Recurrent Patellar Dislocations: Comprehensive Surgical Management
Key Takeaway
Recurrent patellar dislocation is a complex orthopaedic pathology driven by incompetence of the medial patellofemoral ligament (MPFL) and underlying anatomical dysplasia. Successful management requires a comprehensive understanding of extensor mechanism biomechanics, precise clinical and radiographic evaluation, and targeted surgical interventions. This guide details the pathophysiology, diagnostic algorithms, and step-by-step surgical techniques—including MPFL reconstruction and tibial tubercle osteotomies—necessary to restore patellofemoral stability and optimize patient outcomes.
Introduction to Recurrent Dislocations
Recurrent dislocations of a joint typically result from one or more traumatic dislocations where subsequent healing of the joint’s supporting capsuloligamentous structures has been deficient. In the context of the knee, recurrent dislocation of the patella can follow a violent initial dislocation, but it occurs far more frequently in knees with one or more underlying anatomical abnormalities that predispose the patellofemoral joint to instability. In these dysplastic knees, only minor trauma or a simple twisting mechanism is required for the initial dislocation to occur.
The underlying pathological condition causes an abnormal excursion of the extensor mechanism over the femoral condyles. To successfully manage this condition, the orthopaedic surgeon must possess a masterful understanding of the static and dynamic stabilizers of the patellofemoral joint, precise clinical and radiographic evaluation techniques, and a mastery of both soft-tissue and bony surgical reconstructions.
Biomechanics and Functional Anatomy
Several anatomical factors must be meticulously evaluated when assessing a patient with recurrent patellar dislocation. The stability of the patella within the trochlear groove relies on a delicate interplay between dynamic muscle forces and static ligamentous and osseous restraints.
Dynamic Stabilizers
Anatomical studies by Lieb and Berry have elucidated the specific contributions of the various portions of the quadriceps muscle to knee extension and patellar tracking.
* Vastus Lateralis (VL): Pulls laterally to the frontal plane of the femur at an angle of 7 to 10 degrees.
* Vastus Medialis Longus (VML): Muscle fibers pull at 15 to 18 degrees medially.
* Vastus Medialis Obliquus (VMO): Muscle fibers pull at a relatively horizontal 50 to 55 degrees medially.
Clinical Pearl: The primary function of the vastus medialis obliquus (VMO) is not knee extension, but rather to stabilize the patella against the lateral pull of the vastus lateralis. This makes the VMO the critical dynamic stabilizer of the patella.
Static Stabilizers
Static factors, which act as the primary structural stabilizers of the patella, include:
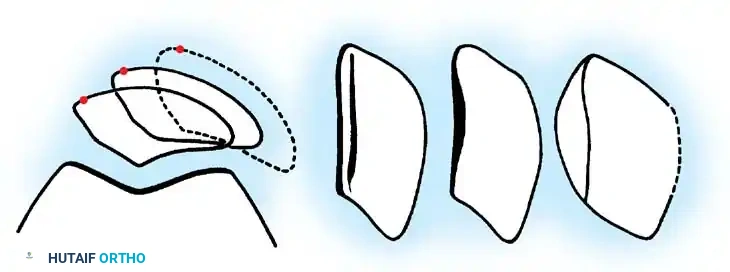
1. The osseous shape of the patella.
2. The depth and contour of the femoral sulcus (trochlea).
3. A patellar tendon of appropriate length (preventing patella alta).
4. A normally tensioned medial capsule reinforced by the patellofemoral and patellotibial ligaments.
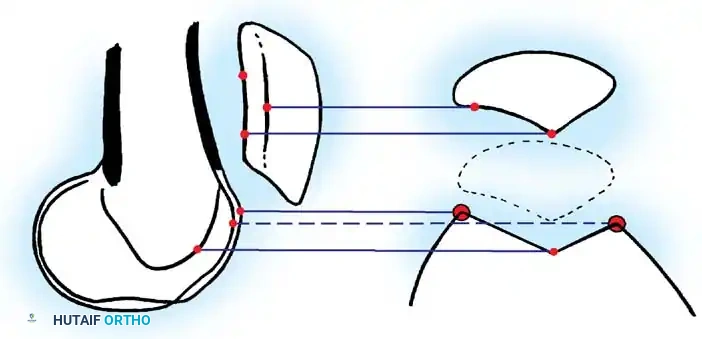
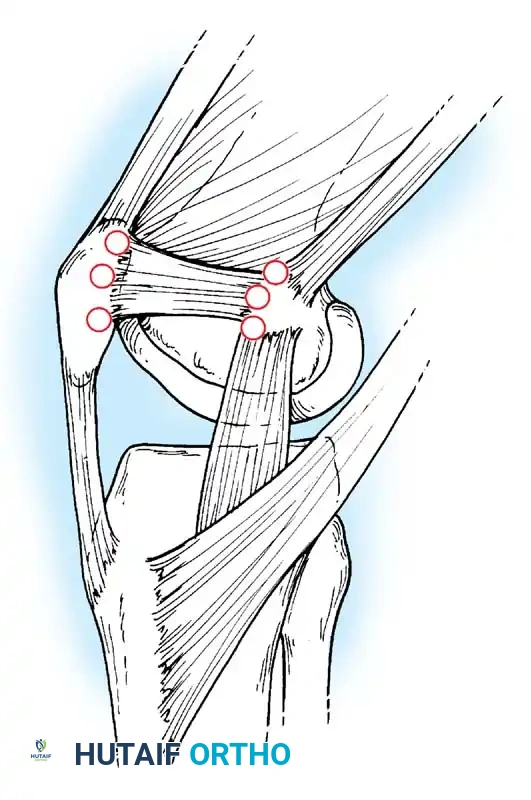
The single most important soft-tissue factor preventing recurrent lateral patellar dislocation is the Medial Patellofemoral Ligament (MPFL). The MPFL is an extrasynovial ligament, located in layer 2 of the medial knee, much like the superficial medial collateral ligament. It provides approximately 60% of the restraining force against lateral patellar displacement from 0 to 30 degrees of knee flexion. Injury to the MPFL may result in minimal long-term damage if healed anatomically, but frequently results in mild-to-moderate laxity, or complete incompetence from femoral avulsion or mid-substance failure, leading to recurrent instability.
