Advanced Operative Management of Recurrent Hip Dislocation and Extensor Mechanism Reconstruction

Key Takeaway
Recurrent hip dislocation without associated fracture is a rare orthopedic challenge often driven by capsular redundancy, labral pathology, or underlying dysplasia. Surgical management requires meticulous preoperative imaging, including CT arthrography, to identify capsular defects. Operative interventions range from soft-tissue plication and modified Bankart-type repairs to structural bone blocks. Concurrently, extensor mechanism deficiencies may necessitate complex reconstructive procedures, such as patellectomy with quadricepsplasty or patellar tendon realignment, to restore joint kinematics and stability.
Recurrent Dislocation of the Hip: Pathoanatomy and Clinical Evaluation
Recurrent dislocation of the hip, particularly in the absence of an associated fracture of the femoral head or the acetabulum, is an exceedingly uncommon clinical entity. The inherent osseous stability of the ball-and-socket joint, combined with the robust static restraints of the iliofemoral, ischiofemoral, and pubofemoral ligaments, makes the hip highly resistant to recurrent instability. Historically, Liebenberg and Dommisse (1969) highlighted the rarity of this condition, documenting instances in only 11 adults and 11 children in their comprehensive review.
When recurrent instability does occur, it is imperative for the orthopedic surgeon to conduct a systematic evaluation to identify the underlying biomechanical or structural failure.
Predisposing Factors to Recurrent Instability
The etiology of recurrent anterior or posterior dislocation of the hip is multifactorial. A thorough preoperative assessment must rule out or confirm the following predisposing factors:
- Acetabular or Femoral Dysplasia: Insufficient femoral head coverage or excessive femoral anteversion significantly reduces the force required for dislocation.
- Occult Acetabular Fracture: Unrecognized shear fractures of the posterior wall can compromise the structural buttress of the joint.
- Joint Infection: Pyogenic arthritis can lead to capsular distension, ligamentous destruction, and subsequent instability.
- Paralytic Conditions: Neuromuscular imbalances (e.g., cerebral palsy, poliomyelitis) alter the dynamic stabilizing forces across the hip joint.
- Generalized Ligamentous Laxity: Particularly prevalent in pediatric populations or patients with connective tissue disorders (e.g., Ehlers-Danlos or Marfan syndrome).
- Congenital Insensitivity to Pain: Lack of protective proprioceptive and nociceptive feedback leads to repetitive microtrauma and eventual joint failure (Charcot arthropathy).
- Massive Soft-Tissue Damage: High-energy trauma resulting in catastrophic failure of the capsule and short external rotators.
- Delayed Reduction of the Initial Dislocation: Prolonged dislocation leads to irreversible stretching and plastic deformation of the capsuloligamentous complex.
- Inadequate Immobilization: Failure to allow sufficient biological healing of the capsule following a primary dislocation event.
SURGICAL PEARL: When recurrent hip dislocations resulting from trauma are surgically explored in the absence of bony injury or underlying dysplasia, the surgeon will almost universally encounter a massive capsular tear. This defect typically features the formation of a large, synovial-lined pouch contiguous with the joint capsule, accompanied by significant tears of the acetabular labrum.
The anatomical location of these labral and capsular tears correlates directly with the direction of instability: anterior tears are pathognomonic for recurrent anterior dislocations, whereas posterior tears are found in recurrent posterior dislocations.
Preoperative Imaging and Diagnostic Arthrography
Standard orthogonal radiography is often insufficient for diagnosing the soft-tissue etiology of recurrent hip instability. Large-volume arthrograms are highly instrumental in the preoperative assessment, allowing the surgeon to visualize capsular redundancy, synovial outpouchings, and labral blunting.
Furthermore, the integration of advanced cross-sectional imaging has revolutionized preoperative planning. Klein et al. demonstrated that combining Computed Tomography (CT) with arthrography provides unparalleled spatial resolution to precisely locate capsular tears and labral avulsions prior to surgical intervention.
Fig. 45-18A: Arthrogram in recurrent posttraumatic hip dislocation. On the anteroposterior view, the contrast material fails to remain contained within the anatomical hip joint. Instead, it pools at the neck region, escaping through a massive capsular rent inferiorly.

Fig. 45-18B: When the head and neck of the femur are rotated for a lateral view, the contrast material is clearly visualized flowing into a large, uncontained synovial sac posteriorly, confirming the loss of capsular integrity.

Fig. 45-18C: Anteroposterior radiograph of the hip following a posterior bone block operation. This procedure was indicated due to a severely deficient and eroded posterior labrum and acetabular lip.
