Sternoclavicular Joint Dislocations: Comprehensive Surgical Management
Key Takeaway
Sternoclavicular joint dislocations represent complex orthopedic challenges requiring precise diagnostic and therapeutic strategies. While anterior dislocations are common and often managed nonoperatively, posterior dislocations constitute true orthopedic emergencies due to the proximity of vital mediastinal structures. This comprehensive guide details the biomechanics, advanced imaging protocols, closed reduction maneuvers, and meticulous surgical techniques necessary for managing both acute and chronic sternoclavicular instability, emphasizing the absolute contraindication of transarticular pin fixation.
INTRODUCTION TO STERNOCLAVICULAR JOINT INSTABILITY
The sternoclavicular (SC) joint represents the sole true synovial articulation between the axial skeleton and the upper extremity. Because of its unique diarthrodial saddle configuration, it possesses minimal intrinsic osseous stability, relying almost entirely on a robust complex of surrounding ligaments. Traumatic dislocation of the sternoclavicular joint is a relatively rare but highly significant clinical entity, typically resulting from high-energy indirect forces transmitted through the shoulder girdle.
While anterior dislocations are the most frequent and generally carry a benign long-term prognosis even when irreducible, posterior (retrosternal) dislocations are potentially life-threatening. The posterior displacement of the medial clavicle places the critical structures of the superior mediastinum—including the trachea, esophagus, great vessels, and brachial plexus—at immediate risk of compression or laceration. Consequently, the management of SC joint dislocations demands a profound understanding of regional anatomy, precise diagnostic imaging, and meticulous surgical technique.
SURGICAL ANATOMY AND BIOMECHANICS
To master the operative and nonoperative management of the SC joint, the orthopedic surgeon must first understand its complex stabilizing structures. The joint is a diarthrodial saddle joint, but the articular surfaces are highly incongruent. Less than half of the medial clavicle articulates with the shallow clavicular notch of the manubrium sterni.
The Ligamentous Stabilizers
Stability is conferred by four primary soft-tissue structures:
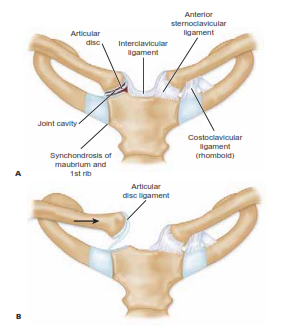
* Capsular Ligaments: The joint capsule is thickened anteriorly and posteriorly. The posterior capsule is the most robust structure and represents the primary restraint to both anterior and posterior translation of the medial clavicle.
* Intra-articular Disc (Meniscus): A dense fibrocartilaginous disc divides the joint into two separate synovial cavities. It attaches superiorly to the medial clavicle and inferiorly to the first costal cartilage, acting as a hinge and a shock absorber.
* Interclavicular Ligament: Spanning the jugular notch, this ligament connects the superomedial aspects of both clavicles, resisting downward displacement of the distal clavicle.
* Costoclavicular (Rhomboid) Ligament: A dense, bipartite ligament connecting the inferior surface of the medial clavicle to the first rib and its costal cartilage. It consists of anterior and posterior fascicles that cross obliquely, providing critical stability against superior displacement and rotation.
Clinical Pearl: Whether the sternoclavicular joint subluxates or fully dislocates depends entirely on the sequential failure of these structures. Complete dislocation requires the rupture of the capsular ligaments, the intra-articular disc, and the costoclavicular ligament.
Mediastinal Proximity
The posterior aspect of the SC joint is separated from the superior mediastinum by only a few millimeters. Structures immediately posterior include the innominate (brachiocephalic) veins, the superior vena cava, the aortic arch, the right brachiocephalic artery, the left common carotid artery, the trachea, the esophagus, and the thoracic duct. This anatomical reality dictates the catastrophic potential of posterior dislocations.
MECHANISM OF INJURY AND CLASSIFICATION
Traumatic dislocations are broadly classified by the direction of the displaced medial clavicle relative to the sternum.
Anterior Dislocations
Anterior dislocations are the most common. They typically result from an indirect force applied to the anterolateral aspect of the shoulder with the arm abducted. This force rolls the shoulder backward, levering the medial clavicle anteriorly out of the sternal articulation. Patients present with considerable pain, localized swelling, and a prominent, palpable deformity over the medial chest wall. The displaced clavicle may appear elevated or depressed near the first rib, depending on the exact pattern of ligamentous disruption.
