Acute Septic Arthritis of the Hip: Comprehensive Surgical Management and Approaches
Key Takeaway
Acute septic arthritis of the hip is a surgical emergency, particularly in pediatric patients where the unique vascular anatomy places the femoral head at high risk for osteonecrosis and pathological dislocation. Prompt diagnosis via image-guided aspiration and emergent surgical drainage—utilizing anterior, posterior, lateral, or medial approaches—is paramount. This guide details the operative techniques, biomechanical considerations, and postoperative protocols essential for preserving joint function and preventing devastating sequelae such as osteomyelitis or joint destruction.
Pathophysiology and Biomechanical Considerations
Acute septic arthritis of the hip represents a profound orthopedic emergency that demands immediate diagnostic and therapeutic intervention. The disease process is notably more severe in pediatric populations compared to adults, carrying a significantly higher risk of devastating, lifelong complications.
In the pediatric hip, the metaphysis is intra-capsular. Consequently, hematogenous osteomyelitis beginning in the proximal femoral metaphysis or epiphysis can easily rupture through the thin pediatric cortex directly into the joint space, rapidly converting a localized bone infection into a fulminant septic arthritis.
The most critical biomechanical and anatomical vulnerability in the pediatric septic hip is the precarious blood supply to the femoral head. The retinacular vessels (branches of the medial circumflex femoral artery) traverse the surface of the femoral neck within the joint capsule. As purulent exudate accumulates, intra-articular pressure rises exponentially. This capsular distension creates a tamponade effect, occluding the low-pressure venous drainage and subsequently the arterial supply, placing the femoral head at imminent risk for ischemic osteonecrosis (avascular necrosis). Furthermore, the proteolytic enzymes released by bacteria and host neutrophils rapidly degrade articular cartilage.
Clinical Pearl: If a septic hip goes undiagnosed in an infant, the combination of massive capsular distension, joint effusion, and reflexive muscle spasm can lever the femoral head out of the acetabulum, resulting in a pathological dislocation. Epiphyseal separation is also a documented, albeit rare, complication.
Bilateral septic arthritis is observed more frequently in the hip than in other joints and should raise clinical suspicion for an associated spinal or pelvic infection.
Diagnostic Joint Aspiration
Aspiration of the hip joint is the definitive diagnostic maneuver and must be performed prior to the initiation of empiric antibiotic therapy. A lateral, anterior, or medial approach can be utilized. The use of image intensification (fluoroscopy or ultrasound) is strongly recommended to ensure precise intra-articular needle placement and avoid iatrogenic neurovascular injury.
If fluid cannot be aspirated (a "dry tap"), an arthrogram should be performed by injecting a small amount of radiopaque contrast to verify the needle’s intra-articular position. Occasionally, highly viscous purulence cannot be aspirated through a needle, yet its presence is later confirmed during open arthrotomy. If clinical suspicion remains high and systemic symptoms are uncontrolled, surgical exploration is mandated despite a negative aspiration.
Lateral Aspiration Technique
The lateral approach is often preferred due to its safety profile, avoiding the anterior neurovascular bundle.
* Position the patient supine.
* Insert a large-bore spinal needle at a 45-degree angle to the surface of the thigh, entering just inferior and anterior to the greater trochanter.
* Advance the needle medially and proximally, keeping it in close proximity to the bone.
* Depending on the patient's size, the needle will enter the joint capsule at a depth of 5 to 10 cm.
Anterior Aspiration Technique
- Identify the anterior superior iliac spine (ASIS) and palpate the femoral artery in line with the inguinal ligament.
- Insert the needle 2.5 cm lateral and 2.5 cm distal to the palpated femoral pulse to avoid the neurovascular bundle.
- Direct the needle at a 45-degree angle to the skin surface.
- Advance the needle 5 to 7.5 cm medially and proximally until the bony resistance of the femoral neck is felt, then aspirate.
Medial Aspiration Technique
- Position the patient with the affected leg flexed and abducted. This position relaxes the capsule and is typically the most comfortable resting posture for a patient with a septic hip.
- Place the needle inferior to the adductor longus tendon.
- Utilizing image intensification, advance the needle in a plane strictly posterior/inferior to the palpated femoral artery until the femoral head or neck is reached.