Pathophysiology and Predisposing Factors
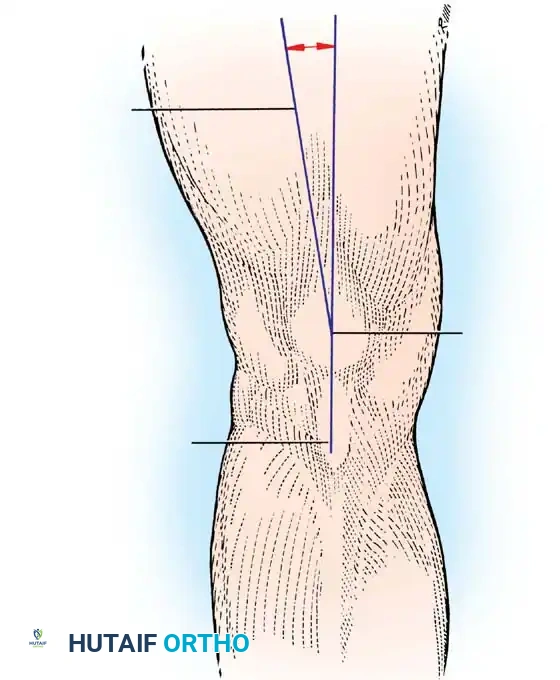
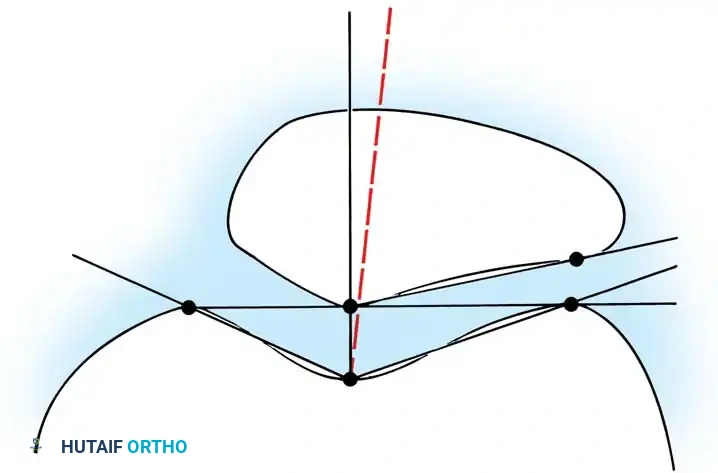
Static and dynamic forces naturally tend to displace the patella laterally during knee extension. Brattström first described the Q angle as the angle formed by the line of pull of the quadriceps mechanism and that of the patellar tendon as they intersect at the center of the patella.
Clinically, this angle is represented by the intersection of a line drawn from the anterior superior iliac spine (ASIS) to the center of the patella, with a second line drawn from the center of the tibial tuberosity to the center of the patella. For this measurement to be accurate, the patella must be centered on the trochlea by flexing the knee to 30 degrees.
* Normal Q Angle (Males): 8 to 10 degrees.
* Normal Q Angle (Females): 15 degrees ± 5 degrees.
This physiologic valgus angle imparts a lateral force vector to the patellofemoral joint as the knee extends. Factors that pathologically increase this Q angle include:
* Genu valgum
* Increased femoral anteversion
* External tibial torsion
* A laterally positioned tibial tuberosity (increased TT-TG distance)
* A tight lateral retinaculum
The Q angle can also be increased dynamically by internally rotating the femur on a fixed tibia, such as during a athletic "cutting" maneuver.
