Chronic Unreduced Proximal Tibiofibular Joint Dislocations: Comprehensive Surgical Management
Key Takeaway
Chronic unreduced dislocations of the proximal tibiofibular joint are rare, frequently missed injuries that present with lateral knee pain, ankle instability, or peroneal nerve dysfunction. Operative management is indicated for symptomatic patients failing conservative care. Surgical options include proximal fibular resection or anatomic ligamentous reconstruction. Arthrodesis is generally contraindicated due to its disruption of normal fibular rotation during ankle dorsiflexion, which predictably leads to secondary ankle morbidity.
Comprehensive Introduction and Patho-Epidemiology
Posttraumatic, chronic subluxation or unreduced dislocation of the proximal tibiofibular joint (PTFJ) represents a relatively rare but highly debilitating clinical entity within orthopedic surgery. These lesions typically manifest following high-energy trauma, such as motor vehicle collisions, or complex twisting injuries sustained in contact sports, which catastrophically disrupt the anterior and posterior capsular ligaments of the PTFJ. Because the primary focus during the acute phase of trauma is frequently and understandably directed toward more obvious, limb-threatening, or functionally dominant intra-articular knee pathology—such as multiligamentous knee injuries, cruciate ligament tears, or complex tibial plateau fractures—PTFJ dislocations are notoriously underappreciated. Consequently, they are frequently missed during the initial primary and secondary surveys in the emergency department.
When an acute dislocation is left unreduced, the joint inevitably progresses to a state of chronic instability or fixed, unreduced dislocation. This chronicity initiates a complex, deleterious cascade of biomechanical alterations that profoundly affect both the knee and the ankle. The pathophysiology of the chronic state is characterized by dense fibrotic scarring, severe capsular contracture, and progressive degradation of the articular cartilage within the PTFJ. As the normal anatomical footprint of the fibular head is lost, the dynamic stabilizing function of the biceps femoris and the fibular collateral ligament (FCL) is fundamentally altered, leading to secondary posterolateral corner (PLC) insufficiency and a predictable varus or rotatory thrust during the gait cycle.
Epidemiologically, chronic PTFJ dislocations are most frequently observed in young, active males, particularly those involved in high-impact sports such as football, rugby, wrestling, and extreme downhill skiing. The initial mechanism of injury often involves a sudden, violent inversion and plantarflexion of the foot and ankle with simultaneous knee flexion and external rotation of the tibia. According to the foundational classification by Ogden, acute dislocations are categorized into anterolateral, posteromedial, and superior types. Anterolateral dislocations are by far the most common, accounting for nearly 85% of cases, and are the most likely to transition into a chronic, symptomatic state if the initial reduction is missed or inadequately stabilized. Posteromedial dislocations are typically associated with direct trauma to the fibular head and carry a significantly higher risk of concomitant common peroneal nerve injury. Superior dislocations are almost exclusively seen in conjunction with severe distal tibiofibular syndesmotic disruptions or lateral malleolar fractures, emphasizing the structural coupling of the fibula.
The clinical presentation of a chronic, unreduced PTFJ dislocation is highly variable, which further complicates the diagnostic process. While an old, unreduced dislocation may occasionally be entirely asymptomatic, requiring no formal surgical intervention, the vast majority of patients eventually develop profound and debilitating symptoms. Patients typically present with chronic, localized lateral knee pain that is exacerbated by deep flexion, squatting, or pivoting movements. Mechanical symptoms are a hallmark of the condition; patients frequently describe a palpable "clunking," a sensation of "giving way," or a visible snapping of the biceps femoris tendon over the dislocated fibular head during strenuous activities. Furthermore, due to the obligate biomechanical coupling of the proximal and distal tibiofibular joints, patients frequently report insidious onset ankle pain, restricted dorsiflexion, and subjective ankle instability. Neurological deficits, ranging from transient paresthesias in the first web space to profound foot drop, indicate common peroneal nerve dysfunction secondary to chronic traction or compression by fibrotic scar tissue.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the PTFJ anatomy is an absolute prerequisite for any orthopedic surgeon contemplating surgical intervention in this region. The PTFJ is a diarthrodial synovial joint situated between the lateral condyle of the tibia and the head of the fibula. The articular facets exhibit significant morphological variability, which Ogden classically divided into two distinct types: horizontal and oblique. The horizontal type (inclination less than 20 degrees) is generally more stable and allows for greater rotatory movement, whereas the oblique type (inclination greater than 20 degrees) is inherently more susceptible to dislocation due to reduced osseous constraint. The joint capsule is relatively thick anteriorly and is contiguous with the superior tibiofibular joint recess, which communicates with the primary knee joint cavity in approximately 10% to 20% of the adult population.