- Aspirate the joint cavity.
Surgical Drainage: Operative Approaches
Emergent open arthrotomy and copious irrigation remain the gold standard for acute septic arthritis of the hip. Drainage may be accomplished through an anterior, posterior, lateral, or medial approach.
The anterior approach is overwhelmingly preferred in pediatric patients for three critical reasons:
1. It avoids the posterior retinacular vessels, thereby protecting the major blood supply to the femoral head.
2. It preserves the posterior capsule, significantly reducing the risk of postoperative posterior dislocation.
3. The anatomical landmarks are superficial and easily identifiable in small children.
Conversely, in adult patients, the posterior approach is often favored as it provides dependent drainage when the patient is supine and utilizes an anatomical interval highly familiar to most orthopedic surgeons.
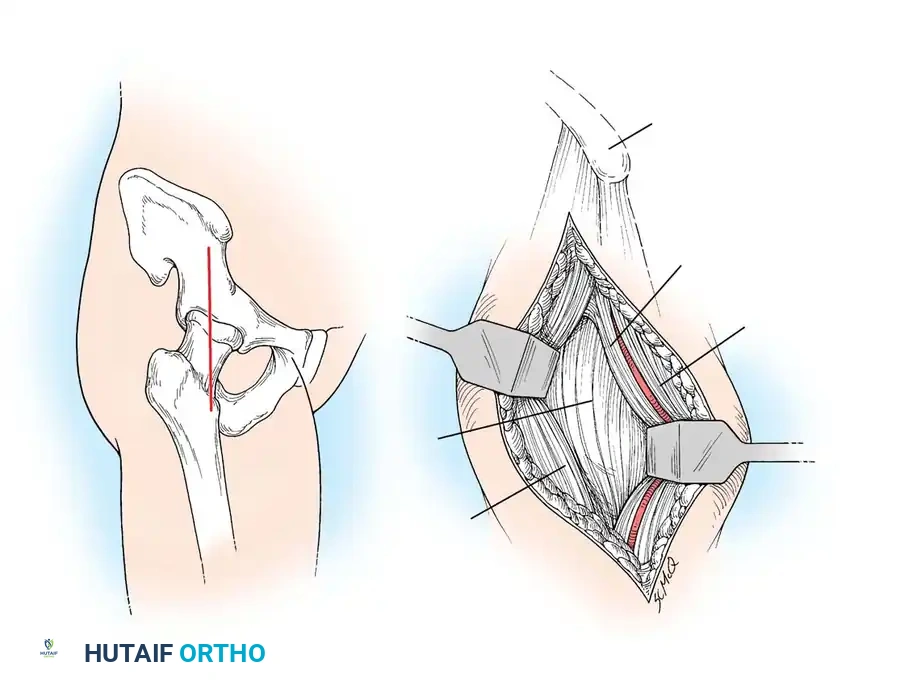
Anterior Drainage Technique
This approach utilizes the internervous plane between the sartorius (femoral nerve) and the tensor fasciae latae (superior gluteal nerve).
- Incision: Make a vertical longitudinal incision beginning approximately 1 cm inferior to the anterior superior iliac spine (ASIS).
- Superficial Dissection: Identify the sartorius muscle medially and the tensor fasciae latae (TFL) laterally. Use blunt dissection to develop this internervous plane.
- Deep Dissection: Deepen the exposure to identify the rectus femoris muscle. Retract the rectus femoris medially (or detach its direct head from the anterior inferior iliac spine if necessary for exposure). Retracting the vastus lateralis laterally exposes the anterior hip joint capsule.
- Capsulotomy: Incise the capsule longitudinally or in a T-shape. Immediately evacuate the purulent material and obtain cultures.
- Irrigation: Irrigate the joint profusely with several liters of sterile saline to mechanically debride the joint and remove all fibrinous exudate.
- Closure: Leave the joint capsule open to prevent re-accumulation of pressure. Close the subcutaneous tissue and skin loosely over a surgical drain (e.g., a Jackson-Pratt drain) to allow for continuous egress of fluid.
- Extended Exposure: If wider exposure is required, the skin incision can be extended proximally along the iliac crest, subperiosteally detaching the origins of the TFL and anterior gluteal muscles from the outer table of the ilium.