Surgical Interventions for Recurrent Hip Dislocation
The surgical management of recurrent hip dislocation is dictated by the underlying pathoanatomy. Procedures are broadly categorized into bony reconstructions and soft-tissue stabilization techniques.
Bony Reconstruction Procedures
Procedures involving the bony structures are indicated when there is a structural deficiency of the acetabular rim or underlying dysplasia.
* Posterior Bone Block: As reported by Lutter, a posterior bone block harvested from the iliac crest is highly successful in patients presenting with a deficient and eroded posterior labrum. The graft acts as a physical buttress, preventing posterior translation of the femoral head.
* Innominate Osteotomy: In pediatric patients presenting with recurrent anterior dislocation driven by excessive femoral anteversion and acetabular dysplasia, Haddad and Drez successfully utilized a redirectional innominate osteotomy combined with a varus derotational femoral osteotomy to restore concentric joint kinematics.
Soft-Tissue Stabilization Procedures
When the osseous architecture is intact, soft-tissue procedures are employed to eliminate capsular redundancy and reinforce the dynamic stabilizers of the hip.
* Capsular Plication: Involves the aggressive imbrication of the enlarged capsule and the posterior musculature, specifically targeting the quadratus femoris and the gemelli.
* Piriformis Tendon Transfer: For posterior recurrent dislocations, the piriformis tendon can be detached from its insertion and transferred over the posterior capsule. This serves as a dynamic, reinforcing buttress against posterior subluxation.
* Iliopsoas Tendon Transfer: For recurrent anterior dislocations, Dall et al. described transferring the iliopsoas tendon to the greater trochanter. This rerouting transforms the iliopsoas into an anterior buttress and a dynamic internal rotating force, counteracting anterior instability.
TECHNIQUE: Modified Bankart-Type Repair for Recurrent Dislocation of the Hip with Labral Lesion (Lieberman, Altchek, and Salvati)
Lieberman et al. described a highly effective, modified Bankart-type repair utilizing a posterolateral approach. This technique is specifically indicated for patients with posttraumatic recurrent posterior dislocation of the hip driven by capsular redundancy and labral detachment. By combining a capsulorrhaphy with a structural allograft, this procedure restores both the static capsular tension and the osseous buttress of the posterior rim.
Patient Positioning and Surgical Approach
- Positioning: Place the patient in the lateral decubitus position on a radiolucent operating table. Ensure rigid pelvic fixation using anterior and posterior supports. Drape the operative leg free to allow for full intraoperative range of motion and assessment of stability.
- Approach: Utilize a standard posterolateral (Kocher-Langenbeck) approach to the hip. Incise the fascia lata and split the gluteus maximus in line with its fibers. Identify and carefully protect the sciatic nerve throughout the procedure. Tag and reflect the short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus) near their femoral insertions to expose the posterior capsule.
Capsulotomy and Joint Preparation
- T-Plasty Incision: Make a transverse incision in the posterior capsule, oriented perpendicular to the acetabular rim, to create a T-plasty. This allows for excellent visualization of the intra-articular space and the posterior labrum.
- Joint Inspection: Evacuate any intra-articular hematoma or loose bodies. Inspect the femoral head for chondral damage and evaluate the posterior labrum. If a soft-tissue defect is identified as the primary cause of instability, a labral repair and capsulorrhaphy are mandatory to recreate a stable joint. A bone block will be used to supplement this soft-tissue reconstruction.
Osseous Preparation and Suture Placement
- Drill Holes: Identify the posterior acetabular rim. Using a specialized drill guide, create three distinct drill holes along the posterior rim at the 7-o’clock, 9-o’clock, and 11-o’clock positions (referencing a right hip; adjust accordingly for the left).
- Suture Passage: Pass heavy, nonabsorbable sutures (e.g., #2 or #5 FiberWire) through each of the three drill holes.
- Capsular Flap Management: Trim the inferior and superior capsular flaps that were created during the T-plasty. Advance the inferior flap superiorly; this maneuver is critical to eliminate the pathological capsular redundancy.
- Suture Placement in Capsule: Pass the previously placed nonabsorbable sutures through the advanced inferior aspect of the capsule. Do not tie them at this stage.
Bone Grafting and Final Fixation
- Allograft Preparation: Create a bleeding bony trough along the posterior acetabular rim using a high-speed burr or osteotome. Sculpt a structural femoral head allograft to perfectly match the contour of this prepared rim.
- Graft Fixation: Rigidly fix the allograft to the posterior acetabulum using two 6.5-mm cancellous screws equipped with washers to prevent screw head subsidence into the graft.
