Brachioradialis to ECRB Transfer & Key Pinch Restoration
Key Takeaway
The transfer of the brachioradialis to the extensor carpi radialis brevis (ECRB) is a foundational reconstructive procedure for restoring wrist extension in tetraplegic patients. Augmenting this with key pinch restoration techniques, such as the Moberg, Brand, or Bruner tenodeses, significantly enhances hand function. This guide details the biomechanical principles, step-by-step surgical approaches, and postoperative rehabilitation protocols essential for optimizing outcomes in upper limb paralysis reconstruction.
INTRODUCTION TO UPPER LIMB RECONSTRUCTION IN TETRAPLEGIA
The restoration of upper extremity function in patients with cervical spinal cord injuries (tetraplegia) is one of the most profoundly impactful interventions in reconstructive orthopedic surgery. For patients with mid-cervical lesions, the ability to extend the wrist and perform a basic pinch can mean the difference between total dependence and functional independence in activities of daily living (ADLs).
The cornerstone of this reconstructive hierarchy is the restoration of active wrist extension, typically achieved via the transfer of the brachioradialis (BR) to the extensor carpi radialis brevis (ECRB). Once wrist extension is secured, the biomechanical foundation is laid for restoring thumb flexion and key pinch through various tenodesis techniques or active tendon transfers.
This comprehensive guide details the biomechanical rationale, precise surgical techniques, and postoperative protocols for the BR to ECRB transfer, alongside advanced reconstructive strategies for key pinch restoration, including the Moberg, Brand, Bruner, and House procedures.
PREOPERATIVE EVALUATION AND INDICATIONS
Patient selection and meticulous preoperative assessment are paramount. The International Classification for Surgery of the Hand in Tetraplegia (ICSHT) categorizes patients based on the number of expendable, functioning muscles below the elbow graded at Medical Research Council (MRC) grade 4 or higher.
Prerequisites for Tendon Transfer
To be considered a candidate for a BR to ECRB transfer and subsequent key pinch restoration, the patient must meet several strict criteria:
* Motor Power: The donor muscle (brachioradialis) must be at least MRC Grade 4.
* Joint Mobility: The wrist and thumb joints must have full, supple passive range of motion. Any contractures must be addressed preoperatively via therapy or surgical release.
* Sensibility: Adequate sensibility is critical. If two-point discrimination is less than 12 to 15 mm, bilateral hand reconstruction can be considered.
Surgical Warning: If the patient lacks sufficient sensibility and must rely entirely on ocular input (visual feedback) to manipulate objects, reconstructive surgery should be limited to one hand only. Bilateral reconstruction in the absence of proprioceptive and tactile feedback often leads to functional confusion and poor outcomes.
BIOMECHANICS OF THE BRACHIORADIALIS TO ECRB TRANSFER
The selection of the ECRB over the Extensor Carpi Radialis Longus (ECRL) as the recipient tendon is a critical biomechanical decision. The ECRB inserts centrally at the base of the third metacarpal, providing pure, balanced wrist extension. Conversely, the ECRL inserts at the base of the second metacarpal; utilizing it would result in unwanted radial deviation during extension.
The brachioradialis is a powerful muscle with a large cross-sectional area, making it an excellent motor for wrist extension. However, its natural excursion is relatively short (approximately 30 mm). To match the excursion requirements of the wrist extensors, the BR must be extensively mobilized proximally. Because its neurovascular pedicle (from the radial nerve) enters the muscle belly proximally near the elbow, aggressive proximal mobilization of the fascial attachments is both safe and biomechanically necessary to achieve the required 40 to 50 mm of excursion.
SURGICAL TECHNIQUE: BRACHIORADIALIS TO ECRB TRANSFER
Positioning and Preparation
- The patient is placed supine with the operative arm extended on a radiolucent hand table.
- A well-padded pneumatic tourniquet is applied high on the brachium.
- The arm is prepped and draped in a standard sterile fashion.
Incision and Exposure
- Make a longitudinal incision 8 to 10 cm long dorsally along the radial aspect of the mid-to-distal forearm.
- Deepen the incision through the subcutaneous tissue, maintaining meticulous hemostasis.
Nerve Protection and Muscle Mobilization
- Carefully identify the dorsal sensory branch of the radial nerve (Wartenberg's nerve) as it emerges from beneath the brachioradialis tendon in the distal third of the forearm.
- Protect this nerve meticulously with vessel loops during the mobilization of the brachioradialis.