- Surgical Warning: Meticulously protect the lateral femoral cutaneous nerve proximally (often crossing the sartorius) and the ascending branches of the lateral femoral circumflex artery distally.
Posterior Drainage Technique (Ober)
The posterior approach provides excellent dependent drainage. It utilizes a muscle-splitting approach through the gluteus maximus.
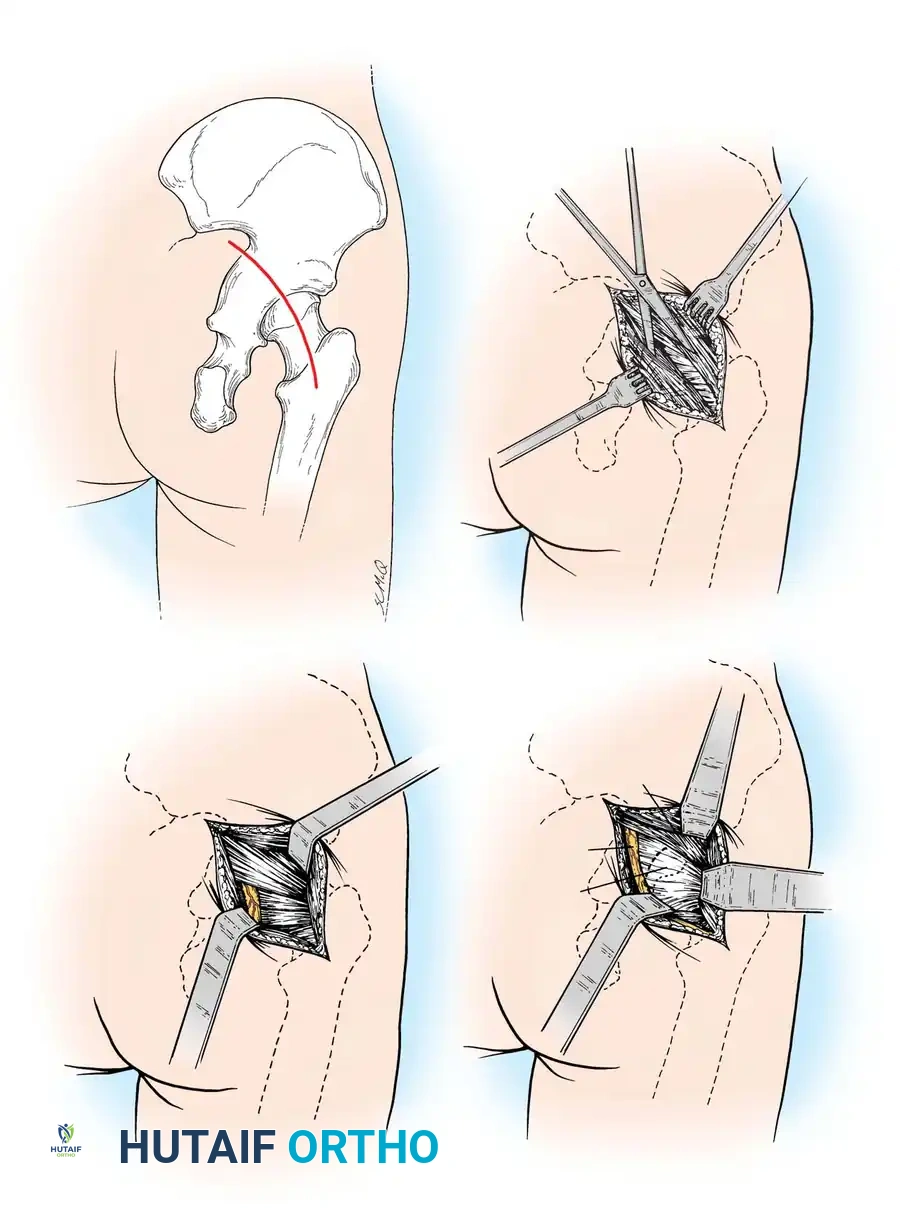
- Positioning: Lateral decubitus position.
- Incision: Make an oblique incision in line with the femoral neck, extending from the posterior tip of the greater trochanter toward the posterior superior iliac spine (PSIS).
