Comprehensive Surgical Management of Extensor Mechanism Injuries
Key Takeaway
Disruption of the knee extensor mechanism requires meticulous surgical intervention to restore biomechanical function. This guide details the operative management of chronic patellar tendinosis, inferior pole stress fractures, and acute patellar tendon ruptures. Key principles include excision of degenerative tissue, rigid internal fixation, and precise restoration of patellar height to prevent patella alta or baja, followed by a phased, evidence-based rehabilitation protocol.
INTRODUCTION TO EXTENSOR MECHANISM PATHOLOGY
The extensor mechanism of the knee—comprising the quadriceps muscle group, quadriceps tendon, patella, patellar retinaculum, patellar tendon, and tibial tubercle—is critical for normal ambulation, deceleration, and dynamic stabilization of the lower extremity. Pathologies affecting this complex range from chronic, overuse-induced degenerative tendinosis to catastrophic acute ruptures.
Surgical management of these conditions requires a profound understanding of knee biomechanics. The extensor mechanism is subjected to tremendous forces, often exceeding seven to eight times body weight during activities such as jumping or deep squatting. Consequently, operative interventions must prioritize rigid biomechanical fixation, precise restoration of anatomical length, and the biological stimulation of healing in hypovascular zones.
REPAIR OF CHRONIC PATELLAR TENDINOSIS
Chronic patellar tendinosis, colloquially known as "jumper’s knee," is a degenerative condition characterized by angiofibroblastic hyperplasia, mucoid degeneration, and a disorganized collagen matrix, predominantly affecting the proximal third of the patellar tendon at its origin on the inferior pole of the patella. When prolonged nonoperative management (eccentric strengthening, shockwave therapy, biologics) fails, surgical debridement and repair are indicated.
Surgical Technique: Open Debridement and Repair
The primary goal of surgery is the excision of the degenerative, non-healing tissue and the stimulation of a robust vascular response to promote the formation of organized type I collagen.
- Approach and Exposure: A longitudinal midline or parapatellar incision is made over the anterior knee, extending from the inferior pole of the patella to the mid-substance of the patellar tendon. The subcutaneous tissues are sharply dissected to expose the peritenon.
- Peritenon Management: The tendon sheath (peritenon) is incised longitudinally. It is critical to handle this tissue meticulously, as it houses the primary vascular supply to the anterior tendon.
- Identification and Excision: Longitudinal incisions are made directly into the tendon substance to expose the central core. The area of degeneration—often appearing as gray, friable, mucoid tissue—is identified and sharply excised.
- Biological Stimulation: The inferior pole of the patella is exposed. To incite a localized healing response and introduce marrow-derived mesenchymal elements into the repair site, the inferior pole is aggressively curetted or drilled using a fine Kirschner wire or high-speed burr.
- Tendon Repair: The resulting defect in the tendon substance is approximated and sutured using side-to-side interrupted 2-0 Vicryl (polyglactin 910) sutures. Care is taken not to over-constrict the tendon, which could alter its biomechanical tracking.
- Closure: The peritenon is meticulously closed over the tendon with interrupted absorbable sutures to prevent adhesion formation and restore the gliding mechanism. The subcutaneous tissue and skin are closed in a routine, layered fashion.
Surgical Pitfall: Failure to adequately close the peritenon can lead to severe postoperative adhesions between the patellar tendon and the subcutaneous tissues, resulting in anterior knee pain and restricted range of motion.
Postoperative Rehabilitation Protocol
Successful outcomes following the repair of chronic patellar tendinosis rely heavily on a structured, phased rehabilitation program.
- Immediate Postoperative Phase (Weeks 0-4): A rigid knee immobilizer or hinged knee brace locked in extension is applied. The patient utilizes crutches for partial weight-bearing. Stage 1 of rehabilitation emphasizes the restoration of passive range of motion (ROM) and the initiation of isometric quadriceps strengthening to prevent profound atrophy.
- Intermediate Phase (Weeks 4-8): Closed-chain kinetic exercises are introduced in Stage 2, provided that postoperative swelling and point tenderness have resolved. Exercises such as shallow leg presses and wall slides are initiated, keeping flexion angles within safe limits to avoid excessive tension on the healing tendon.