Posterior Dislocations
Posterior dislocations result from either a direct blow to the anteromedial clavicle or, more commonly, an indirect force applied to the posterolateral shoulder, driving the shoulder forward and levering the medial clavicle posteriorly.
Surgical Warning: Posterior dislocation is a true orthopedic emergency. The posteriorly displaced medial clavicle can produce respiratory distress (stridor), venous congestion, arterial insufficiency, brachial plexus compression, and even myocardial conduction abnormalities.
The Pediatric and Young Adult Variant: Physeal Fractures
Rockwood extensively documented that the medial clavicular epiphysis is the last physis in the body to close, typically fusing between the ages of 23 and 25 years.
Clinical Pearl: In patients younger than 25 years old, what appears clinically and radiographically as a sternoclavicular dislocation is almost always a Salter-Harris type I or II fracture through the medial clavicular physis. The periosteal sleeve remains attached to the sternum via the intact SC ligaments, while the clavicular shaft displaces.
CLINICAL EVALUATION AND ADVANCED IMAGING
Physical examination reveals asymmetry of the medial clavicles. In anterior dislocations, the medial clavicle is prominent. In posterior dislocations, a palpable void may be noted at the SC joint, accompanied by severe pain, shoulder protraction, and potential signs of mediastinal compression (dysphagia, dyspnea, hoarseness, or diminished upper extremity pulses).
Radiographic Assessment
Standard anteroposterior (AP) radiographs of the chest or shoulder are notoriously difficult to interpret due to the overlapping shadows of the ribs, sternum, and vertebrae.
- The Serendipity View (Apical Lordotic View): Centered over the sternum with the X-ray tube tilted 40 degrees cephalad. This view is highly diagnostic. The medial end of the dislocated clavicle will project superiorly (anterior dislocation) or inferiorly (posterior dislocation) relative to the normal contralateral clavicle.
- Special Views: Techniques described by Heinig, Hobbs, Kattan, and Rockwood can provide additional tangential perspectives, though they have largely been superseded by advanced cross-sectional imaging.
Computed Tomography (CT)
CT scanning is the absolute gold standard for evaluating SC joint pathology. Axial and coronal reconstructions, along with 3D rendering, definitively differentiate between true dislocations and medial physeal fractures. Furthermore, CT angiography (CTA) is critical in posterior dislocations to assess the proximity of the medial clavicle to the great vessels and to rule out occult vascular injury.
MANAGEMENT OF ACUTE ANTERIOR DISLOCATIONS
Acute anterior dislocations are generally managed nonoperatively. While closed reduction can be achieved, maintaining the reduction is notoriously difficult due to the complete disruption of the anterior capsule and costoclavicular ligaments.
Closed Reduction Technique (Heinig's Method)
- Preparation: Meticulous sterile technique is required. The hematoma is infiltrated with a local anesthetic (hematoma block), or the procedure is performed under conscious sedation.
- Positioning: The patient is placed supine with a large, firm sandbag or rolled towel positioned vertically between the scapulae to allow the shoulders to fall posteriorly.
- Maneuver: Traction is applied to the affected extremity in abduction and extension. Simultaneously, direct downward (posterior) pressure is applied over the prominent medial end of the clavicle.
- Post-Reduction: The joint is often grossly unstable upon release of pressure.
Decision Making in Anterior Instability
If the joint remains unstable and re-dislocates, the deformity is generally accepted. Interposition of the torn joint capsule or the intra-articular disc often renders the dislocation irreducible. While the medial clavicle causes an unsightly prominence, functional outcomes are typically excellent, and little disability is expected, particularly for sedentary patients.
Operative intervention for acute anterior dislocations is rarely indicated. If chronic instability becomes painful and functionally limiting, delayed ligament reconstruction or resection of the medial end of the clavicle may be considered.
MANAGEMENT OF ACUTE POSTERIOR DISLOCATIONS
Posterior dislocations demand immediate attention. If the patient exhibits signs of hemodynamic compromise, airway obstruction, or vascular injury, emergent reduction is required, often in conjunction with a trauma or thoracic surgeon.
Closed Reduction Techniques
Closed reduction should be attempted in the operating room under general anesthesia, with a thoracic surgeon available on standby due to the risk of catastrophic hemorrhage if a vessel has been lacerated by the clavicle and is tamponaded by the bone.