- Superficial Dissection: Split the gluteus maximus muscle bluntly in line with its muscle fibers. Ligate any crossing branches of the inferior gluteal vessels as they are encountered to maintain hemostasis.
- Deep Dissection: Place a Charnley retractor. Identify and meticulously protect the sciatic nerve, which lies in the medial angle of the surgical field, superficial to the short external rotators.
- Capsular Exposure: Identify the short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus). Tag and divide them near their insertion on the greater trochanter, reflecting them medially to protect the sciatic nerve.
- Capsulotomy: Incise the posterior capsule. Crucial Step: The capsulotomy should be made medially, near its pelvic attachment at the acetabular rim, to avoid injuring the retinacular blood supply traversing the femoral neck.
- Irrigation and Closure: Evacuate pus, irrigate profusely with saline, leave the capsule open, and close the skin loosely over deep drains.
Lateral Drainage Technique
- Incision: Make a longitudinal incision 7.5 to 12.5 cm long, centered over and parallel to the anterior border of the greater trochanter.
- Dissection: Incise the fascia lata to expose the vastus lateralis and the anterior border of the gluteus medius.
- Deep Exposure: Detach the anterior portion of the vastus lateralis origin from the vastus ridge. Retract the abductor musculature (gluteus medius/minimus) proximally and anteriorly to gain access to the anterior capsule.
- Drainage: Incise the capsule, evacuate the purulence, irrigate thoroughly, and close loosely over drains.
Medial Drainage Technique (Ludloff)
The medial approach is particularly useful when a concurrent pelvic or psoas abscess is suspected, as it allows access to the communication behind the iliopsoas muscle.
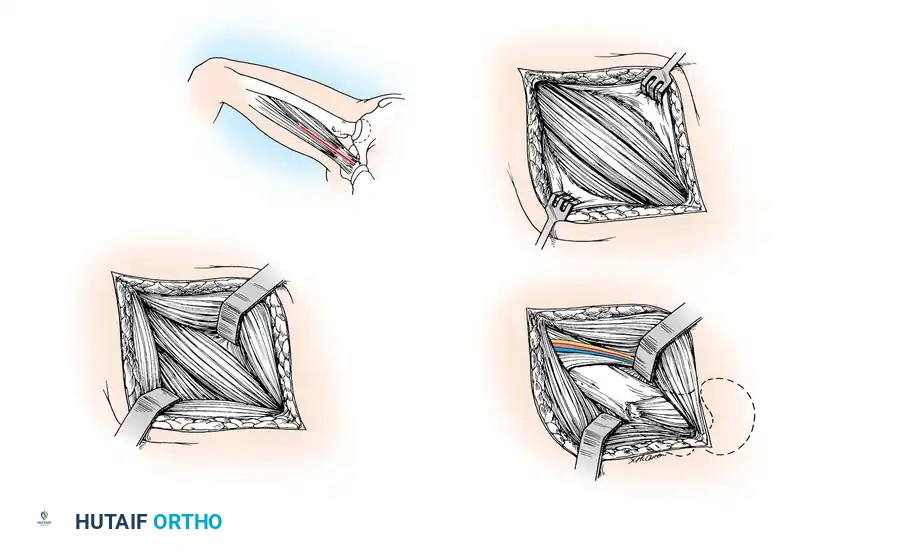
- Positioning: Supine, with the affected hip flexed, abducted, and externally rotated (the "frog-leg" position).
- Incision: Make a longitudinal incision 7.5 to 10 cm long on the medial aspect of the proximal thigh, centered over the adductor longus.
- Superficial Dissection: Expose the proximal one-fourth of the gracilis and adductor longus muscles. Develop the longitudinal cleavage plane between the adductor longus (anteriorly) and the gracilis (posteriorly).
- Deep Dissection: Bluntly dissect posterior to the adductor longus and pectineus muscles. This trajectory leads directly into the abscess cavity, which frequently communicates with the hip joint behind the iliopsoas tendon. The lesser trochanter serves as the deep anatomical landmark.
- Drainage: Evacuate the pus, irrigate the wound with saline, and close the skin loosely over drains.
