Mastering Clavicle Excision and Sternoclavicular Joint Reconstruction
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Mastering Clavicle Excision and Sternoclavicular Joint Reconstruction. Clavicle excision and sternoclavicular joint reconstruction address various pathologic disorders affecting the medial clavicle, most commonly osteoarthritis. Other conditions include rheumatoid arthritis, crystal deposition disease, and instability. These procedures aim to alleviate severe symptoms, pain, or dysfunction arising from these medical issues.
Introduction and Epidemiology
Pathologic disorders affecting the medial clavicle and the sternoclavicular joint encompass a broad spectrum of degenerative, inflammatory, traumatic, and idiopathic conditions. Osteoarthritis represents the most frequently encountered pathology in this region, predominantly affecting male laborers subjected to repetitive load-bearing activities, perimenopausal women, and patients who have undergone radical neck dissection. The disruption of normal shoulder girdle kinematics following radical neck dissection often leads to accelerated degenerative changes at the medial clavicle.
Other significant conditions affecting the sternoclavicular joint include rheumatoid arthritis, seronegative spondyloarthropathies, crystal deposition diseases, sternoclavicular hyperostosis, condensing osteitis, and avascular necrosis of the medial clavicle (Friedrich disease). While primary involvement of the sternoclavicular joint in rheumatologic conditions is relatively rare, it frequently manifests in the late stages of systemic disease.

Infection of the sternoclavicular joint is an uncommon but potentially devastating condition. It is disproportionately observed in intravenous drug users, immunocompromised individuals, and patients with indwelling central venous catheters. The clinical presentation may initially appear indolent, but progression can lead to mediastinitis or osteomyelitis. Prompt aspiration for Gram stain, cell count, and culture is mandatory when infection is suspected, followed by aggressive surgical irrigation and débridement.

Instability of the sternoclavicular joint is a rare entity, accounting for less than 3% of all shoulder girdle injuries, yet it carries profound clinical significance. Traumatic instability is classified by the direction of clavicular head displacement relative to the sternum, categorizing into superior, anterior, or posterior dislocations. Posterior instability is a surgical emergency due to the proximity of life-threatening retrosternal structures, including the brachiocephalic vessels, trachea, and esophagus. Conversely, atraumatic instability is typically anterior, insidious in onset, and frequently associated with generalized ligamentous laxity or collagen disorders. Symptomatic traumatic instability necessitates closed reduction and potential ligamentous reconstruction, whereas primary resection of the clavicular head is contraindicated in the setting of acute instability.
Surgical Anatomy and Biomechanics
The sternoclavicular joint is a diarthrodial, saddle-shaped articulation that serves as the sole true synovial articulation between the upper extremity appendicular skeleton and the axial skeleton. It is widely considered the most unconstrained joint in the human body. The articular surface of the medial clavicle is disproportionately larger than the shallow clavicular notch of the manubrium, resulting in less than half of the medial clavicle articulating with the sternum at any given time. This inherent osseous incongruity dictates that the stability of the sternoclavicular joint is almost entirely dependent on its surrounding ligamentous and capsular envelope.
An intra-articular fibrocartilaginous disc bisects the joint, attaching superiorly to the medial clavicle and inferiorly to the first costal cartilage. This disc functions to absorb axial loads and mitigate superior displacement of the medial clavicle.

The primary static restraints of the sternoclavicular joint include four major ligamentous complexes:
1. Capsular Ligaments The anterior and posterior capsules are the most critical stabilizers. Biomechanical studies demonstrate that the posterior capsule is the primary restraint to both anterior and posterior translation of the medial clavicle. Disruption of the posterior capsule is a prerequisite for significant sternoclavicular instability.
2. Costoclavicular Ligament Also known as the rhomboid ligament, this robust structure consists of anterior and posterior fascicles. It anchors the inferior aspect of the medial clavicle to the first rib and its costal cartilage. It serves as the primary pivot point for clavicular motion in the axial plane and restrains superior elevation of the clavicle.
3. Interclavicular Ligament Connecting the superomedial aspects of both clavicles across the jugular notch, this ligament provides minimal functional restraint but assists in resisting downward glide of the lateral clavicle.
4. Intra-articular Disc Ligament Contributes to joint congruity and shock absorption.