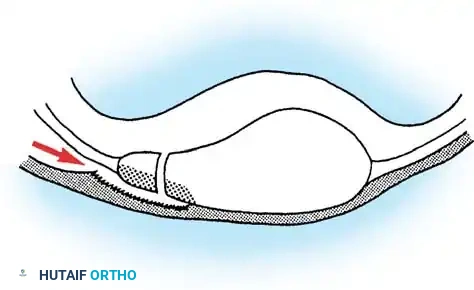
Furthermore, an abnormally small or dysplastic patella can interfere with smooth gliding motion. A high-riding patella (patella alta) is considered by many authors to be the most common anatomical cause of recurrent dislocation, as the patella fails to engage the stabilizing bony confines of the trochlea during early flexion. Dysplasia of the femoral condyles, particularly a hypoplastic lateral femoral condyle, removes the critical bony buttress that prevents lateral subluxation.
Clinical Evaluation
History
In patients with recurrent dislocation or subluxation, an accurate history remains one of the most vital diagnostic tools, as patellar instability can mimic various other "internal derangements" of the knee (e.g., meniscal tears, ACL injuries).
Patients frequently report diffuse anterior knee pain aggravated by ascending or descending stairs. The pain is often described as a dull ache punctuated by intermittent episodes of sharp, severe pain. A profound feeling of insecurity, "giving way," or the knee "going out" is a hallmark symptom.
Physical Examination
The examination begins with the patient seated. Observe the patellar height; an upward tilt ("camel back" sign) indicates patella alta.
Dynamic Tracking: Evaluate tracking by having the seated patient slowly extend the knee. A positive J sign—a sudden lateral subluxation of the patella as the knee approaches terminal extension—indicates severe maltracking and loss of early trochlear engagement.
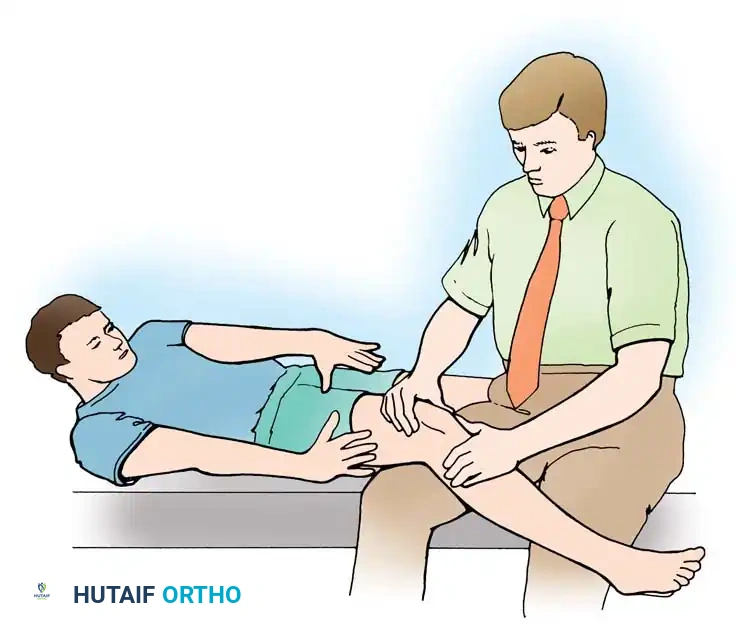
Ligamentous Testing: With the patient supine and the knee flexed 30 degrees over a bolster, measure the Q angle. Insufficiency of the MPFL is tested by applying an inferolaterally directed stress.
Apprehension Test: The examiner holds the relaxed knee in 20 to 30 degrees of flexion and manually subluxes the patella laterally. A positive test occurs when the patient suddenly complains of pain, exhibits quadriceps guarding, and physically resists further lateral motion.
Passive Patellar Glide: Visually divide the patella into four longitudinal quadrants. Passively move the patella medially and laterally at 0 and 20 degrees of flexion. Normal passive glide is 1 to 2 quadrants. Glide of 3 or more quadrants laterally indicates MPFL incompetence. Limited medial glide (<1 quadrant) indicates excessive lateral retinacular tightness.
Patellar Tilt Test: Performed with the knee in full extension. Place fingers along the medial patella and the thumb on the lateral aspect. Inability to elevate the lateral facet to the horizontal plane indicates a pathologically tight lateral retinaculum.
Surgical Warning: Always assess for generalized ligamentous laxity (Beighton score). Patients with connective tissue hyperlaxity (hyperextension of knees/elbows >10 degrees, thumb to forearm, etc.) have higher failure rates with isolated soft-tissue reconstructions and require careful surgical planning.
Radiographic Evaluation
A comprehensive radiographic series is mandatory for surgical planning.
