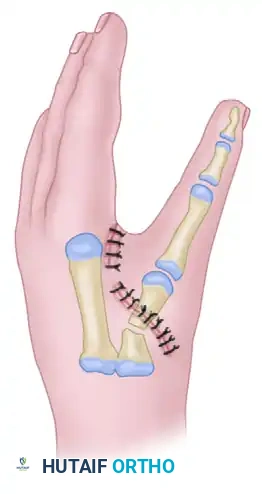
2. Metacarpal Osteotomy
Perform a transverse or slightly oblique osteotomy at the proximal metaphysis of the index metacarpal. Resect a calculated segment of the metacarpal shaft to achieve the desired recession (shortening), ensuring the tip of the new "thumb" aligns appropriately with the proximal interphalangeal (PIP) joint of the long finger.
3. Rotation and Abduction
Mobilize the distal segment of the index ray. To optimize the pinch vector:
* Rotate the distal portion 110 degrees along its longitudinal axis (pronating it to face the long finger).
* Abduct the ray 20 degrees radialward to open the neo-web space.

4. Skeletal Fixation and Closure
Secure the osteotomy site rigidly. While the historical text implies stabilization, modern techniques dictate the use of crossed K-wires or a small fragment plate to maintain the 110-degree rotation and 20-degree abduction. Close the skin incisions meticulously, often requiring local flap rearrangement (e.g., Z-plasties) in the web space to prevent contracture.
ABSENT THUMB (APLASIA) AND POLLICIZATION
Syndromic Associations and Systemic Evaluation
Absence of the thumb (Blauth Grade V) is the most severe manifestation of the hypoplastic thumb spectrum. It is rarely an isolated anomaly and mandates a rigorous systemic workup. It is frequently associated with radial ray deficiencies (radial clubhand) and several life-threatening syndromic conditions:
* VACTERL Association: Vertebral, Anal, Cardiac, Tracheoesophageal, Renal, and Limb anomalies.
* Holt-Oram Syndrome: Autosomal dominant (TBX5 mutation) associated with atrial or ventricular septal defects.
* TAR Syndrome: Thrombocytopenia-Absent Radius syndrome.
* Fanconi Anemia: A critical diagnosis to rule out due to the risk of fatal bone marrow failure.
* Trisomy 18 & Ring D Chromosome Abnormalities.
💡 Clinical Pearl: The TAR Syndrome Exception
In classic radial clubhand, the radius is absent, and the thumb is concomitantly absent or severely hypoplastic. However, TAR syndrome is the notable exception. In TAR syndrome, the radius is absent, but the thumb is characteristically present.
Functional Implications
Bilateral absence of the thumb creates extreme functional impairment. Infants naturally compensate by developing a strong lateral pinch between the index and long fingers. Rotational deformity of the fingers may allow limited, rudimentary opposition, but fine motor manipulation of small objects remains severely compromised.
Principles of Pollicization
Function and appearance are dramatically improved with a satisfactory pollicization of the index finger. Pollicization involves the neurovascular island transfer of the index finger to the thumb position, shortening of the metacarpal (which becomes the new trapezium), and complex tendon transfers to recreate thenar mechanics.
Timing of Surgery:
The timing of pollicization is dictated by the child’s natural neurocognitive development of prehensile activities. Because infants begin to develop pinch and grasp patterns around 3 months of age, the optimal window for pollicization is between 6 and 12 months of age.
* Operating within this window allows sufficient physical growth of the hand to make the microvascular and tendinous dissection safer.
* More importantly, it capitalizes on maximal cortical plasticity, allowing the brain to seamlessly integrate the transferred index finger as a thumb.
* In bilateral cases, pollicization of one side should be performed early (within the 6-12 month window). The parents and surgical team can then evaluate functional outcomes before deciding on the timing for the contralateral side.
Functional Outcomes:
Surgeons must set realistic expectations with parents regarding the outcomes of pollicization. Staines et al. extensively reviewed functional outcomes in children undergoing pollicization for thumb aplasia. Key findings include:
* Strength: Postoperative grip and pinch strengths typically reach only about 50% (half) of the strength of an uninvolved, normal hand.
* Dexterity: While gross grasp is vastly improved, activities requiring simultaneous pinch and complex manipulation of small objects (e.g., buttoning clothes, manipulating coins) remain the most difficult tasks for these patients.
Despite these limitations, pollicization remains one of the most elegant and functionally transformative procedures in pediatric orthopedic hand surgery, converting a severely impaired, four-fingered hand into a functional, prehensile unit.
You Might Also Like