Standard Abduction-Traction Technique:
1. Positioning: Patient supine with a large sandbag between the scapulae.
2. Maneuver: Lateral traction is applied to the affected arm in abduction and extension.
3. Manipulation: The surgeon grasps the medial clavicle with their fingers and exerts strong anterior traction.
4. Towel Clip Assist: If manual grasping is insufficient, the skin is sterilely prepped, and a sterile penetrating towel clip is used to percutaneously grasp the medial clavicle to apply direct anterior traction.
The Buckerfield and Castle Maneuver:
An alternative technique utilizing a lever-axis principle.
1. Traction is applied to the affected arm with the shoulder in adduction.
2. A posteriorly directed force is applied to the lateral shoulder and distal clavicle.
3. This leverages the medial clavicle anteriorly, using the first rib as a fulcrum.
Post-Reduction Protocol
Unlike anterior dislocations, posterior dislocations are usually stable once reduced because the intact anterior capsule prevents over-reduction, and the scapula rests against the posterior thoracic wall.
* Immobilization: A figure-of-eight soft dressing, a commercially prepared clavicular strap, or a figure-of-eight plaster dressing is applied.
* Duration: Immobilization is maintained for 4 weeks.
* Rehabilitation: Activities and heavy lifting are strictly restricted for a minimum of 6 weeks to allow capsuloligamentous healing.
OPERATIVE MANAGEMENT AND SURGICAL APPROACHES
Surgical intervention is fraught with risk and must be approached with profound respect for the regional anatomy. Reports by Worman and Leagus, Brown, and Omer suggest that the incidence of significant complications approaches 25% following sternoclavicular procedures.
Indications for Surgery
- Irreducible Posterior Dislocation: Failure to achieve closed reduction under general anesthesia. The joint cannot be left posteriorly dislocated due to the persistent danger to mediastinal structures.
- Chronic, Symptomatic Anterior Dislocation: Old, unreduced, or recurrent anterior dislocations that cause severe pain or functional limitation (rare).
Surgical Warning: The Absolute Contraindication of Transarticular Pins
Under no circumstances should transarticular pins (Steinmann pins or Kirschner wires) be used to stabilize the sternoclavicular joint. The literature is replete with reports of fatal complications resulting from the migration of intact or broken pins into the heart, pulmonary artery, innominate artery, or aorta. Fixation must rely entirely on robust suture or graft reconstruction.
Open Reduction and Ligament Reconstruction (Kennedy's Technique)
Because of the significant injury to the joint capsule, articular disc, and extra-articular ligaments, simple open reduction is insufficient. Kennedy and others recommend formal ligament reconstruction.
Preoperative Preparation:
* General anesthesia with endotracheal intubation.
* A cardiothoracic surgeon must be consulted and ideally present or immediately available.
* Blood products must be typed and crossed.
Surgical Approach:
1. Incision: A 7- to 8-cm transverse or L-shaped incision is made centered over the SC joint, extending laterally over the medial clavicle and medially over the manubrium.
2. Dissection: The platysma is divided. The periosteum of the medial clavicle is incised longitudinally.
3. Subperiosteal Exposure: Dissection must remain strictly subperiosteal. A blunt retractor (e.g., a malleable or Doyen retractor) is carefully placed posterior to the medial clavicle to protect the mediastinal structures.
4. Joint Debridement: The joint is inspected. The torn intra-articular disc and interposed capsular remnants are excised to allow reduction.
Reconstruction (Figure-of-Eight Graft):
Autograft (semitendinosus, gracilis, or palmaris longus) or allograft is utilized to reconstruct the stabilizing ligaments.
1. Drill Holes: Using a 3.2mm or 4.0mm drill, two holes are created in the medial clavicle (superior to inferior) and two corresponding holes in the manubrium. Crucial Step: A protective retractor must be placed behind the bone during drilling to prevent the drill bit from plunging into the mediastinum.
2. Graft Passage: The graft is passed through the drill holes in a figure-of-eight fashion.
3. Reduction and Fixation: The clavicle is anatomically reduced into the sternal notch. The graft is tensioned and sutured to itself using heavy, non-absorbable sutures (e.g., #2 or #5 FiberWire).
4. Capsular Repair: The remaining anterior capsule and periosteal sleeve are imbricated over the reconstruction for added stability.
Postoperative Protocol
- The patient is placed in a strict shoulder immobilizer or sling for 4 to 6 weeks.
- Pendulum exercises may begin at 2 weeks, but active elevation above 90 degrees is prohibited until 6 weeks.
-
Full return to contact sports or heavy labor is delayed until 4 to 6 months postoperatively, contingent upon radiographic maintenance of reduction and clinical stability.
You Might Also Like