Anteroposterior (AP) View
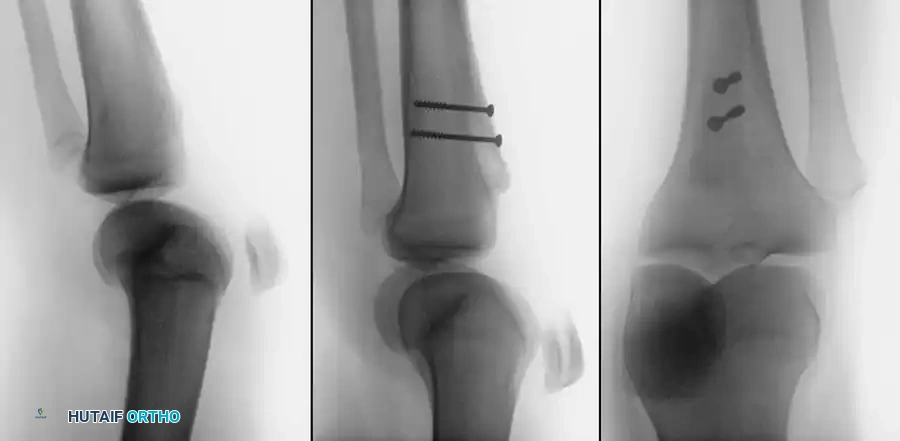
Rarely provides direct information regarding patellofemoral tracking but is essential to rule out bipartite patella (a normal variant) or osteochondral fractures of the medial patellar facet or lateral femoral condyle, which frequently occur during dislocation or relocation.
Lateral View
Crucial for determining patellar height (patella alta or infera).
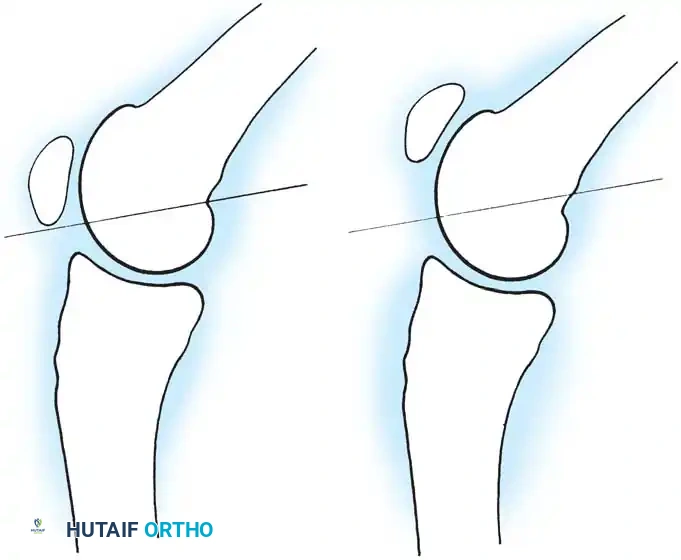
* Blumensaat Line: With the knee flexed 30 degrees, a line extending through the intercondylar notch should intersect the lower pole of the patella. If the patella is proximal to this line, patella alta is present.
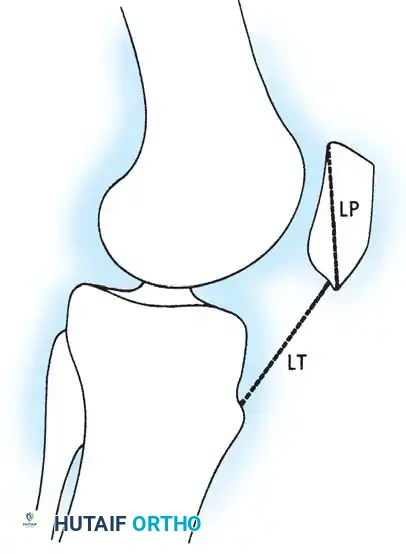
- Insall-Salvati Ratio: The ratio of the length of the patellar tendon (LT) to the diagonal length of the patella (LP). A normal ratio is 1.0. A ratio ≥ 1.2 indicates patella alta.
- Dejour Trochlear Depth: Measured on a true lateral radiograph at 20 degrees of flexion. The trochlear depth measured 1 cm from the top of the groove should be ≥ 5 mm. A crossing sign indicates trochlear dysplasia.