Note on Arthroscopic Drainage: While arthroscopic drainage for acute septic arthritis of the hip has been reported in recent literature with some small studies showing good to excellent results, open arthrotomy remains the gold standard. Arthroscopy requires specialized pediatric equipment, carries a steep learning curve, and may not allow for the complete removal of thick, loculated fibrinous exudate compared to open techniques.
Postoperative Management Protocols
Postoperative immobilization and joint offloading are critical to prevent pathological dislocation and allow the inflamed capsule to heal.
- Infants and Toddlers: Postoperatively, the child is best managed in a double hip spica cast. The affected extremity must be positioned in moderate abduction and slight flexion to center the femoral head within the acetabulum and maximize joint volume, thereby reducing residual pressure. Adequate windows must be cut into the cast over the surgical site to allow for daily wound inspection, drain management, and dressing changes.
- Older Children and Adults: These patients are typically confined to bed rest with Buck's skin traction (or skeletal traction if instability is noted) applied to the affected limb. Traction relieves muscle spasm, distracts the joint surfaces (preventing cartilage necrosis from mechanical pressure), and maintains alignment.
- Rehabilitation: Traction is maintained until the wound has healed, systemic inflammatory markers (CRP, ESR) have normalized, and the patient demonstrates active control of the leg (e.g., the ability to perform a straight leg raise against gravity). Following this, protective weight-bearing using crutches is permitted, and active range-of-motion exercises are aggressively initiated to prevent intra-articular adhesions and fibrous ankylosis.
Complications of Acute Septic Arthritis of the Hip
Pathological Dislocation
Pathological dislocation is predominantly a pediatric complication, rarely seen in adults. It occurs due to the combination of massive capsular distension from purulence, ligamentous laxity induced by hyperemia, and severe reflex muscle spasms.
If the dislocation is recognized early—before severe soft-tissue contractures develop—reduction is usually accomplished easily at the time of surgical drainage. The hip is then stabilized in a spica cast, and satisfactory long-term function may result.
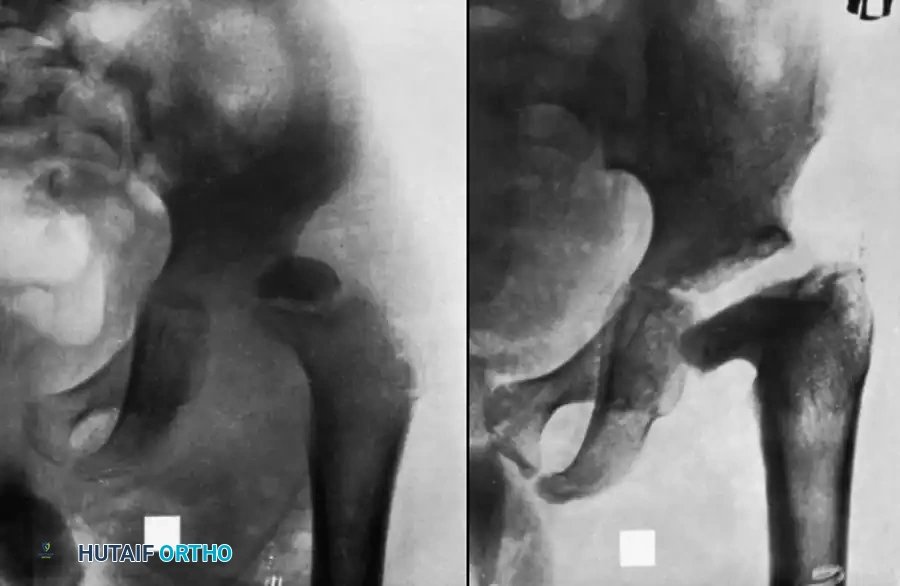
However, if the diagnosis is delayed and the femoral head has been damaged by infection or ischemia, immediate manipulation is contraindicated. Attempting closed reduction on a compromised, osteopenic proximal femur carries a high risk of iatrogenic femoral neck fracture. Instead, skeletal traction should be applied via a distal femoral pin. Traction is gradually increased until radiographic imaging confirms the femoral head has been pulled down to the level of the acetabulum. Only then is the dislocation reduced via gentle abduction and internal rotation. Post-reduction, the hip is immobilized in a spica cast until stability is achieved or until fibrous/bony ankylosis develops.