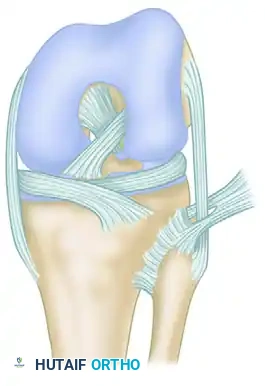
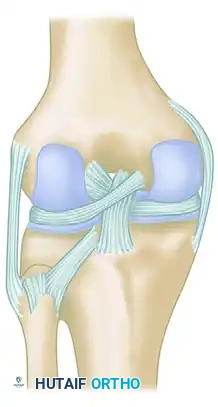
The ligamentous restraints of the PTFJ are robust and function synergistically to resist multiplanar displacing forces. The primary static stabilizers include the anterior superior tibiofibular ligament (ASTFL) and the posterior superior tibiofibular ligament (PSTFL). The ASTFL is composed of two or three broad, flat, and distinct bands that pass obliquely upward from the anterior aspect of the fibular head to insert onto the lateral tibial condyle. It is the primary restraint to anterolateral translation. The PSTFL is a single, thick, and highly robust band passing from the posterior aspect of the fibular head to the posterior aspect of the lateral tibial condyle, deep to the popliteus tendon. It serves as the primary restraint to posteromedial subluxation.
In addition to these static capsuloligamentous structures, the PTFJ is heavily reliant on the dynamic stabilization provided by the posterolateral corner musculotendinous units. The fibular collateral ligament (FCL) and the biceps femoris tendon share a complex, bifurcated insertion footprint on the fibular head. The biceps femoris tendon splits into an anterior and posterior arm, effectively enveloping the FCL insertion. This intimate anatomical relationship dictates that any displacement of the fibular head fundamentally alters the resting tension and dynamic vector of the FCL and biceps femoris, compromising both the lateral knee stability and the PTFJ itself. Furthermore, the common peroneal nerve courses directly posterior to the biceps femoris tendon, wrapping around the fibular neck from posterior to anterior. This precarious anatomical positioning makes the nerve highly vulnerable to traction injuries during dislocation and iatrogenic injury during surgical dissection.
Biomechanically, the fibula is not a static osseous strut; rather, it is a highly dynamic structure that undergoes complex, multiplanar motion during the normal gait cycle. The proximal and distal tibiofibular joints function as a single, linked biomechanical unit. During dorsiflexion of the ankle, the wider anterior portion of the talar dome forcefully engages the ankle mortise. To accommodate this lateral plane rotation and the expansion of the talus, the fibula must translate proximally, move laterally, and, critically, rotate externally around its longitudinal axis. Any surgical procedure that rigidly tethers the proximal fibula to the tibia—such as a PTFJ arthrodesis—will abolish this obligate external rotation. This biomechanical mismatch predictably leads to severe ankle pain, restricted dorsiflexion, and secondary ankle instability, rendering arthrodesis obsolete in modern orthopedic practice.
Exhaustive Indications and Contraindications
The decision-making process for treating chronic unreduced PTFJ dislocations must be highly individualized, driven primarily by the patient's symptomatology, functional demands, and physiological age. The overarching philosophy dictates that asymptomatic chronic dislocations, regardless of the radiographic appearance, should be managed with benign neglect. However, when symptoms become refractory to comprehensive nonoperative modalities—including targeted physical therapy, custom bracing, and activity modification—surgical intervention becomes the standard of care.