- Identify the musculotendinous junction of the BR. Release its distal fascial attachments and mobilize the muscle belly proximally.
- Key Step: Proximal mobilization of the brachioradialis is mandatory to enhance its excursion. This is safe because the radial nerve motor branches enter the muscle in the proximal third of the forearm. Release the investing fascia until the muscle yields an excursion of at least 4 cm when pulled.
Tendon Weaving and Tensioning
- Identify the extensor carpi radialis brevis (ECRB) tendon. Trace it distally to confirm its insertion into the base of the third metacarpal.
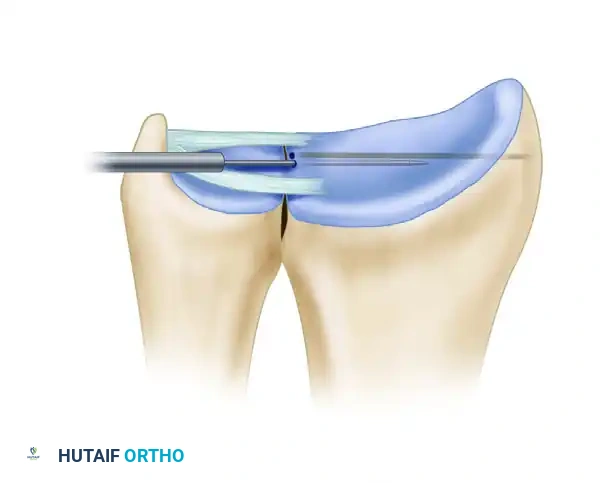
- Transect the BR tendon distally and weave it through the ECRB tendon using a standard Pulvertaft weave technique (passing the donor tendon through the recipient tendon several times at 90-degree angles).
- Tensioning: Place tension on the transferred unit. Temporarily suture the weave and assess the tenodesis effect. The wrist should rest in approximately 30 degrees of extension, and full passive wrist flexion should be achievable without undue tension or laxity of the transferred unit.
Restoration of wrist extension and key pinch when the brachioradialis is the only remaining functioning muscle unit, demonstrating the transfer into the ECRB.
RESTORATION OF KEY PINCH
Once wrist extension is secured, the next functional priority is restoring thumb pinch. Key pinch (lateral pinch), where the thumb pulp presses against the lateral aspect of the index finger middle phalanx, is biomechanically more desirable and easier to achieve than a chuck-jaw pinch (three-fingered palmar pinch).
Key pinch should be restored in all tetraplegic patients who possess grade 4 or better wrist extensor motor power. It is estimated that at least 75% of all tetraplegic patients may be candidates for a key pinch procedure.
If no expendable motor units are available for an active tendon transfer to the flexor pollicis longus (FPL), several well-designed tenodesis procedures can harness active wrist extension to drive passive thumb flexion.
The Moberg Key Grip Procedure
The Moberg key grip procedure is the historical precursor and the simplest of all thumb flexion tenodesis techniques.
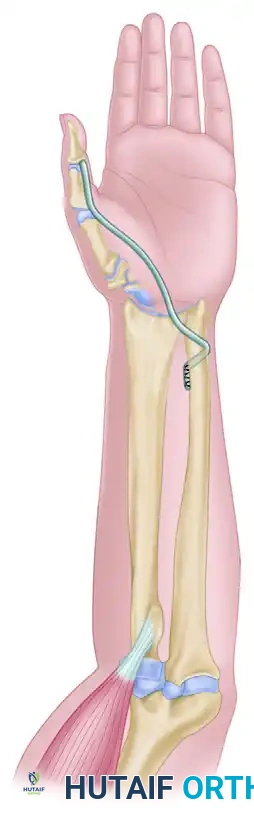
* Mechanism: The FPL tendon is tenodesed (anchored) to the distal radius.
* Action: When the patient actively extends the wrist (using the newly transferred BR to ECRB), the tenodesed FPL tendon tightens, pulling the volar pulp of the thumb strongly against the radial side of the index finger.
* Modifications: To increase the flexion torque at the metacarpophalangeal (MCP) joint, Moberg advocated for the release of the A1 pulley, allowing the FPL tendon to sublux volarward. This procedure often requires concurrent stabilization of the thumb interphalangeal (IP) and MCP joints (via arthrodesis or capsulodesis) to prevent collapse under load.