Clinical Pearl (Lloyd-Roberts): In infants, severe osteopenic changes in the femoral head associated with acute septic arthritis can mimic complete joint destruction on plain radiographs. What appears to be a dislocation with total destruction of the proximal femur may actually be a viable femoral head that has simply demineralized. These hips should be explored or gently manipulated, as the head may survive and remodel once reduced and the infection cleared.
Osteomyelitis
When infection is confined strictly to the joint space, prompt arthrotomy and targeted intravenous antibiotic therapy usually prevent secondary osteomyelitis of the proximal femur.
However, if osteomyelitis does occur and results in sequestration of the femoral head in children under 12 years of age, the entire cartilaginous head may be totally reabsorbed. Alternatively, if the retinacular circulation is restored, the head may act as a scaffold and be replaced by new bone via creeping substitution.
In older children and adults, a devascularized femoral head typically remains as an infected, necrotic sequestrum that acts as a nidus for chronic infection. This requires formal surgical excision. While any approach can be used, the anterior approach provides superior exposure for complete head and neck resection.
In children, osteomyelitis of the ilium may also complicate septic arthritis (either as the primary source or a secondary extension). Both the joint and the ilium require meticulous drainage. In adults, impaired circulation may lead to pathological fractures of the femoral neck alongside sequestration.
Pelvic Abscess
A pelvic abscess complicating a septic hip arises from suppurative lymphadenitis of the iliac nodes or direct extension from the joint into the iliopsoas bursa (which communicates with the hip joint in up to 15% of patients).
These abscesses are retroperitoneal. They tend to gravitate along the iliopsoas muscle beneath the inguinal ligament, eventually pointing in the medial thigh. In cases of massive accumulation, the pus may track proximally along the psoas fascia and point proximal to the posterior iliac crest. MRI is the imaging modality of choice to determine the true extent of psoas and retroperitoneal involvement. While open drainage was historically required, many of these can now be successfully managed with CT-guided percutaneous aspiration and drain placement.
If open drainage is required (as advised by Freiberg and Perlman):
* Medial Pointing: Use the Ludloff incision. Dissect bluntly between the adductor longus and brevis to find the abscess anterior or posterior to the pectineus.
* Anterior Pointing: Incise directly over the mass, exercising extreme caution to protect the femoral neurovascular bundle. Drainage above the inguinal ligament is discouraged due to the risk of incomplete evacuation and the potential for creating a fecal fistula.
* Posterior Pointing: Make an incision parallel and just proximal to the posterior iliac crest. Detach the abdominal musculature from the crest and open the abscess via blunt dissection.
Persistent Infection and Salvage Procedures
Persistent chronic infection around the hip is a catastrophic complication. It is characterized by extensive soft-tissue scarring, chronic draining sinus tracts, and recurrent acute exacerbations when sinuses become blocked.
Unless aggressive, radical surgical debridement is performed, chronic sepsis will lead to systemic amyloidosis or sepsis. Girdlestone described a radical salvage operation for chronic pyogenic infection of the hip. The Girdlestone resection arthroplasty involves complete saucerization of the infected area. The femoral head, neck, and infected acetabular margins are radically resected. A massive block of infected muscle and scar tissue is excised to ensure wide-open, dependent drainage.
Modern modifications of the Girdlestone procedure often involve a three-stage approach to control infection:
1. Radical Resection: A classic Girdlestone procedure to remove all osteomyelitic bone.
2. Muscle Flap Transposition: Transposition of a vascularized muscle pedicle (e.g., vastus lateralis or rectus abdominis) into the massive dead space left by the resection of the proximal femur and acetabulum. This brings robust blood supply to the infected bed.
3. External Fixation: Application of a spanning external fixator to prevent unrestrained, painful motion of the femoral shaft, maintain leg length as much as possible, and protect the transposed muscle flap while the infection is eradicated.
While this salvage procedure eradicates the infection, it results in a pseudarthrosis, profound leg-length discrepancy, and a significantly altered gait, underscoring the absolute necessity of early, aggressive management of the acute septic hip.
You Might Also Like