The medial clavicular epiphysis is the last physis to ossify (appearing around age 18) and the last to fuse (fusing between ages 22 and 25). Consequently, many presumed sternoclavicular dislocations in young adults are, in fact, physeal fractures (Salter-Harris types I or II) of the medial clavicle.
The biomechanics of traumatic instability are dictated by the vector of the applied force. If an indirect force impacts the anterior shoulder, the shoulder girdle is driven posteriorly. The clavicle utilizes the first rib as a fulcrum, levering the medial clavicle head anteriorly and resulting in an anterior dislocation. Conversely, a force impacting the posterior shoulder drives the shoulder girdle anteriorly, leveraging the medial clavicle posteriorly into the mediastinum. Direct blows to the medial clavicle can also precipitate posterior dislocations.

Indications and Contraindications
Surgical intervention at the sternoclavicular joint is reserved for specific, refractory pathologies due to the inherent risks associated with the retrosternal anatomy. Medial clavicle excision is primarily indicated for degenerative or inflammatory arthritis that has failed exhaustive conservative management. The critical surgical tenet during excision is the preservation of the costoclavicular ligament; resection exceeding 1.5 cm of the medial clavicle will compromise this ligament, leading to iatrogenic instability and profound morbidity.
Sternoclavicular joint reconstruction is indicated for symptomatic, recurrent traumatic instability, irreducible acute posterior dislocations, or chronic posterior dislocations causing mediastinal compression. Atraumatic anterior instability is virtually never an indication for operative reconstruction, as these patients typically achieve functional adaptation through physical therapy, and surgical outcomes in this cohort are historically poor.

| Pathology | Operative Indications | Non Operative Indications |
|---|---|---|
| Osteoarthritis | Refractory pain failing >6 months of conservative therapy; functional limitation. | Mild to moderate symptoms; high surgical risk; perimenopausal transient synovitis. |
| Anterior Dislocation | Chronic, highly symptomatic instability failing physical therapy (rare); skin compromise. | Acute anterior dislocation; asymptomatic chronic dislocation; voluntary atraumatic instability. |
| Posterior Dislocation | Acute dislocation failing closed reduction; signs of vascular, tracheal, or esophageal compression. | Acute dislocation successfully reduced closed with stable post-reduction examination. |
| Infection | Abscess formation; osteomyelitis; failure of systemic antibiotics; joint destruction. | Early cellulitis without intra-articular purulence (rarely applicable). |
| Sternoclavicular Hyperostosis | Severe functional impairment; impending airway/vascular compromise (rare). | Asymptomatic or mildly symptomatic hyperostosis; SAPHO syndrome responding to medical management. |
Pre Operative Planning and Patient Positioning
Thorough preoperative evaluation is paramount. Standard radiographic evaluation includes a true anteroposterior view and the Serendipity view. The Serendipity view is obtained with the patient supine and the X-ray beam angled 40 degrees cephalad, centered on the manubrium. In a normal joint, both clavicles intersect the same horizontal plane. In an anterior dislocation, the affected clavicle appears superior to the contralateral side; in a posterior dislocation, it appears inferior.

Advanced imaging is mandatory for surgical planning. A computed tomography scan with three-dimensional reconstruction is the gold standard for evaluating sternoclavicular joint pathology. It accurately delineates the direction of dislocation, assesses osseous morphology for degenerative changes, and evaluates the integrity of the medial clavicular epiphysis in young adults. Most importantly, a contrast-enhanced CT angiogram of the chest is critical in cases of posterior dislocation to evaluate the proximity of the displaced clavicle to the brachiocephalic artery, subclavian vein, trachea, and esophagus. Magnetic resonance imaging may be utilized to assess the intra-articular disc, evaluate for osteomyelitis, or diagnose early avascular necrosis.

A multidisciplinary approach is essential for any surgical intervention involving the sternoclavicular joint, particularly posterior dislocations. A thoracic or vascular surgeon must be consulted preoperatively and ideally be present or immediately available in the operating room. The surgical facility must be equipped with a sternal saw and major vascular instrumentation.
The patient is positioned supine on a radiolucent operating table. A bump is placed vertically between the scapulae to allow the shoulders to fall posteriorly, which aids in reducing posterior dislocations and opens the anterior joint space. The head of the bed is elevated 30 degrees (reverse Trendelenburg) to decrease venous engorgement. The operative field is prepped widely, from the mandible to the costal margin, and laterally to the bilateral acromioclavicular joints. The ipsilateral arm is draped free to allow for intraoperative manipulation.
Detailed Surgical Approach and Technique
Medial Clavicle Excision
The primary goal of medial clavicle excision is to resect the arthritic articular surface while meticulously preserving the costoclavicular ligament to prevent postoperative instability.
- Incision and Dissection A 5 to 7 cm transverse or slightly oblique incision is made centered over the medial clavicle and sternoclavicular joint. Subcutaneous tissues are divided, and the platysma is incised in line with the skin incision.
- Fascial Incision The investing fascia of the sternocleidomastoid and pectoralis major is incised sharply. The periosteum over the medial clavicle is elevated as a continuous sleeve. It is critical to preserve the robust anterior capsule, which will be repaired at the conclusion of the procedure.
- Joint Arthrotomy The joint is entered, and the intra-articular disc is identified and typically excised if severely degenerated.
- Osteotomy Using a micro-sagittal saw or an osteotome, the medial clavicle is resected. The osteotomy must be strictly limited to 1.0 to 1.5 cm from the articular margin. Resection beyond this point invariably compromises the costoclavicular ligament insertion.
- Closure The remaining medial clavicle is smoothed with a rasp. The robust periosteal sleeve and anterior capsule are meticulously imbricated and repaired using heavy non-absorbable sutures to provide a static restraint against anterior translation.

Sternoclavicular Joint Reconstruction
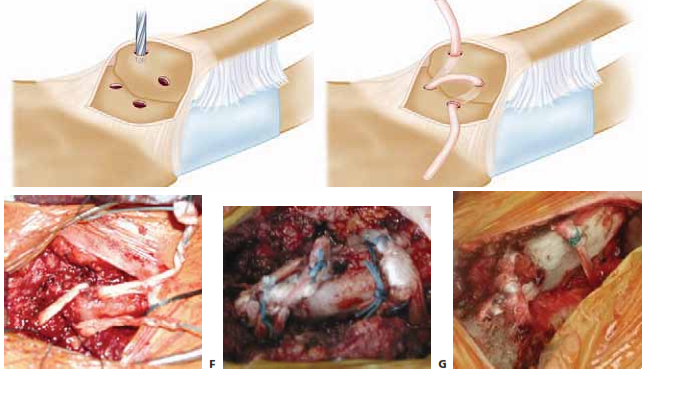
When the ligamentous restraints are irreparably damaged, or if an iatrogenic excision has compromised the costoclavicular ligament, a soft tissue reconstruction is required. The figure-of-eight autograft reconstruction (using semitendinosus or gracilis) is the biomechanically superior and most widely accepted technique.
- Exposure The joint is exposed as described above. The medial clavicle and the manubrium are cleared of soft tissue, preserving the periosteal sleeve.
- Preparation of Drill Holes A malleable retractor is carefully placed posterior to the manubrium and medial clavicle to protect the mediastinal structures. Two drill holes are created in the manubrium, typically 1.5 cm apart, and two corresponding holes are drilled in the medial clavicle. The holes should be 4.0 to 4.5 mm in diameter to accommodate the graft.
- Graft Passage The autograft or allograft is passed in a figure-of-eight fashion through the osseous tunnels. The graft must cross the joint space to replicate the function of the anterior and posterior capsules.
- Tensioning and Fixation The joint is anatomically reduced. The graft is tensioned and secured either by suturing the graft limbs to themselves using high-tensile non-absorbable sutures or by utilizing interference screws within the osseous tunnels.
- Augmentation The remnant anterior capsule and periosteum are closed over the graft to provide additional stability.

Closed Reduction of Posterior Dislocation
Acute posterior dislocations should initially be managed with closed reduction under procedural sedation or general anesthesia in the operating room.
1. The patient is positioned supine with a bolster between the scapulae.
2. The surgeon applies lateral traction to the abducted and extended arm.
3. If reduction is not achieved, the surgeon may sterilely prep the chest, apply a sterile towel clip to the medial clavicle percutaneously, and apply direct anterior traction to lift the clavicle out of the mediastinum.
4. Reduction is often accompanied by a palpable and audible clunk. Post-reduction stability is assessed; most posterior dislocations are stable once reduced due to the intact anterior capsule.
Complications and Management
Surgical intervention at the sternoclavicular joint carries a unique and potentially catastrophic complication profile compared to other orthopedic procedures. The proximity of the great vessels, pleura, and trachea mandates meticulous surgical technique and a deep understanding of retrosternal anatomy.

Intraoperative vascular injury is the most feared complication. Aberrant drill penetration, aggressive retractor placement, or loss of control of a bone fragment can lacerate the brachiocephalic vein or artery. Immediate packing, control of hemorrhage, and emergent thoracic surgical intervention are required. Pneumothorax can occur if the pleural dome is violated during deep dissection or drilling.
Postoperative complications include recurrent instability, which is often the result of inadequate graft tensioning, failure to address costoclavicular ligament insufficiency, or patient non-compliance with postoperative immobilization. Infection, while rare, requires prompt irrigation and débridement, often with removal of the graft material if a reconstruction was performed.
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage Strategies and Management |
|---|---|---|---|
| Vascular Injury | < 1% | Errant drilling; over-penetration of osteotome; chronic posterior dislocation adhering to vessels. | Immediate packing; emergent sternotomy/thoracotomy by thoracic surgeon; vascular repair. |
| Pneumothorax | 1 to 2% | Violation of pleural dome during inferior dissection or drilling. | Intraoperative recognition; chest tube thoracostomy; postoperative radiographic monitoring. |
| Recurrent Instability | 5 to 15% | Graft stretching; failure of fixation; unrecognized costoclavicular ligament disruption. | Revision reconstruction with robust allograft; possible medial clavicle resection if highly symptomatic and unrepairable. |
| Iatrogenic Instability | 10 to 20% (post-excision) | Resection of >1.5 cm of medial clavicle, compromising the costoclavicular ligament. | Soft tissue reconstruction (figure-of-eight graft) to stabilize the remaining clavicle to the first rib or sternum. |
| Infection | 1 to 3% | Prolonged operative time; immunocompromised state; hardware utilization. | Aggressive I&D; removal of non-incorporated graft/hardware; targeted IV antibiotic therapy. |
| Hardware Migration | Variable (Historical) | Use of smooth Kirschner wires or Steinmann pins for SCJ fixation. | ABSOLUTE CONTRAINDICATION. Pins must never be used in the SCJ due to fatal migration into the heart or great vessels. |
Post Operative Rehabilitation Protocols
The success of sternoclavicular joint reconstruction relies heavily on strict adherence to postoperative rehabilitation protocols. The reconstructed ligaments require adequate time for biological incorporation and healing before being subjected to the complex multi-planar forces of the shoulder girdle.
Phase 1 Immediate Postoperative Period (Weeks 0 to 4)
The patient is immobilized in a sling or a figure-of-eight brace immediately following surgery. Immobilization is strictly maintained for 4 to 6 weeks. Cryotherapy is utilized for edema and pain control. Elbow, wrist, and hand active range of motion is encouraged to prevent distal stiffness. Shoulder motion is strictly limited to pendulum exercises and passive forward flexion up to 90 degrees. Abduction and extension are explicitly prohibited to prevent stress on the anterior reconstruction.
Phase 2 Intermediate Rehabilitation (Weeks 4 to 8)
The sling is gradually weaned. Active-assisted and active range of motion exercises are initiated in all planes. Scapular stabilization exercises (rhomboids, trapezius, serratus anterior) are introduced to ensure proper scapulothoracic kinematics, which unloads the sternoclavicular joint. Isotonic strengthening of the deltoid and rotator cuff begins, utilizing low resistance and high repetitions.
Phase 3 Advanced Strengthening (Weeks 8 to 12)
Progressive resistance exercises are incorporated. Patients may begin closed kinetic chain exercises. Range of motion should be symmetric to the contralateral side by the end of this phase.
Phase 4 Return to Activity (Months 3 to 6)
Heavy lifting, contact sports, and manual labor are restricted until at least 4 to 6 months postoperatively. Return to play criteria include full, painless range of motion, normal scapulothoracic rhythm, and symmetric strength on isokinetic testing.
Summary of Key Literature and Guidelines
The academic consensus regarding the management of medial clavicle pathology and sternoclavicular joint instability has evolved significantly, driven by advancements in biomechanical understanding and advanced imaging.
Historically, the use of transarticular Kirschner wires or Steinmann pins was described for stabilizing the sternoclavicular joint. However, classic literature, including comprehensive reviews by Rockwood and Wirth, has definitively condemned this practice. The migration of smooth pins into the mediastinum has resulted in numerous documented fatalities due to cardiac tamponade and great vessel laceration. Consequently, the use of unthreaded transarticular pins is universally considered an absolute contraindication in modern orthopedic surgery.
The biomechanical superiority of the figure-of-eight reconstruction technique was firmly established by Spencer et al., who demonstrated that a robust soft-tissue graft passed through the manubrium and medial clavicle most accurately restores the native kinematics and load-to-failure strength of the intact joint. This has become the gold standard for sternoclavicular reconstruction.
Current clinical guidelines mandate the use of computed tomography for any suspected sternoclavicular dislocation. The literature emphasizes that plain radiography, even with specialized views like the Serendipity view, is insufficient for definitive surgical planning, particularly in differentiating posterior dislocations from medial physeal fractures in patients under 25 years of age. Furthermore, multidisciplinary guidelines strongly recommend the immediate availability of a cardiothoracic surgeon during the open reduction of chronic posterior dislocations, given the high risk of catastrophic hemorrhage from vessels that may have become adherent to the displaced clavicle.
You Might Also Like