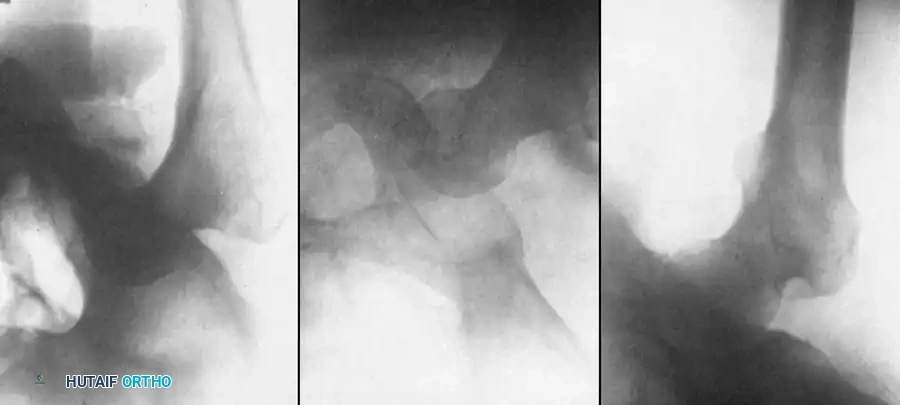
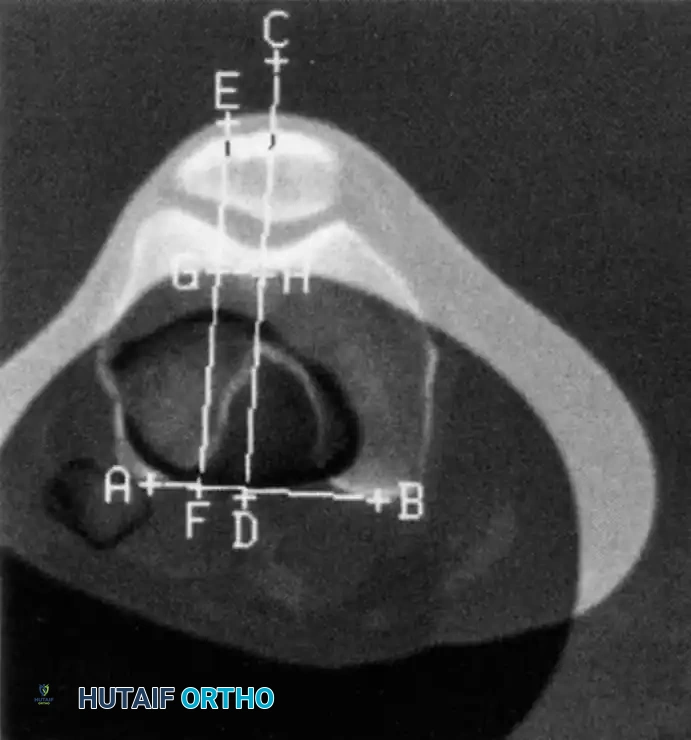
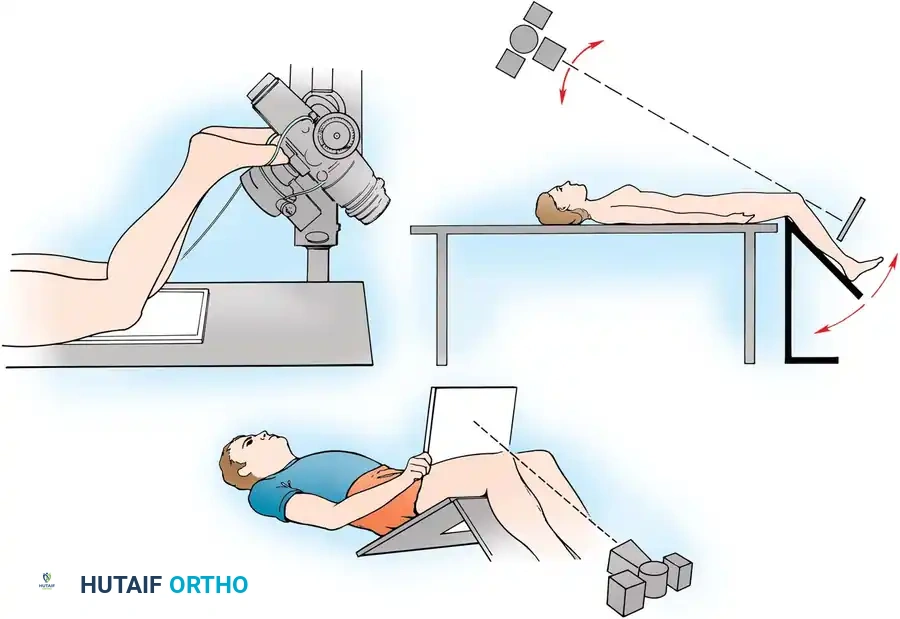
Axial (Merchant/Sunrise) Views
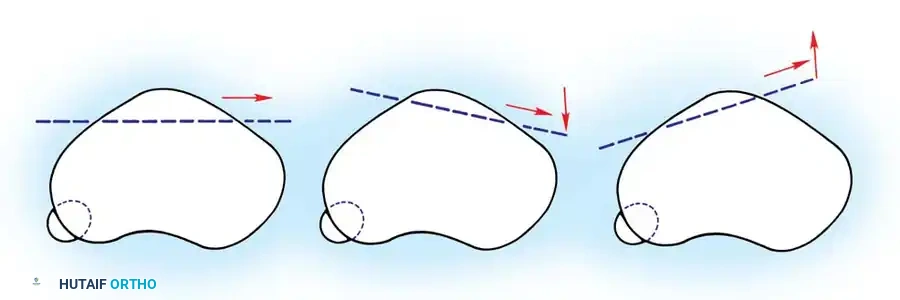
Used to evaluate trochlear morphology, patellar tilt, and subluxation. Maldague and Malghem described progressive lateral patellar tilt where the median ridge of the patella superimposes on, or moves posterior to, the lateral facet.