The Brand Modification
Paul Brand modified the Moberg procedure to improve the line of pull and prevent the bowstringing associated with A1 pulley release.
* Technique: The A1 pulley of the thumb MCP joint is left intact. The FPL tendon is divided proximally, routed across the palm beneath the flexor tendons, passed through the Guyon canal, and finally tenodesed to the distal radius.
* Biomechanical Advantage: This routing creates a superior vector for adduction and flexion, significantly improving the strength and aesthetics of the key pinch while preventing volar bowstringing of the FPL.
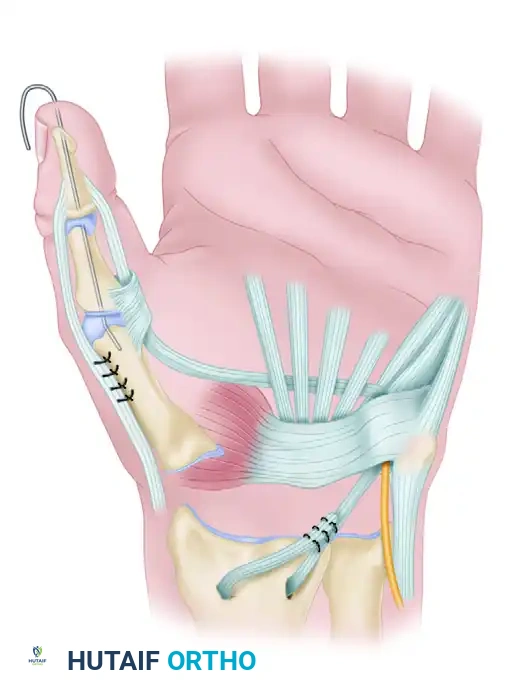
Brand's modification of the Moberg operation to create a "simple hand grip," routing the FPL through the Guyon canal.
The Bruner "Winch" Tenodesis
Bruner described a unique "winch" tenodesis for thumb flexion that relies on the preservation of active forearm supination rather than wrist extension.
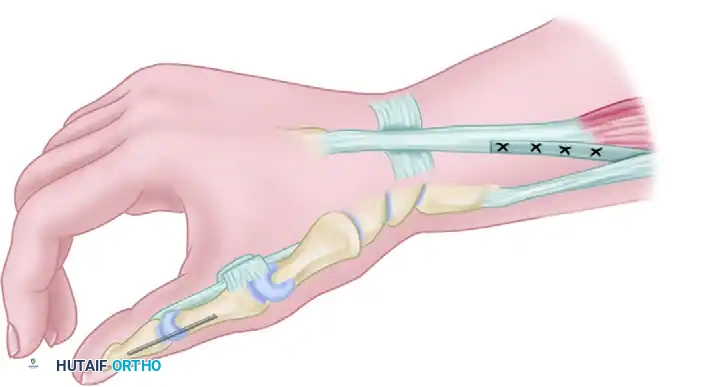
* Technique: The FPL tendon is routed around the distal ulna and anchored to its dorsal aspect through a drill hole. The thumb IP joint is often temporarily or permanently arthrodesed.
* Action: During active forearm supination, the distance between the thumb and the distal ulna increases, causing the anchored FPL tendon to tighten and flex the thumb against the index finger.
Bruner "winch" operation demonstrating the routing of the FPL tendon around the distal ulna.

Detail of the Bruner tenodesis, showing the FPL anchored against the dorsal aspect of the ulna via a drill hole.
Clinical Pearl: Electromyographic studies of patients who underwent BR to FPL transfers show a pattern of synergistic electrical activity similar to normal subjects performing thumb flexion and elbow extension. If preoperative wrist extensor torque is robust (> 10 foot-lb), an active BR transfer to the FPL for thumb flexion is preferred. If wrist torque is weak, the BR must be used to augment wrist extension (to ECRB), and thumb flexion should be achieved via tenodesis.
ADVANCED COMPREHENSIVE RECONSTRUCTIONS
Patients in ICSHT groups 4 and 5 (possessing functioning BR, ECRL, ECRB, and Pronator Teres) constitute a large percentage of those undergoing reconstructive efforts. For these patients, systematic, multi-stage programs have been developed to restore grasp, key pinch, and release. The two most prominent are the House and Zancolli reconstructions.
The House Reconstruction
House et al. described a comprehensive two-stage procedure for reconstructing digital flexion and key pinch.
