Anterior Dislocation of the Lunate: Comprehensive Surgical Management and Carpal Biomechanics
Key Takeaway
Anterior dislocation of the lunate represents the final stage of perilunate instability, typically resulting from high-energy hyperextension injuries. Prompt recognition is critical to prevent irreversible median nerve damage and carpal collapse. This guide details the complex ligamentous anatomy, radiographic parameters including DISI and VISI deformities, and step-by-step surgical management utilizing combined dorsal and volar approaches for anatomic reduction and ligamentous restoration.
INTRODUCTION TO CARPAL INSTABILITY AND LUNATE DISLOCATIONS
The most common and clinically devastating carpal dislocation is the anterior dislocation of the lunate. Representing a true orthopedic emergency, this injury is the terminal event in the continuum of perilunate instability, classically described by Mayfield as Stage IV perilunate dissociation. It typically occurs following high-energy trauma, such as a fall onto an outstretched hand (FOOSH) with the wrist in extreme hyperextension, ulnar deviation, and intercarpal supination.
Failure to promptly recognize and anatomically reduce an anterior lunate dislocation leads to catastrophic outcomes, including acute median nerve compression, chronic carpal instability, advanced degenerative collapse (SLAC/SNAC), and avascular necrosis of the lunate. This comprehensive guide details the intricate pathoanatomy, radiographic evaluation, and step-by-step surgical management required to restore carpal kinematics.
PATHOANATOMY AND CARPAL BIOMECHANICS
The stability of the carpus relies entirely on its complex network of intrinsic (interosseous) and extrinsic (capsular) ligaments, as no tendons insert directly onto the proximal carpal row. The lunate acts as the intercalated segment between the rigid distal radius and the distal carpal row, making its stability highly dependent on the integrity of the scapholunate (SL) and lunotriquetral (LT) ligaments.
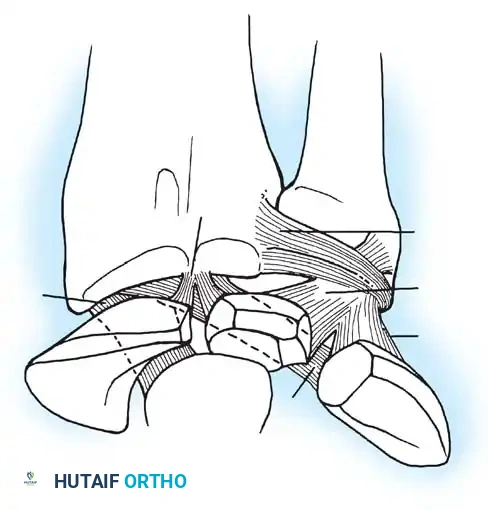
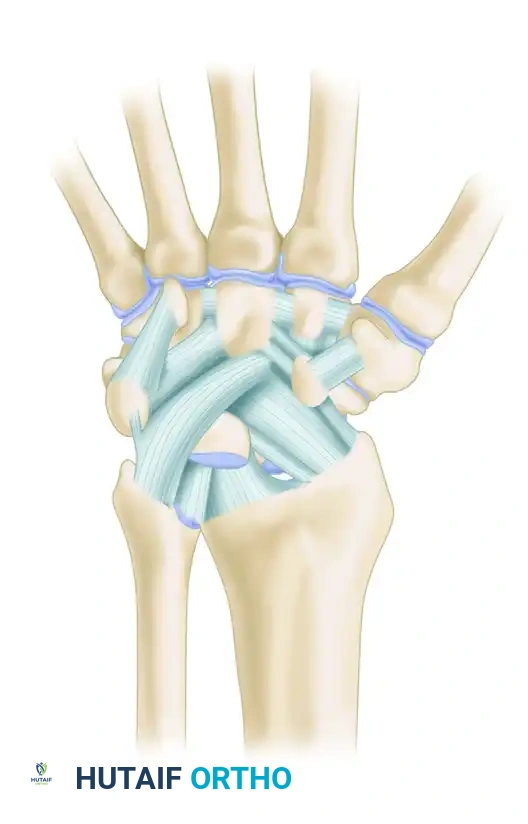
The Palmar Ligamentous Complex
The palmar radiocarpal ligaments are thicker and biomechanically more robust than their dorsal counterparts. They form a double-V configuration that dictates carpal motion and stability.
Key ligaments include:
* Radioscaphocapitate (RSC) Ligament: Acts as a critical sling supporting the scaphoid waist.
* Long and Short Radiolunate (LRL, SRL) Ligaments: Provide primary volar tethering to the lunate.
* Ulnocarpal Ligaments: Comprising the ulnolunate, ulnotriquetral, and ulnocapitate ligaments, which stabilize the ulnar aspect of the carpus.