Magnetic Resonance Imaging (MRI)
MRI is the gold standard for evaluating the site and extent of MPFL injury (typically avulsed from the femoral origin at Schöttle's point) and for identifying radiographically occult osteochondral lesions. It is also utilized to measure the Tibial Tubercle-Trochlear Groove (TT-TG) distance. A TT-TG distance > 20 mm is highly pathologic and typically necessitates a bony realignment procedure.
Surgical Treatment
Surgical intervention is indicated for recurrent dislocations that have failed conservative management (physiotherapy focusing on VMO strengthening and core stability), or in acute settings where a large osteochondral fracture requires fixation or removal.
Diagnostic Arthroscopy
Every surgical intervention for patellar instability should begin with a thorough diagnostic arthroscopy.
1. Assess the articular cartilage of the patella and trochlea.
2. Identify and remove or fix any loose osteochondral fragments.
3. Evaluate dynamic patellar tracking from the anterolateral portal while ranging the knee.
Lateral Retinacular Release
Historically overutilized, isolated lateral release is rarely indicated for recurrent dislocation, as it does not address the primary pathology (MPFL incompetence) and can lead to medial patellar subluxation. It is now primarily used as an adjunct procedure if the lateral retinaculum remains pathologically tight (negative tilt test) after medial reconstruction.

Medial Patellofemoral Ligament (MPFL) Reconstruction
MPFL reconstruction is the gold standard soft-tissue procedure for recurrent patellar instability in the absence of severe bony malalignment (TT-TG < 20mm, normal patellar height).
Step-by-Step Technique:
1. Graft Harvest: A gracilis or semitendinosus autograft is harvested, or an allograft is prepared. The graft is whipstitched at both ends.
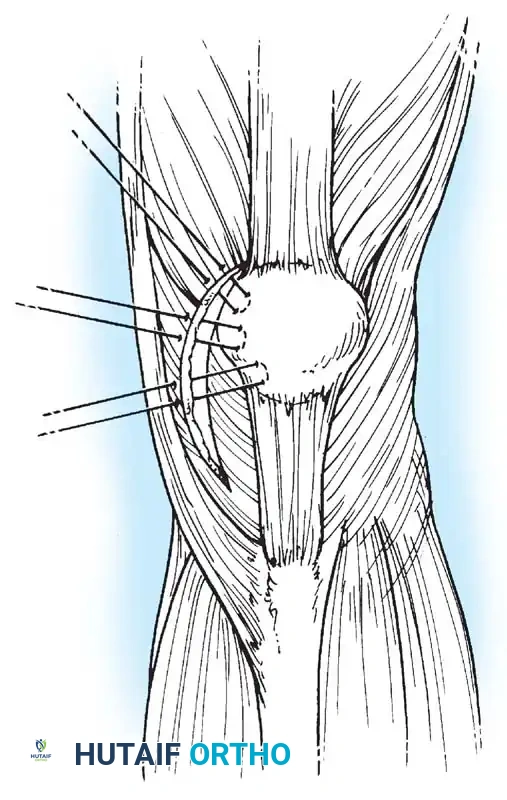
2. Patellar Preparation: A 2-cm incision is made over the medial border of the patella. The upper half of the medial patellar border is exposed. Two transverse drill holes or suture anchors are placed in the proximal half of the patella.
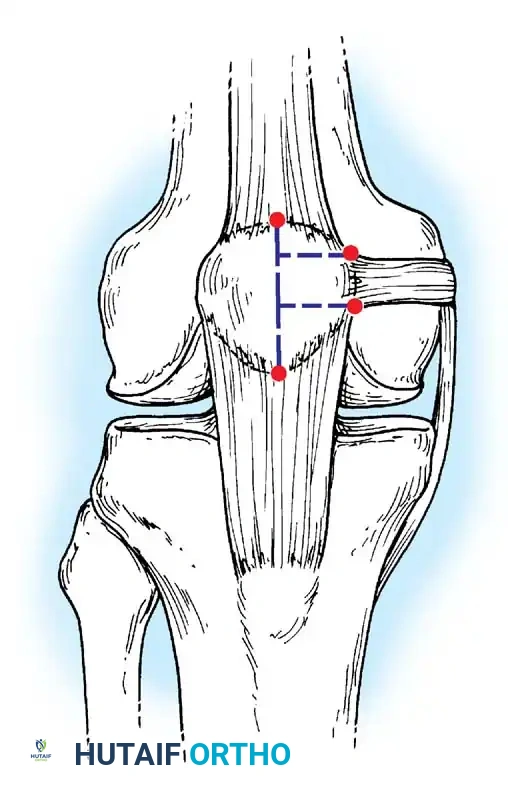
3. Femoral Preparation: The anatomic femoral origin (Schöttle's point) is identified fluoroscopically. This point is located 1 mm anterior to the posterior cortex extension line, 2.5 mm distal to the posterior articular border of the medial femoral condyle, and proximal to the level of the posterior point of Blumensaat's line.