Stage 1: The Extensor Phase (and Flexor Preparation)
* Digital Flexion: Accomplished by transferring the Extensor Carpi Radialis Longus (ECRL) to the Flexor Digitorum Profundus (FDP).
* Thumb Adduction/Opposition: Obtained by transferring the BR to the thumb, utilizing the Flexor Digitorum Superficialis (FDS) of the ring finger as an in situ graft.
* Pinch Augmentation: Key pinch and grasp strength are enhanced by an active transfer into the FPL using the pronator teres, the extensor or flexor carpi ulnaris, or the brachioradialis (depending on availability).
* Thumb Stabilization: The thumb carpometacarpal (CMC) joint is stabilized either by arthrodesis or by tenodesis of the abductor pollicis longus (APL).
Stage 2: The Release Phase
* Consists of intrinsic and extrinsic extensor tenodeses to allow the fingers to open when the wrist is flexed. If sufficient motor units are available, active extension of the thumb and fingers can be reconstructed.
Outcomes and Modifications:
House and Shannon compared two modifications of this reconstruction regarding thumb control: CMC fusion versus adduction-opposition transfer.
* CMC Arthrodesis: Provided the hand with better fine motor control and slightly stronger overall grasp.
* Adduction-Opposition Transfer: Afforded the ability to grasp larger objects and produced slightly greater lateral pinch force.
* Patients with bilateral reconstructions often prefer having each hand reconstructed differently (one with CMC fusion, one with transfer) to maximize their versatility in performing diverse ADLs. In House's series, key pinch increased from nonmeasurable preoperatively to an average of 3.3 kg postoperatively.
The Zancolli Two-Step Procedure
While similar in its goals to the House reconstruction, the Zancolli technique differs primarily in its approach to the release phase. Zancolli places a higher emphasis on actively restoring finger extension rather than relying solely on tenodesis effects, utilizing available expendable motors to drive the extensor digitorum communis (EDC) and extensor pollicis longus (EPL).
POSTOPERATIVE CARE AND REHABILITATION
The success of tendon transfers in tetraplegia is heavily dependent on strict adherence to postoperative rehabilitation protocols. The transferred muscle must heal securely, and the patient must undergo cortical re-education to fire the muscle in its new functional role.
Phase 1: Immobilization (Weeks 0-4)
- Immediately postoperatively, the upper extremity is immobilized in a well-padded plaster splint or cast.
- For a BR to ECRB transfer, the wrist is immobilized in 30 to 40 degrees of extension to remove all tension from the healing Pulvertaft weave.
- If a concurrent key pinch tenodesis was performed, the thumb is immobilized in the desired pinch posture against the radial aspect of the index finger.
Phase 2: Early Mobilization and Biofeedback (Weeks 4-8)
- The rigid cast is removed and replaced with a custom thermoplastic removable splint.
- Active range-of-motion (ROM) exercises are initiated under the strict supervision of a specialized hand therapist.
- Cortical Re-education: Patients are taught to fire the brachioradialis (normally an elbow flexor) to achieve wrist extension. Biofeedback techniques, including surface EMG, are highly effective in helping patients isolate and contract the transferred muscle.
- Passive stretching of the transfer is strictly avoided during this phase to prevent elongation and attenuation of the tendon weave.
Phase 3: Strengthening and Integration (Months 2-12)
- Progressive resistance exercises are gradually introduced.
- Therapy shifts toward integrating the new movements into functional ADLs (e.g., holding a pen, grasping a cup, managing zippers).
- Night Splinting: Splinting is continued between exercise sessions and strictly at night for 8 to 12 months postoperatively to protect the transfer from inadvertent stretching during sleep.
COMPLICATIONS AND PITFALLS
- Over-tensioning or Under-tensioning: The most common technical error. An overly tight BR to ECRB transfer will result in a fixed wrist extension contracture, severely limiting the patient's ability to utilize tenodesis release. An overly loose transfer will fail to provide adequate extension torque.
- Radial Nerve Injury: Iatrogenic injury to the superficial sensory branch of the radial nerve during BR mobilization can lead to painful neuromas, which are particularly devastating in patients who rely heavily on their remaining upper extremity sensibility.
- Stretching of the Transfer: Non-compliance with postoperative splinting protocols can lead to elongation of the tendon weave, resulting in a progressive loss of wrist extension power and a failure of the dependent key pinch tenodesis. Strict patient education regarding the 8-to-12-month night splinting requirement is mandatory.
You Might Also Like