* Space of Poirier: A central weak area in the volar capsule between the capitate and lunate. In Mayfield Stage IV injuries, the lunate extrudes volarly through this exact rent into the carpal tunnel.
Surgical Warning: The radioscapholunate (RSL) ligament, or ligament of Testut, is not a true mechanical stabilizer but rather a neurovascular conduit. Surgical approaches must respect the true mechanical stabilizers (RSC and LRL) to prevent iatrogenic instability.
RADIOGRAPHIC EVALUATION AND INSTABILITY PATTERNS
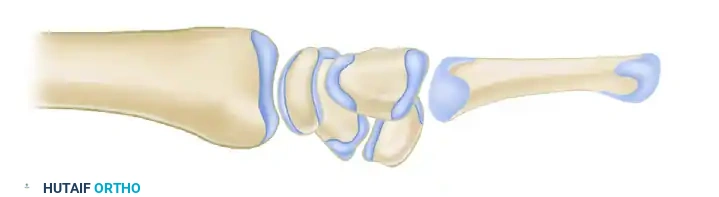
Accurate interpretation of orthogonal wrist radiographs is paramount. On a normal lateral radiographic view, the carpus exhibits a collinear arrangement. The half-moon–shaped profile of the lunate articulates congruently with the cup of the distal radius proximally and with the rounded proximal capitate distally.
Intercalated Segmental Instability
When the intrinsic ligaments fail, the lunate loses its balanced intercalated position, resulting in predictable collapse patterns dictated by the remaining intact ligaments.
Dorsal Intercalated Segmental Instability (DISI)
A DISI deformity occurs primarily following scapholunate ligament disruption. Released from the volar-flexing force of the scaphoid, the lunate extends dorsally, tethered by the intact triquetrum.
* Radiographic Criteria: The concave distal surface of the lunate points dorsally. The scapholunate angle increases to greater than 80 degrees (normal is 30° to 60°), and the capitolunate angle exceeds 20 degrees.

Volar Intercalated Segmental Instability (VISI)
A VISI deformity typically follows lunotriquetral ligament disruption. Deprived of the dorsiflexing influence of the triquetrum, the lunate follows the scaphoid into abnormal palmar flexion.
* Radiographic Criteria: The concave distal surface of the lunate points palmarly. The scapholunate angle decreases to less than 30 degrees.
Differentiating Perilunate vs. Lunate Dislocations
Understanding the difference between a perilunate dislocation and a true anterior lunate dislocation is critical for reduction maneuvers.
Dorsal Perilunate Dislocation (Mayfield Stage II/III):
The lunate remains seated within the lunate fossa of the distal radius, but the capitate and the rest of the carpus are dislocated dorsally.
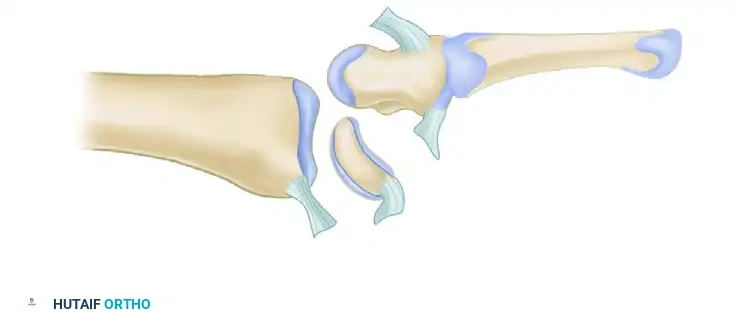
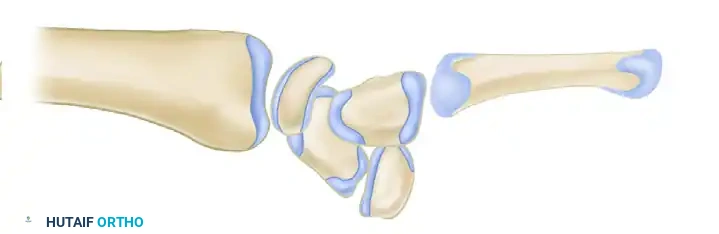
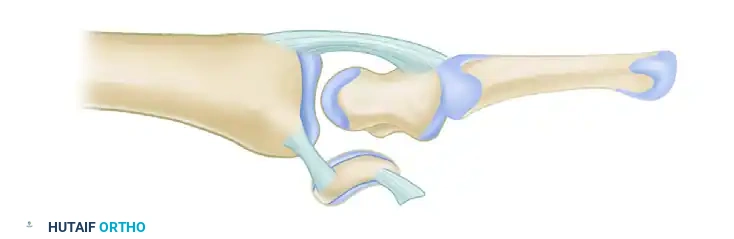
Anterior Lunate Dislocation (Mayfield Stage IV):
The dorsal radiocarpal ligaments tear, and the capitate forces the lunate volarly out of the radiocarpal joint. The lunate rotates 90 degrees and spills into the carpal tunnel, appearing as a "spilled teacup" on the lateral radiograph. The capitate drops down to articulate directly with the radius.