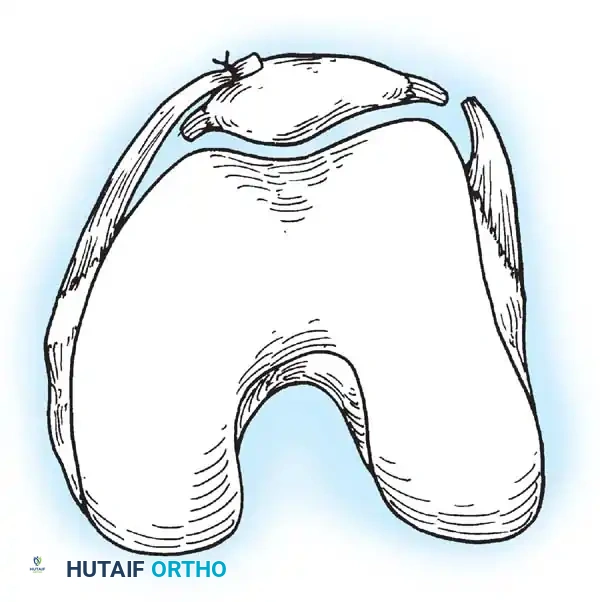
4. Graft Passage: The graft is passed through layer 2 of the medial retinaculum, remaining extrasynovial, from the patella to the femoral footprint.

📚 Medical References
- recurrent patellar dislocation, Clin Orthop Relat Res 144:27, 1979.
- Cosgarea AJ, Schatzke MD, Seth AK, et al: Biomechanical analysis of fl at and oblique tibial tubercle osteotomy for recurrent patellar instability, Am J Sports Med 27:507, 1999.
- Cox JS: An evaluation of the Elmslie-Trillat procedure for management of patellar dislocations and subluxations: a preliminary report, Am J Sports Med 4:72, 1976.
- Cox JS: Evaluation of the Roux-Elmslie-Trillat procedure for knee extensor realignment, Am J Sports Med 10:303, 1982.
- Dandy DJ, Griffi th SD: Lateral release for recurrent dislocation of the patella, J Bone Joint Surg 71B:121, 1989.
- Davis DK, Fithian DC: Techniques of medial retinacular repair and reconstruction, Clin Orthop Relat Res 402:38, 2002.
- Deie M, Ochi M, Sumen Y, et al: Reconstruction of the medial patellofemoral ligament for the treatment of habitual or recurrent dislocations of the patella in children, J Bone Joint Surg 85B:887, 2003.
- Deie M, Ochi M, Sumen Y, et al: A long-term follow-up study after medial patellofemoral ligament reconstruction using the transferred semitendinosus tendon for patellar dislocation, Knee Surg Sports Traumatol Arthrosc 13:522, 2005.
- Drez D Jr, Edwards TB, Williams CS: Results of medial patellofemoral ligament reconstruction in the treatment of patellar dislocation, Arthroscopy 17:298, 2001.
- Ferguson RB, Brown TD, Fu FH, et al: Relief of patellofemoral contact stress by anterior displacement of the tibial tubercle, J Bone Joint Surg 61A:159, 1979.
- Fithian DC, Meier SW: The case for advancement and repair of the medial patellofemoral ligament in patients with recurrent patellar instability, Oper Tech Sports Med 7:81, 1999.
- Floyd A, Phillips P, Khan MRH, et al: Recurrent dislocation of the patella: histochemical and electromyographic evidence of primary muscle pathology, J Bone Joint Surg 69B:790, 1987.
- Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment, Clin Orthop Relat Res 177:176, 1983.
- [
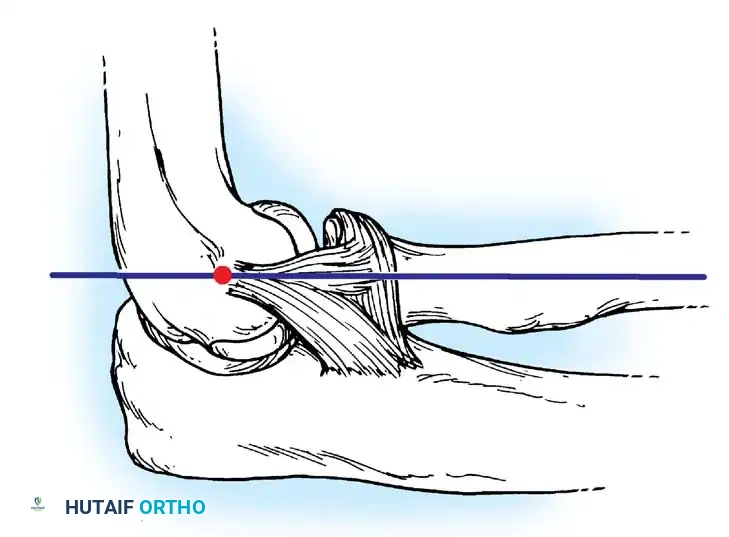
Lateral collateral ligament
Annular ligament
Conjoined insertion
Fig. 45-70 Lateral collateral and annular ligament complex of elbow. Lateral collateral ligament originates off humerus at axis point of ulnohumeral joint, which lies at intersection of anterior humeral line and radiocapitellar axis. Radial collateral ligament blends with annular ligament to insert in conjoined fashion onto proximal ulna. (Redrawn from Cohen MS, Bruno RJ: The collateral ligaments of the elbow, Clin Orthop Relat Res 383:123, 2001.)
Fulkerson JP: Patellofemoral pain disorders: evaluation and management, J Am Acad Orthop Surg 2:124, 1994.](https://pubmed.ncbi.nlm.nih.gov/?term=%21%5BLateral%20collateral%20ligament%5D%28/media/hutaifortho/hutaifortho-references-p2738-c00f56.webp%29%0A%0A%2ALateral%20collateral%20ligament%2A%0A%0AAnnular%20ligament%0A%0AConjoined%20insertion%0A%0AFig.%2045-70%20Lateral%20collateral%20and%20annular%20ligament%20complex%20of%20elbow.%20Lateral%20collateral%20ligament%20originates%20off%20humerus%20at%20axis%20point%20of%20ulnohumeral%20joint%2C%20which%20lies%20at%20intersection%20of%20anterior%20humeral%20line%20and%20radiocapitellar%20axis.%20Radial%20collateral%20ligament%20blends%20with%20annular%20ligament%20to%20insert%20in%20conjoined%20fashion%20onto%20proximal%20ulna.%20%28Redrawn%20from%20Cohen%20MS%2C%20Bruno%20RJ%3A%20The%20collateral%20ligaments%20of%20the%20elbow%2C%20Clin%20Orthop%20Relat%20Res%20383%3A123%2C%202001.%29%0A%0AFulkerson%20JP%3A%20Patellofemoral%20pain%20disorders%3A%20evaluation%20and%20management%2C%20J%20Am%20Acad%20Orthop%20Surg%202%3A124%2C%201994.)
- Fulkerson JP, Becker GJ, Meaney JA, et al: Anteromedial tibial tubercle transfer without bone graft, Am J Sports Med 18:490, 1990.
- Fulkerson JP, Schutzer SF: After failure of conservative treatment for painful patellofemoral malalignment: lateral release or realignment? Orthop Clin North Am 17:283, 1986.
- Galeazzi R: Nuove applicazion del trapianto muscolare e tendineo (XII Congress Societa Italiana di Ortopedia), Arch Ortop 1922, p 38. Garth WP, DiChristina DG, Holt G: Delayed proximal repair and distal realignment after patellar dislocation, Clin Orthop Relat Res 377:132, 2000.
- Geary M, Schepsis A: Management of fi rst-time patellar dislocations, Orthopedics 27:1058, 2004.
- Goldthwait JE: Slipping or recurrent dislocation of the patella: with the report of eleven cases, Boston Med Surg J 150:169, 1904.
- Grana WA, Hinkley B, Hollingsworth S: Arthroscopic evaluation and treatment of patellar malalignment, Clin Orthop Relat Res 186:122, 1984.
- Grelsamer RP: Current concepts review: patellar malalignment, J Bone Joint Surg 82A:1639, 2000.
- Günal I, Karatosun V: Patellectomy: an overview with reconstructive procedures, Clin Orthop Relat Res 389:74, 2001.
- Harwin SF, Stern RE: Subcutaneous lateral retinacular release for chondromalacia of patellae: a preliminary report, Clin Orthop Relat Res 156:207, 1981.
- Hauser EDW: Total tendon transplant for slipping patella: new operation for recurrent dislocation of the patella, Surg Gynecol Obstet 66:199, 1938.
- Hautamaa PV, Fithian DC, Kaufman KR, et al: Medial soft tissue restraints in lateral patellar instability and repair, Clin Orthop Relat Res 349:174, 1998.
- Haxton HA: The function of the patella and the effects of its excision, Surg Gynecol Obstet 80:389, 1945.
- Ho SSW, Jaureguito JW: Functional anatomy and biomechanics of the patellofemoral joint, Oper Tech Sports Med 2:238, 1994.
- Hughston JC: Reconstruction of the extensor mechanism for subluxating patella, Am J Sports Med 1:6, 1972.
- Hughston JC, Walsh WM: Proximal and distal reconstruction of the extensor mechanism for patellar subluxation, Clin Orthop Relat Res 144:36, 1979.
- Hungerford DS, Barry M: Biomechanics of the patellofemoral joint, Clin Orthop Relat Res 144:9, 1979.
- Inoue M, Shino K, Hirose H, et al: Subluxation of the patella: computed tomography analysis of patellofemoral congruence, J Bone Joint Surg 70A:1331, 1988.
- Insall J: Patella pain: current concepts review, J Bone Joint Surg 64A:147, 1982.
- Insall JN, Falvo KA, Wise DW:
You Might Also Like