- Advanced Phase (Weeks 8-12+): Stage 3 consists of activity-specific exercises. It is imperative to avoid premature eccentric overload, which can disrupt the maturing collagen matrix.
- Return to Play: A return to full, unrestricted athletic activities is permitted only when the patient has achieved 85% to 90% of contralateral limb strength and a full, painless range of motion.
STRESS FRACTURES OF THE INFERIOR PATELLAR POLE
Stress fractures through the inferior pole of the patella represent a severe manifestation of chronic extensor mechanism overload, most frequently observed in elite jumping athletes, such as collegiate basketball players. These fractures often present as non-unions due to the constant distraction forces exerted by the patellar tendon.
Surgical Technique: Internal Fixation and Bone Grafting
Operative intervention is required to achieve rigid stabilization and biological union of the fracture fragments.
- Exposure: A longitudinal midline or curvilinear transverse incision is utilized to adequately expose the inferior pole of the patella and the proximal patellar tendon.
- Debridement: If the fracture is chronic (several weeks old), the fibrous non-union tissue must be meticulously debrided. The sclerotic fracture surfaces are freshened with a curette or burr to expose bleeding, healthy cancellous bone.
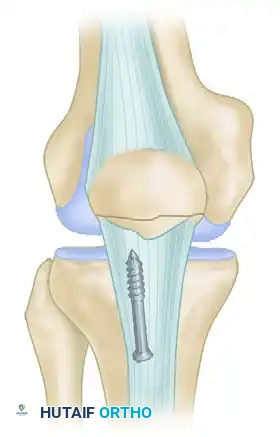
- Internal Fixation: The fracture is reduced and secured using parallel, vertical 4.0 mm partially threaded cancellous screws inserted from distal to proximal through the inferior pole.
- Suture Augmentation: If the bone quality is poor or the fragment is highly comminuted, the fixation can be augmented with heavy nonabsorbable sutures (e.g., No. 5 FiberWire) passed circumferentially through the screw holes or around the screw heads in a tension-band configuration.
- Corticocancellous Slot Graft (Optional but Recommended): To enhance biological healing and provide structural support, an oscillating saw is used to harvest a corticocancellous slot graft (typically 10 mm wide × 15 mm long) from the anterior surface of the proximal patella. This graft is then translated distally across the fracture site.
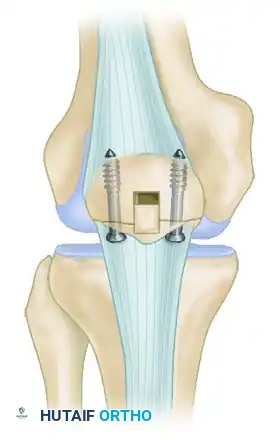


FIGURE 48-28: Stress fracture of the inferior pole of the patella in a collegiate basketball player. The fracture is secured with parallel screws, and a corticocancellous slot graft is placed distally across the fracture site to promote osteosynthesis.
Postoperative Care for Stress Fractures
Following rigid fixation, a cylinder cast or locked hinged knee brace is applied in full extension. The cast is worn continuously for 6 weeks to protect the osteosynthesis. After 6 weeks, clinical and radiographic union is assessed. Once confirmed, active range-of-motion and progressive strengthening exercises are initiated. Return to full athletic activity is usually possible between 10 to 16 weeks, contingent upon complete radiographic healing and functional recovery.
RUPTURE OF THE EXTENSOR MECHANISM OF THE KNEE
Disruption of the extensor mechanism is a profoundly debilitating injury. While fractures of the patella are the most common cause of extensor mechanism failure, soft tissue disruptions—namely, ruptures of the quadriceps tendon and the patellar tendon—are the next most frequent etiologies.
Epidemiology and Mechanism of Injury
The classic mechanism of injury involves a violent, eccentric overload to the extensor mechanism. This typically occurs when the foot is firmly planted, the knee is partially flexed, and the patient's body weight forcefully decelerates, overwhelming the tensile strength of the tendon.
- Patellar Tendon Ruptures: These injuries are predominantly seen in patients younger than 40 years old, particularly in an athletic demographic. The rupture most frequently occurs as an avulsion from the inferior pole of the patella.