MIDCARPAL AND ADVANCED INSTABILITY PATTERNS
Lichtman’s Midcarpal Instability
Lichtman et al. described palmar instability in the midcarpal region (capitolunate joint) as a manifestation of laxity in the ulnar arm of the arcuate ligament (triquetrohamate and triquetrocapitate ligaments).
* Pathomechanics: This laxity allows the proximal carpal row to fall into a palmar-flexed position (VISI). Defects in the dorsal intercarpal and radiotriquetral ligaments contribute to this static malpositioning.
* Clinical Presentation: Patients report a painful "clunk" with ulnar deviation and pronation. A palmar sag is visible at the midcarpal joint.
* Physical Examination (Midcarpal Shift Test): Passively moving the hand from a relaxed neutral position into ulnar deviation reproduces the clunk. At extreme ulnar deviation, the proximal row suddenly snaps from flexion into extension, correcting the volar sag.
* Imaging: Video fluoroscopy or cineradiography is highly diagnostic, demonstrating the sudden catch-up clunk of the proximal row.
Other Complex Instability Patterns
- Capitolunate Instability Pattern (CLIP Wrist): Nondissociative instability often related to ligamentous laxity or malunited distal radius fractures altering the articular tilt.
- Ulnar Translocation of the Carpus: Characterized by the entire carpus sliding ulnarly down the radial articular slope. It is predominantly seen in severe rheumatoid arthritis due to inflammatory destruction of the extrinsic radiocarpal ligaments, though it can occur post-traumatically.
- SLAC and SNAC Wrist: Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC) represent the end-stage degenerative pathways of untreated rotary subluxation of the scaphoid. Cartilage loss progresses predictably from the radial styloid to the radioscaphoid joint, and finally the capitolunate joint, notably sparing the radiolunate joint due to its concentric articulation.
Clinical Pearl: The preservation of the radiolunate joint in SLAC/SNAC wrists is the biomechanical foundation that allows for salvage procedures such as Proximal Row Carpectomy (PRC) or Four-Corner Fusion.
SURGICAL MANAGEMENT: STEP-BY-STEP OPERATIVE TECHNIQUE
Acute anterior dislocation of the lunate requires emergent closed reduction to relieve pressure on the median nerve, followed by definitive open reduction and internal fixation (ORIF) with ligamentous repair.
1. Emergent Closed Reduction (Tavernier’s Maneuver)
Before proceeding to the operating room, a closed reduction should be attempted under conscious sedation or hematoma block.
* Traction: Apply 10 to 15 pounds of longitudinal traction using finger traps for 10 minutes to distract the carpus and open the radiocarpal space.
* Manipulation: For an anterior lunate dislocation, the wrist is extended while the surgeon's thumb applies firm, distally directed pressure on the volar aspect of the extruded lunate. The wrist is then gradually flexed to allow the capitate to snap dorsally over the lunate, capturing it back into the intercalated position.
* Immobilization: Place the wrist in a sugar-tong splint in neutral to slight flexion. Post-reduction radiographs must be scrutinized for Gilula's lines.
2. Patient Positioning and Setup
- Anesthesia: General anesthesia or regional axillary block.
- Positioning: Supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm.
- Equipment: Mini-C-arm fluoroscopy, 0.045-inch and 0.062-inch Kirschner wires (K-wires), micro-suture anchors, and a carpal distractor.
3. The Combined Dorsal and Volar Approach
A combined approach is the gold standard. The dorsal approach allows for anatomic reduction of the carpal bones and repair of the critical interosseous ligaments (SL and LT). The volar approach is mandatory to decompress the median nerve and repair the rent in the Space of Poirier.
The Volar Approach (Carpal Tunnel Release):
1. Make an extended carpal tunnel incision, crossing the wrist crease obliquely toward the flexor carpi radialis (FCR) tendon.
2. Release the transverse carpal ligament completely to decompress the median nerve, which is often contused or flattened.
3. Retract the flexor tendons ulnarly and the median nerve radially.
4. Identify the massive rent in the volar capsule (Space of Poirier). The lunate is often visible protruding through this defect.
5. Irrigate the joint and remove any osteochondral shear fragments. Do not close the capsule yet; proceed to the dorsal approach.
The Dorsal Approach:
1. Make a longitudinal dorsal incision centered over Lister's tubercle.
2. Elevate full-thickness fasciocutaneous flaps. Open the third dorsal compartment, transpose the extensor pollicis longus (EPL) tendon radially, and elevate the second and fourth compartment tendons.
3. Perform a Berger ligament-sparing capsulotomy. Create a radially based triangular flap by incising the capsule parallel to the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments.
4. Expose the proximal carpal row. The extensive tearing of the scapholunate and lunotriquetral ligaments will be evident.
4. Open Reduction and Internal Fixation
- Reduction: Using a joystick technique (inserting 0.045-inch K-wires into the scaphoid, lunate, and triquetrum), manipulate the carpal bones into anatomic alignment. Ensure the lunate is seated congruently in the lunate fossa.
- Pinning:
- Reduce the scapholunate joint, correcting the rotary subluxation of the scaphoid. Drive two 0.045-inch K-wires from the scaphoid into the lunate.
- Reduce the lunotriquetral joint and stabilize it with one or two K-wires driven from the triquetrum into the lunate.
- If midcarpal instability is profound, a K-wire may be driven from the scaphoid into the capitate to neutralize the construct.
- Fluoroscopic Confirmation: Confirm restoration of Gilula’s arcs and normal SL/LT intervals (<2mm) on AP and lateral fluoroscopy.
5. Ligamentous Repair
- Dorsal Repair: Repair the dorsal bands of the scapholunate and lunotriquetral ligaments using intraosseous suture anchors (e.g., 1.5mm or 2.0mm anchors) placed into the lunate.
- Volar Repair: Return to the volar wound. Repair the rent in the Space of Poirier and the volar extrinsic ligaments (LRL, RSC) using heavy non-absorbable sutures. This step is critical to prevent recurrent volar extrusion of the lunate.
6. Closure
- Close the dorsal capsule meticulously.
- Leave the transverse carpal ligament open to prevent postoperative compartment syndrome of the carpal tunnel.
- Close the skin loosely over drains if necessary. Apply a bulky, sterile compressive dressing and a volar-dorsal plaster splint in neutral wrist alignment.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative rehabilitation phase is as critical as the surgical execution to ensure stability while mitigating stiffness.
- Weeks 0-2: The patient remains in the postoperative bulky splint. Strict elevation and immediate active range of motion of the digits, elbow, and shoulder are mandated to prevent tendon adhesions and complex regional pain syndrome (CRPS).
- Weeks 2-8: Sutures are removed at 14 days. The patient is transitioned to a short-arm cast or a rigid custom thermoplastic splint. Pin tract care is initiated if K-wires are left percutaneous (though buried wires are preferred to reduce infection risk).
- Weeks 8-10: K-wires are removed in the clinic or under local anesthesia. The patient is referred to a specialized hand therapist. Gentle active and active-assisted range of motion (ROM) of the wrist begins. Dart-thrower's motion is encouraged as it minimizes stress on the healing SL ligament.
- Months 3-6: Passive ROM and progressive strengthening are initiated. Heavy lifting and impact activities are restricted until 6 months postoperatively.
COMPLICATIONS AND SALVAGE PROCEDURES
Despite optimal surgical management, anterior lunate dislocations carry a high risk of long-term morbidity.
- Median Neuropathy: Acute median nerve palsy is common at presentation. If symptoms do not resolve post-reduction, emergent carpal tunnel release is indicated. Chronic neuropathy may require neurolysis.
- Avascular Necrosis (AVN) of the Lunate: The extensive soft-tissue stripping inherent to a Stage IV injury disrupts the lunate's tenuous blood supply. Transient ischemia is common, but true Kienböck's-like AVN may develop, necessitating vascularized bone grafting or salvage procedures.
- Post-Traumatic Osteoarthritis: Up to 50% of patients will develop radiographic evidence of midcarpal or radiocarpal arthrosis within 5 to 10 years, regardless of reduction quality.
- Carpal Stiffness: Loss of 20% to 30% of normal wrist flexion/extension is expected. Patients must be counseled preoperatively regarding this permanent limitation.
Salvage Options:
If acute repair fails, or if the patient presents with chronic, neglected lunate dislocation (typically >8 weeks old), anatomic reduction is often impossible due to contracture and cartilage degradation. In these scenarios, salvage procedures are indicated:
* Proximal Row Carpectomy (PRC): Excision of the scaphoid, lunate, and triquetrum, allowing the capitate to articulate with the lunate fossa. Requires an intact proximal capitate articular surface.
* Four-Corner Fusion: Arthrodesis of the capitate, hamate, lunate, and triquetrum with excision of the scaphoid. Preferred if the capitate head is arthritic but the radiolunate joint is preserved.
* Total Wrist Arthrodesis: The definitive salvage for pan-carpal arthritis or failed partial fusions, providing a stable, pain-free, but immobile wrist.
===
You Might Also Like