Surgical intervention is explicitly indicated in patients presenting with chronic, debilitating lateral knee pain that limits activities of daily living or prevents return to sport. Mechanical symptoms, such as recurrent subluxation, palpable clunking, or an overt sensation of knee instability during pivoting maneuvers, are strong indications for operative management. Furthermore, the presence of progressive neurological deficits, such as common peroneal nerve paresthesias or motor weakness directly attributable to the unreduced fibular head, constitutes an absolute indication for surgical exploration, neurolysis, and joint reconstruction or resection. Finally, patients who exhibit concomitant posterolateral corner insufficiency or distal syndesmotic pain secondary to the proximal anatomical distortion are prime candidates for surgical correction to restore the global biomechanics of the lower extremity.
Contraindications to surgical intervention must be carefully respected to avoid catastrophic postoperative outcomes. Absolute contraindications include active local or systemic infection, severe medical comorbidities precluding safe administration of anesthesia, and an inadequate or compromised soft tissue envelope overlying the lateral aspect of the knee. Relative contraindications include asymptomatic chronic dislocations discovered incidentally on imaging, advanced degenerative joint disease of the ipsilateral lateral knee compartment (which may necessitate a more comprehensive arthroplasty approach), and poorly controlled psychiatric conditions or non-compliance that would preclude adherence to strict postoperative rehabilitation protocols.
The choice between the two primary surgical pathways—proximal fibular resection (fibulectomy) and anatomic ligamentous reconstruction—is nuanced. Resection is generally favored in older, lower-demand patients, or in cases where the articular cartilage of the PTFJ is completely destroyed, provided meticulous attention is paid to reattaching the PLC structures. Conversely, anatomic ligamentous reconstruction is the strongly preferred, joint-preserving option for young, high-demand athletes, adolescents with open physes, and patients in whom preservation of the native PLC biomechanics is paramount. Arthrodesis of the PTFJ is universally contraindicated due to the unacceptable incidence of secondary ankle morbidity.
| Parameter | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Clinical Symptoms | Refractory lateral knee pain, mechanical clunking, giving way. | Asymptomatic incidental finding on radiographs or advanced imaging. |
| Neurological Status | Progressive common peroneal nerve palsy, chronic paresthesias. | Pre-existing, irreversible severe neuropathy unrelated to the PTFJ. |
| Biomechanical Factors | Concomitant PLC instability, secondary distal syndesmotic/ankle pain. | Advanced ipsilateral lateral compartment osteoarthritis (relative). |
| Patient Factors | High-demand athletes, young patients (Reconstruction preferred). | Severe medical comorbidities, active infection, poor soft tissue envelope. |
| Procedure Specific | Resection: Older patients, severe PTFJ arthritis. Recon: Young athletes. | Arthrodesis: Universally contraindicated due to ankle morbidity. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is essential for achieving optimal surgical outcomes in the management of chronic PTFJ dislocations. The clinical evaluation must be exhaustive, encompassing a detailed neurovascular examination of the lower extremity, with specific focus on the motor and sensory distributions of the common peroneal nerve. Special clinical tests, such as the dial test at 30 and 90 degrees of knee flexion, varus stress testing, and the posterolateral drawer test, must be performed to assess the integrity of the posterolateral corner. The distal tibiofibular syndesmosis and ankle joint must also be evaluated for secondary instability or restricted range of motion.
Diagnostic imaging is the cornerstone of surgical templating. Standard orthogonal radiographs (AP and lateral) of the knee, along with comparison views of the contralateral uninjured knee, are mandatory to assess the general osseous alignment and identify any associated fractures. However, plain radiographs are often insufficient for fully characterizing the complex, multiplanar deformity of a chronic dislocation. A high-resolution Computed Tomography (CT) scan with 3D reconstructions is the gold standard for defining the exact position of the fibular head relative to the lateral tibial condyle, assessing the degree of articular cartilage wear, and planning the trajectory for bone tunnels or resection cuts. Magnetic Resonance Imaging (MRI) is indispensable for evaluating the soft tissue envelope, specifically the integrity of the FCL, biceps femoris tendon, popliteus complex, and the exact course of the common peroneal nerve amidst the fibrotic scar tissue.
Once the decision between resection and reconstruction is made, specific surgical templating is performed. For anatomic ligamentous reconstruction, the surgeon must decide on the graft type. An ipsilateral autologous gracilis tendon is the most common choice, offering excellent tensile strength with minimal donor site morbidity. Alternatively, a semitendinosus autograft or an allograft (such as a tibialis anterior tendon) may be utilized if the hamstring tendons are inadequate or previously harvested. The diameter of the anticipated graft dictates the size of the drill bits used for the fibular and tibial bone tunnels, typically ranging from 5.0 mm to 6.0 mm. For fibular resection, the surgeon must plan the exact level of the osteotomy, ensuring sufficient bone is removed to prevent impingement while preserving adequate length for the reattachment of the FCL and biceps femoris.
Patient positioning and anesthesia require careful coordination between the surgical and anesthesia teams. General anesthesia is typically preferred, often supplemented with a regional adductor canal block for postoperative pain control; however, sciatic nerve blocks should be avoided or used with extreme caution, as they mask the ability to monitor common peroneal nerve function postoperatively. The patient is placed in the supine position on a standard radiolucent operating table. A sandbag or gel bump is placed under the ipsilateral hip to internally rotate the leg, bringing the lateral aspect of the knee into optimal view. A sterile pneumatic tourniquet is applied to the proximal thigh. The contralateral leg is well-padded and secured. The surgical leg is prepped and draped in a standard sterile fashion, ensuring that the entire limb from the iliac crest to the toes is accessible, allowing for dynamic assessment of knee and ankle range of motion intraoperatively.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of chronic PTFJ dislocations demands meticulous dissection and a profound respect for the regional anatomy. The two primary definitive procedures—Proximal Fibular Resection and Anatomic Ligamentous Reconstruction—are detailed below.
Proximal Fibular Resection (Fibulectomy)
The goal of proximal fibular resection is to eliminate the painful, chronically dislocated articulation while rigorously reconstructing the posterolateral corner to prevent iatrogenic knee instability.
- Incision and Exposure: A lateral curvilinear incision is utilized. The incision begins approximately 3 cm proximal to the lateral joint line, extends distally directly over the prominent fibular head, and curves gently anteriorly along the border of the peroneal muscle compartment. The subcutaneous tissues are sharply dissected, and hemostasis is meticulously achieved. The deep fascia is incised in line with the skin incision.
- Common Peroneal Nerve Neurolysis: This is the most critical and perilous step of the procedure. The common peroneal nerve must be visually identified before any deep dissection or resection occurs. The nerve is located immediately posterior to the biceps femoris tendon, coursing distally and wrapping around the fibular neck. Using blunt dissecting scissors and loupe magnification, a meticulous neurolysis is performed. The nerve is freed from the dense, chronic scar tissue over a length of 5 to 7 cm. A vessel loop is passed around the nerve to allow for gentle, atraumatic retraction throughout the remainder of the case.
- Soft Tissue Detachment: The insertions of the biceps femoris tendon and the fibular collateral ligament (FCL) on the fibular head are carefully identified. Using a #15 scalpel blade, these structures are sharply detached from the bone as a single contiguous sleeve if possible. The detached ends are immediately secured with heavy, non-absorbable locking sutures (e.g., #2 FiberWire) to facilitate subsequent reattachment.
- Bone Resection: The proximal fibula is skeletonized circumferentially, taking extreme care to protect the retracted peroneal nerve and the anterior tibial vessels. An oscillating saw is used to resect the proximal 1.5 to 2.0 cm of the fibula. The osteotomy cut must be angled obliquely from proximal-lateral to distal-medial. This specific trajectory ensures that no prominent bony spike remains laterally to irritate the skin or the peroneal nerve. The resected fibular head is removed and sent for routine histopathological analysis.
- Ligamentous Reattachment (PLC Reconstruction): Failure to adequately reattach the FCL and biceps femoris will result in catastrophic varus and rotatory knee instability. The lateral aspect of the tibial condyle, just distal to the articular margin, is decorticated with a high-speed burr to create a bleeding bone bed. Two double-loaded suture anchors (4.5 mm or 5.5 mm) are placed into the prepared tibial footprint. Alternatively, a transosseous bone tunnel technique can be employed. The previously tagged FCL and biceps femoris are advanced to the tibia and tied down securely while the knee is held in 30 degrees of flexion and neutral rotation, applying a valgus force to tension the lateral structures appropriately.
- Closure: The surgical field is thoroughly irrigated. The deep fascial layers are closed loosely to prevent any potential compartment syndrome or compression on the transposed common peroneal nerve. The subcutaneous tissue and skin are closed in a standard layered fashion.
Anatomic Ligamentous Reconstruction
For younger, high-demand patients, anatomic reconstruction utilizing an autograft aims to restore the native stability of the PTFJ while preserving the osseous anatomy and PLC biomechanics.
- Graft Harvest and Preparation: A standard 3 cm longitudinal incision is made over the ipsilateral pes anserinus. The gracilis tendon is identified, isolated, and harvested using an open-ended tendon stripper. The graft is taken to the back table, cleared of muscle belly, and whipstitched at both ends with #2 non-absorbable sutures. The graft is typically sized to 5.0 mm or 5.5 mm in diameter.
- Approach and Joint Debridement: A lateral approach to the PTFJ is performed as described above. The common peroneal nerve is identified, neurolysed, and protected with a vessel loop. The chronically dislocated PTFJ is exposed. A combination of sharp dissection and a mechanical shaver is used to aggressively debride the dense fibrotic scar tissue and capsular remnants from the joint space, mobilizing the fibular head.
- Reduction and Temporary Fixation: The fibular head is manually reduced into its anatomic position on the lateral tibial condyle. Because the joint has been chronically dislocated, it lacks inherent stability even when reduced. Therefore, temporary rigid fixation is mandatory. A 3.2 mm drill bit is used to drill a path from the lateral aspect of the fibula, across the PTFJ, and into the tibia, parallel to the joint line. A 4.5 mm fully threaded cortical screw is placed in a syndesmotic fashion to rigidly hold the reduction. Crucially, this screw is temporary and must be removed postoperatively to restore fibular rotation.
- Tunnel Preparation: With the joint reduced and secured, bone tunnels are created to mimic the native ligamentous footprints. A 5.0 mm or 5.5 mm drill bit (matching the graft size) is used to create an anterior-to-posterior tunnel through the fibular head. A corresponding anterior-to-posterior tunnel is drilled through the lateral tibial condyle, positioned slightly proximal and medial to the fibular tunnel to recreate the trajectory of the ASTFL and PSTFL.
- Graft Passage and Fixation: The prepared gracilis graft is passed through the fibular tunnel from anterior to posterior. The posterior limb of the graft is then routed anteriorly through the tibial tunnel, creating a figure-of-eight configuration that crosses over the joint line. This construct anatomically reconstructs both the anterior and posterior superior tibiofibular ligaments. The graft is tensioned manually with the ankle held in neutral dorsiflexion. Fixation is achieved using bioabsorbable or PEEK interference screws (typically one size larger than the tunnel diameter) placed into both the fibular and tibial tunnels. Alternatively, suspensory cortical buttons can be utilized.
- Closure: The wound is irrigated, and a layered closure is performed, again ensuring no tension is placed over the common peroneal nerve.
Complications, Incidence Rates, and Salvage Management
Surgeons undertaking the management of chronic PTFJ dislocations must be acutely aware of the significant complication profile associated with this anatomical region. The lateral aspect of the knee is unforgiving, and technical errors can lead to devastating functional consequences.
The most feared complication is Common Peroneal Nerve Palsy. The incidence of transient neuropraxia following lateral knee surgery ranges from 2% to 5%, but in the context of chronic PTFJ dislocations with extensive scarring, the risk is markedly elevated. Injury can occur via direct iatrogenic laceration during dissection, thermal necrosis from electrocautery, traction neuropraxia during aggressive retraction or fibular reduction, or postoperative compression from a developing hematoma. Prevention relies entirely on meticulous, early identification and neurolysis of the nerve. If a complete transection is recognized intraoperatively, immediate primary microsurgical epineural repair or cable grafting is mandated. If a palsy is noted postoperatively, immediate removal of compressive dressings is required, followed by serial EMG studies at 6 weeks. Salvage management for permanent palsy involves a posterior tibial tendon transfer to restore active dorsiflexion.
Posterolateral Corner (PLC) Instability is a catastrophic complication primarily associated with proximal fibular resection. If the FCL and biceps femoris are inadequately reattached to the tibia, or if the fixation fails, the patient will develop profound varus and rotatory instability, leading to a debilitating varus thrust during ambulation. The incidence of this complication is directly inversely proportional to the surgeon's attention to detail during the reattachment phase. Avoidance involves using robust fixation methods (double-loaded anchors or transosseous tunnels) and strict adherence to postoperative bracing protocols. Salvage management requires a complex, formal PLC reconstruction using allograft tissue (e.g., Achilles or split Achilles allograft) routed through new tibial and femoral tunnels.
Ankle Morbidity and Syndesmotic Widening represent another significant cluster of complications. As previously emphasized, arthrodesis of the PTFJ abolishes the obligate external rotation of the fibula, leading to an incidence of secondary ankle pain approaching 75% in historical series. Furthermore, in the context of ligamentous reconstruction, failure to remove the temporary trans-articular syndesmotic screw at the appropriate time (3 to 6 months) will result in identical biomechanical tethering, hardware breakage, and ankle morbidity. Avoidance requires strict adherence to the planned secondary hardware removal procedure. Salvage for a painful PTFJ arthrodesis involves a takedown of the fusion mass and a secondary proximal fibular resection to restore the independent motion of the distal fibula.
Recurrent Instability of the PTFJ can occur following ligamentous reconstruction. This typically results from graft elongation, premature removal of the temporary syndesmotic screw before biologic graft incorporation has occurred, or failure to address concomitant PLC injuries. The incidence is estimated at 5% to 10% in high-demand populations. Avoidance entails robust graft tensioning, secure interference screw fixation, and maintaining the temporary syndesmotic screw for a minimum of 12 weeks. Salvage for a failed reconstruction usually necessitates a conversion to a proximal fibular resection.
| Complication | Estimated Incidence | Mechanism / Risk Factor | Avoidance Strategy | Salvage Management |
|---|---|---|---|---|
| Common Peroneal Nerve Palsy | 5% - 15% | Traction, direct laceration, hematoma compression. | Early identification, meticulous neurolysis, gentle retraction. | Acute repair, AFO bracing, delayed tendon transfer. |
| PLC Instability | 2% - 8% | Failure of FCL/Biceps reattachment post-resection. | Robust anchor/tunnel fixation, proper tensioning in 30° flexion. | Formal allograft PLC reconstruction. |
| Ankle Morbidity | >70% (if fused) | Loss of obligate fibular rotation (Arthrodesis/retained screw). | Avoid arthrodesis; mandate removal of temporary screw at 3-6 mos. | Takedown of fusion, conversion to fibular resection. |
| Recurrent PTFJ Instability | 5% - 10% | Graft stretch, premature screw removal, missed PLC injury. | Figure-of-eight graft routing, maintain screw for 12+ weeks. | Revision reconstruction or conversion to fibular resection. |
| Hardware Irritation | 10% - 20% | Prominent screw heads, lateral fibular spike post-resection. | Oblique fibular osteotomy cut, countersink hardware. | Hardware removal after complete healing. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must be meticulously tailored to the specific surgical procedure performed, as the biomechanical goals and tissue healing timelines differ significantly between fibular resection and ligamentous reconstruction. Communication between the orthopedic surgeon and the physical therapy team is paramount to ensure that the reconstructed tissues are protected while preventing debilitating joint stiffness.
Rehabilitation Following Proximal Fibular Resection
The primary goal following a fibulectomy is to protect the crucial soft tissue reattachment of the FCL and biceps femoris to the lateral tibia while allowing for early mobilization of the knee joint.
- Phase 1: Maximum Protection (0 to 2 weeks): Immediately postoperatively, the patient is placed in a hinged knee brace locked in full extension. Weight-bearing is permitted as tolerated with the use of crutches, as axial loading in full extension does not place significant stress on the lateral structures. The primary focus during this phase is wound healing, strict edema control, and the prevention of deep vein thrombosis. Active ankle pumps are encouraged to promote venous return and maintain distal mobility.
- Phase 2: Controlled Mobilization (2 to 6 weeks): The hinged knee brace is unlocked to allow progressive passive and active-assisted range of motion (ROM). The goal is to achieve 0 to 90 degrees of flexion by the end of week 4, and full ROM by week 6. Crucial Restriction: Isolated, active hamstring curls (specifically targeting the biceps femoris) are strictly prohibited during this phase to prevent avulsion of the healing tendon from its new tibial footprint. Quadriceps isometric exercises and straight leg raises in the brace are initiated.
- Phase 3: Strengthening and Return to Function (6 to 12 weeks): The knee brace is gradually weaned and discontinued. Progressive resistance exercises for the quadriceps, hamstrings, and hip abductors are initiated. Closed kinetic chain exercises (e.g., leg presses, shallow squats) are emphasized to promote dynamic joint stability.
- Phase 4: Advanced Activity (12+ weeks): Patients may begin a structured return-to-run program, starting with light jogging on a treadmill. Plyometric training and sport-specific agility drills are introduced. Full return to contact sports is typically permitted between 4 and 6 months, contingent upon the restoration of symmetrical muscle strength and the absence of any dynamic varus thrust.
Rehabilitation Following Ligamentous Reconstruction
The rehabilitation following an anatomic reconstruction is inherently more conservative in the early phases due to the presence of the temporary trans-articular syndesmotic screw and the need for biologic incorporation of the tendon graft within the bone tunnels.
- Phase 1: Strict Protection (0 to 6 weeks): The patient is placed in a hinged knee brace locked in full extension. Weight-bearing is strictly limited to non-weight-bearing or touch-down weight-bearing (toe-touch only) with bilateral crutches. This restriction is critical to prevent cyclical loading and subsequent breakage of the temporary syndesmotic screw. Passive ROM is permitted from 0 to 90 degrees, but active knee flexion is avoided to protect the graft.
- Phase 2: Progressive Weight-Bearing (6 to 12 weeks): The patient is allowed to gradually progress to full weight-bearing as tolerated, still utilizing the hinged brace for mediolateral support. Active ROM exercises are initiated, aiming for full, symmetrical knee flexion and extension. Light, closed kinetic chain strengthening begins.
- Hardware Removal (3 to 6 months): This is a mandatory, planned secondary intervention. Between 12 and 24 weeks postoperatively, the patient is taken back to the operating room. Under local anesthesia with sedation, or a brief general anesthetic, a small stab incision is made over the lateral fibula, and the temporary 4.5 mm trans-articular syndesmotic screw is removed. This critical step unlocks the PTFJ, restoring the obligate external rotation of the fibula required for normal ankle biomechanics.
- Phase 3: Advanced Rehabilitation (Post-Screw Removal): Following the removal of the syndesmotic screw, the rehabilitation protocol accelerates rapidly. Advanced proprioceptive training, aggressive plyometrics, and sport-specific cutting and pivoting drills are initiated. The patient is cleared for full, unrestricted return to high-impact sports once functional testing demonstrates >90% limb symmetry index (LSI) compared to the contralateral leg, typically around 6 to 8 months from the index reconstruction.
Summary of Landmark Literature and Clinical Guidelines
The surgical management