- Capsulorrhaphy Completion: Complete the soft-tissue repair by tying the previously passed capsular sutures. This action simultaneously tightens the posterior capsule and repairs the labral defect against the newly reconstructed rim.
- Superior Flap Imbrication: Imbricate the superior capsular flap over the newly advanced inferior aspect of the capsule. Achieve this by bringing up the most superior suture and tying it through the superior capsular flap in a horizontal mattress fashion, creating a robust, double-layered capsular repair.
SURGICAL WARNING: Meticulous attention must be paid to the trajectory of the 6.5-mm cancellous screws used for allograft fixation. Errant screw placement can result in intra-articular penetration, leading to catastrophic iatrogenic chondral damage to the femoral head. Intraoperative fluoroscopy is mandatory to confirm extra-articular screw placement.
Postoperative Rehabilitation Protocol
- Adults: Immediate postoperative immobilization in a custom-molded hip abduction brace is required for 6 weeks. The patient is restricted to touch-down weight bearing (TDWB) with bilateral crutches for a total of 12 weeks to ensure adequate incorporation and healing of the structural bone graft. If there are intraoperative concerns regarding the adequacy of fixation, or if patient compliance is questionable, skeletal traction or a rigid hip spica cast may be indicated.
- Children: Immobilization in a well-molded hip spica cast is generally indicated for a minimum of 6 weeks to ensure absolute compliance and protection of the repair.
Adjunctive Lower Extremity Reconstructions: Extensor Mechanism Repair
While the management of recurrent hip dislocation focuses on the proximal joint, comprehensive orthopedic reconstruction often requires addressing concurrent or isolated pathology within the extensor mechanism of the knee. The following techniques detail historical and contemporary approaches to severe patellofemoral dysfunction and medial subluxation.
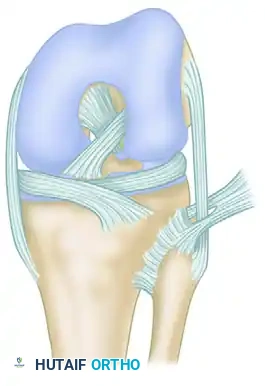
Patellectomy and Quadricepsplasty (West and Soto-Hall Technique)
In cases of severe, unsalvageable patellar comminution or end-stage patellofemoral osteoarthritis where patellectomy is indicated, restoring the mechanical advantage of the extensor mechanism is paramount. The West and Soto-Hall technique provides a robust plastic repair of the quadriceps to minimize extensor lag.
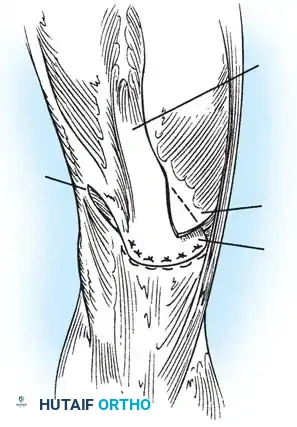
Fig. 45-16A: West and Soto-Hall technique. Following excision of the patella, a lateral release is performed. The vastus medialis is mobilized, and the quadriceps tendon is prepared for advancement over the patellar tendon defect.
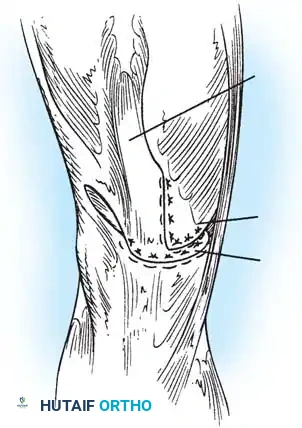
Fig. 45-16B: The quadriceps tendon is drawn distally and sutured directly to the patellar tendon. The vastus medialis is then advanced distally and laterally, imbricating it over the midline repair to centralize the tracking vector and reinforce the extensor mechanism.
Key Surgical Steps:
1. Excision: Carefully enucleate the patella from its tendinous envelope, preserving as much continuous retinacular tissue as possible.
2. Lateral Release: Perform a controlled lateral retinacular release to decompress the lateral compartment and allow for medial mobilization of the extensor mechanism.
3. Tendon Approximation: Draw the central quadriceps tendon distally and suture it securely to the proximal stump of the patellar tendon using heavy, nonabsorbable locking sutures.
4. Vastus Medialis Advancement: Mobilize the vastus medialis obliquus (VMO). Advance it distally and laterally over the primary repair site. This V-Y type advancement not only thickens the repair but restores the dynamic medial stabilizing force lost during patellectomy.
Reconstruction for Medial Subluxation of the Patella (Hughston Technique)
Medial subluxation of the patella is a highly debilitating condition, frequently occurring as an iatrogenic complication following an overzealous lateral retinacular release. