Management of Hallux Interphalangeal and Metatarsophalangeal Joint Dislocations
Key Takeaway
Dislocation of the hallux interphalangeal and first metatarsophalangeal joints are rare but complex injuries requiring precise anatomical understanding. This guide details the pathoanatomy, Jahss classification, and step-by-step surgical techniques for open reduction. Key steps include managing the plantar plate, sesamoid complex, and utilizing Kirschner wire fixation for unstable joints to restore biomechanical alignment and function.
Introduction to Hallux Dislocations
Dislocations involving the first ray of the foot—specifically the first metatarsophalangeal (MTP) joint and the interphalangeal (IP) joint of the hallux—are relatively rare but biomechanically devastating injuries. The first ray is paramount to the weight-bearing mechanics of the human foot, particularly during the toe-off phase of the gait cycle where it must withstand forces exceeding body weight.
Because of the robust ligamentous and capsular structures stabilizing these joints, dislocations typically require high-energy trauma or severe hyperextension forces. Failure to achieve an anatomic and stable reduction can lead to chronic pain, post-traumatic arthritis, severe gait dysfunction, and progressive forefoot deformity. This comprehensive guide details the pathoanatomy, classification, and step-by-step surgical management for open reduction of both the first MTP and hallux IP joints.
Dislocation of the First Metatarsophalangeal Joint
Dislocation of the first MTP joint is an uncommon injury, primarily due to the intrinsic stability provided by the complex capsuloligamentous structures, including the plantar plate, the sesamoid complex, and the strong collateral ligaments.
Mechanism of Injury and Pathoanatomy
The classic mechanism of injury is forced hyperextension of the great toe. This extreme dorsiflexion force causes the proximal phalanx to displace onto the dorsum of the first metatarsal head and neck.
As the proximal phalanx translates dorsally, the metatarsal head is driven plantarly, frequently buttonholing through the plantar capsular structures. The metatarsal head becomes mechanically incarcerated by a tight anatomical noose:
* Medial Border: The flexor hallucis brevis (FHB) medial head and the abductor hallucis tendons.
* Lateral Border: The lateral head of the FHB and the adductor hallucis tendons.
* Dorsal Border: The displaced plantar plate and the deep transverse metatarsal ligament, which have been stripped from their proximal attachments and pulled dorsally over the metatarsal neck.
* Plantar Border: The unyielding plantar aponeurosis, which acts as a tension band preventing plantar reduction maneuvers.
Furthermore, the flexor hallucis longus (FHL) tendon typically subluxates and lies lateral to the trapped metatarsal head, further complicating closed reduction efforts.
💡 Clinical Pearl: Associated Injuries
Always maintain a high index of suspicion for concomitant injuries. In complex dislocations of the MTP joints, tarsometatarsal (Lisfranc) joint injuries are frequently present. Initial radiographs must be scrutinized carefully to rule out subtle midfoot instability. Furthermore, more than half of these high-energy injuries present as open dislocations, necessitating emergent open débridement, copious irrigation, and relocation.
The Jahss Classification System
The Jahss classification is the universally accepted system for categorizing first MTP joint dislocations. It is based on the integrity of the intersesamoid ligament and the sesamoid bones themselves, which dictates whether the dislocation is reducible by closed means.
- Type I: The intersesamoid ligament remains completely intact. The entire sesamoid complex and plantar plate are displaced dorsally over the metatarsal neck. Because the anatomical noose is intact, the metatarsal head is firmly trapped. Type I injuries are irreducible by closed means and mandate open reduction.
- Type IIA: The intersesamoid ligament is ruptured. This rupture allows the tibial and fibular sesamoids to separate widely. Because the restrictive noose is broken, Type IIA injuries can frequently be reduced via closed manipulation.
- Type IIB: The intersesamoid ligament remains intact, but there is a transverse fracture of one of the sesamoids (usually the tibial sesamoid). The distal fracture fragment is pulled distally with the plantar plate. Similar to Type IIA, the disruption of the complex's integrity usually allows for successful closed reduction.
Radiographic Assessment
Standard weight-bearing (if tolerated) anteroposterior (AP), lateral, and oblique radiographs of the foot are mandatory. The lateral view will clearly demonstrate the dorsal displacement of the proximal phalanx. The AP view is critical for assessing the sesamoid complex to apply the Jahss classification.


Radiographic examples demonstrating complex dislocation patterns of the first ray. Note the displacement of the sesamoid complex which dictates the Jahss classification and subsequent reducibility.
Surgical Technique: Open Reduction of the First MTP Joint
When closed reduction is impossible (Jahss Type I) or fails, open reduction is indicated.
1. Patient Positioning and Anesthesia
The patient is placed supine on the operating table. A regional ankle block or general anesthesia may be utilized. A calf or thigh tourniquet is applied to ensure a bloodless surgical field.
2. Surgical Approach
A midline medial approach is highly recommended.
* Make a longitudinal incision centered over the medial aspect of the first MTP joint, extending from the mid-shaft of the first metatarsal to the mid-shaft of the proximal phalanx.
* Carefully dissect through the subcutaneous tissues, taking care to identify and protect the medial dorsal cutaneous nerve and the proper plantar digital nerve to the hallux.
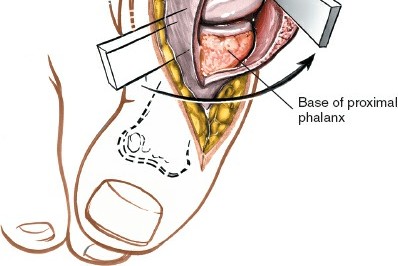
3. Joint Exposure and Decompression
* Identify the abductor hallucis tendon and retract it plantarly.
* The metatarsal head will typically be found protruding medially and plantarly, trapped by the dorsal displacement of the plantar plate and the intact intersesamoid ligament.
* To release the incarceration, a longitudinal incision is made through the medial capsule.
* If the plantar plate and intersesamoid ligament are tightly bound over the metatarsal neck, a Freer elevator or a small curved hemostat is passed dorsally to carefully stretch or incise the obstructing structures. In severe Type I cases, a controlled partial release of the deep transverse metatarsal ligament may be required to allow the sesamoid complex to translate plantarly.
4. Reduction and Stabilization
* Apply longitudinal traction to the hallux while simultaneously applying plantar-directed pressure to the proximal phalanx and dorsal-directed pressure to the metatarsal head.
* Once reduced, assess the stability of the joint through a full range of motion.
* If the joint is highly unstable, temporary transarticular fixation with a 0.062-inch Kirschner wire (K-wire) driven from the tip of the toe across the MTP joint may be necessary, though capsular repair is often sufficient.
* Repair the medial capsule and abductor hallucis meticulously with heavy absorbable sutures (e.g., 2-0 Vicryl) to restore medial stability.
⚠️ Surgical Warning: Avascular Necrosis
Excessive stripping of the soft tissues around the first metatarsal head during open reduction can compromise its precarious blood supply, leading to iatrogenic avascular necrosis (AVN). Dissection must be strictly limited to the structures necessary to achieve reduction.
Dislocation of the Interphalangeal (IP) Joint of the Hallux
While less common than MTP joint dislocations, IP joint dislocations present unique challenges. The IP joint is a hinge joint stabilized by strong collateral ligaments and a thick plantar plate. An accessory sesamoid bone is present within the plantar plate of the IP joint in approximately 50% of individuals.
During a hyperextension injury, the distal phalanx dislocates dorsally. The plantar plate frequently avulses from its proximal attachment on the proximal phalanx and becomes interposed within the joint space. If the IP joint sesamoid is present, it is pulled dorsally into the joint alongside the plantar plate, creating an absolute mechanical block to closed reduction.
Surgical Technique: Open Reduction of the Hallux IP Joint
1. Incision and Exposure
* Make a dorsal inverted L-shaped incision.
* The transverse limb of the "L" should be placed directly over the IP joint line.
* The longitudinal limb should extend proximally along the dorsolateral aspect of the proximal phalanx. This dorsolateral positioning helps avoid the more prominent medial neurovascular bundle.
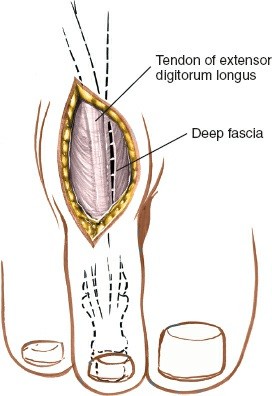
* Carefully deepen the incision. Crucial Step: Identify and meticulously preserve the insertion of the extensor hallucis longus (EHL) tendon into the dorsal base of the distal phalanx.
2. Identifying the Obstruction
* Retract the skin flaps. On one side of the EHL tendon (usually laterally), explore the joint space to identify the interposed plantar plate.
* Identification of the plantar plate is significantly easier if an IP joint sesamoid is present within it, as the firm, cartilaginous or bony mass can be palpated and visualized.
3. Releasing the Plantar Plate
* Once the plantar plate is identified, make a precise 3- to 4-mm longitudinal incision directly into it. This small incision relieves the tension of the entrapped structure.
* Apply longitudinal traction to the great toe and attempt reduction.
4. Managing the Irreducible Joint
* If reduction cannot be accomplished with simple traction and the capsular incision, the plantar plate and sesamoid are likely still firmly wedged dorsal to the condyles of the proximal phalanx.
* Insert a blunt probe or a small Freer elevator into the joint space.
* Use the elevator to physically lever and displace the sesamoid and plantar plate distally, slipping them over the condyles of the proximal phalanx, while an assistant maintains strong longitudinal traction on the great toe.
5. Assessment of Stability and Fixation
* Once anatomic reduction is achieved, assess the joint for stability.
* Stable Reduction: If the joint remains reduced through a functional range of motion and does not subluxate, no transarticular pin fixation is required.
* Unstable Reduction: If the joint is grossly unstable or tends to subluxate dorsally upon release of traction, internal fixation is mandatory.
* Hold the joint in an anatomically reduced, neutral position.
* Drill one or two 0.062-inch Kirschner wires (K-wires) longitudinally. The wires should be driven from distal to proximal, starting at the tip of the distal phalanx, crossing the IP joint, and coming to rest securely in the subchondral bone at the base of the proximal phalanx.
* Cut the K-wires approximately 2 mm outside the skin to allow for easy removal in the clinic. Bend the tips slightly or apply pin caps to prevent proximal migration.
Postoperative Care and Rehabilitation Protocol
Strict adherence to the postoperative protocol is essential to balance the need for tissue healing with the prevention of severe joint stiffness.
Phase I: Acute Healing (Days 0 - 3)
* The surgical site is dressed with sterile, non-adherent dressings.
* Apply a well-padded short-leg cast extending past the toes to protect the K-wires and immobilize the foot.
* The patient is instructed to strictly rest and elevate the extremity above heart level for the first 3 days.
* Activity is restricted to bathroom privileges only to minimize edema and the risk of marginal wound necrosis.
Phase II: Protected Weight Bearing (Days 4 - 21)
* The patient may begin partial weight-bearing (PWB) using crutches.
* Elevation should continue when seated.
* Monitor the pin sites closely for any signs of superficial infection.
Phase III: Pin Removal and Mobilization (Week 3)
* At exactly 3 weeks postoperatively, the transarticular K-wires are removed in the clinic.
* The short-leg cast is discontinued.
* The patient is transitioned to a rigid, postoperative wooden-soled shoe.
* Weight-bearing to tolerance (WBAT) is now permitted.
* Rehabilitation: Active and active-assisted range of motion (ROM) exercises of the interphalangeal joint are initiated immediately upon pin removal to combat capsular contracture.
Phase IV: Return to Function (Week 6 and Beyond)
* At 6 weeks, if clinical healing is progressing well, the patient may transition out of the wooden-soled shoe.
* Wearing of a standard shoe with a wide, accommodating toe box is allowed.
* Aggressive physical therapy focusing on intrinsic foot muscle strengthening, gait retraining, and maximizing first ray ROM is continued.
Complications and Clinical Outcomes
Surgeons must counsel patients extensively regarding the expected outcomes and potential complications following open reduction of hallux dislocations.
- Decreased Range of Motion: This is the most universal complication. Almost all patients will experience some degree of permanent limitation in MTP or IP joint motion. However, clinical studies indicate that this stiffness rarely reduces the patient's endurance for work or routine exercise.
- Plantar Sensitivities: Altered biomechanics and scar tissue formation can lead to chronic plantar sensitivities under the first metatarsal head or the IP joint. In a notable case series, several patients required the full-time use of a custom orthosis with a first ray cutout or metatarsal pad to manage this discomfort.
- Wound Complications: Marginal wound necrosis and prolonged swelling of the toe are common, particularly due to the tenuous dorsal skin envelope and the high-energy nature of the initial trauma. With strict adherence to rest, elevation, and edema control, these are generally not alarming problems and resolve with time.
- Recurrent Dislocation: While rare, recurrent dislocation has been noted, particularly in patients who return to high-impact activities (e.g., jogging) prematurely before adequate capsuloligamentous healing has occurred. Strict adherence to the 6-week protected weight-bearing timeline is crucial.
You Might Also Like