- Quadriceps Tendon Ruptures: These are more common in patients older than 40 years. They are highly associated with systemic diseases that compromise collagen integrity and microvascular perfusion. Associated systemic conditions include systemic lupus erythematosus (SLE), diabetes mellitus, gout, hyperparathyroidism, uremia, and morbid obesity.
- Iatrogenic Risk Factors: A well-documented relationship exists between tendon rupture and the prior use of local corticosteroid injections, systemic corticosteroids, or fluoroquinolone antibiotics, all of which can induce rapid collagen necrosis and tendinopathy.
Anatomy and Pathophysiology
It is a widely accepted orthopedic principle that healthy tendons rarely rupture under physiological loads. Numerous studies indicate that degenerative tendinopathy is almost universally present prior to a macroscopic rupture.
Histologic analyses of ruptured quadriceps tendons have demonstrated significant degenerative changes in up to 64% of cases, with the frequency and severity of these changes increasing linearly with patient age. While many patients report a prodromal history of anterior knee pain, athletes occasionally report no antecedent symptoms, indicating a subclinical degenerative process.
Clinical Pearl: Radiographic evaluation of the patellofemoral joint can offer clues to impending rupture. Degenerative spurring at the superior or inferior poles of the patella—often referred to as the "tooth sign" on a tangential (skyline) view—indicates chronic traction tendinopathy and significant structural changes within the quadriceps or patellar mechanism.



FIGURE 48-29: Degenerative spurring (the "tooth sign") visualized on a tangential view of the patella. This radiographic finding is highly indicative of significant, chronic degenerative changes within the quadriceps mechanism.
Clinical Evaluation and Diagnosis
The diagnosis of a disrupted extensor mechanism is primarily clinical, though it can be easily missed or delayed in the acute setting, particularly in patients with large lower extremities or massive hemarthrosis.
Key Clinical Findings:
1. Patient History: Middle-aged or elderly patients presenting with acute swelling, severe pain, and profound dysfunction of the knee following a history of jumping, squatting, or stumbling. Patients frequently report hearing or feeling an audible "pop."
2. Physical Examination:
* A palpable gap or defect is often felt in the quadriceps tendon (superior to the patella) or the patellar tendon (inferior to the patella).
* In quadriceps ruptures, the patella may be displaced inferiorly (patella baja).
* In patellar tendon ruptures, the patella is displaced superiorly (patella alta) due to the unopposed proximal pull of the quadriceps muscle.
* Significant localized swelling and dependent ecchymosis are common.
3. Functional Testing: The hallmark of a complete extensor mechanism disruption is a significant extension lag or the complete inability to perform an active straight-leg raise. It is crucial to note that an intact medial and lateral retinaculum may allow for weak, partial extension, potentially masking a complete central tendon rupture.
Radiographic Evaluation:
Standard anteroposterior (AP) and lateral radiographs are mandatory. A lateral radiograph, particularly with the knee flexed to 30 degrees, is highly sensitive for evaluating patellar height. A superiorly displaced patella (Insall-Salvati ratio > 1.2) confirms a patellar tendon rupture. If the clinical diagnosis remains equivocal due to swelling or patient guarding, ultrasonography or Magnetic Resonance Imaging (MRI) provides definitive visualization of the soft tissue defect.


FIGURE 48-30: Anteroposterior and lateral radiographs demonstrating an acute patellar tendon rupture. Note the significant superior displacement of the patella (patella alta) on the lateral view, caused by the unopposed contraction of the quadriceps muscle.
Surgical Treatment of Acute Patellar Tendon Rupture
Acute ruptures of the patellar tendon should be repaired as expeditiously as possible, ideally within the first 2 weeks post-injury, provided the overlying skin conditions are optimal (absence of severe abrasions or fracture blisters). Delaying surgery leads to severe quadriceps contracture, making anatomical reduction of the patella exceedingly difficult and often necessitating complex reconstructive procedures or V-Y quadricepsplasty.
As previously noted, the rupture most commonly occurs directly at the osteotendinous junction at the inferior pole of the patella. Upon rupture, the patella—acting as a sesamoid bone within the proximal segment of the tendon—may be retracted 3 to 5 cm proximally by the resting tone and contracture of
You Might Also Like
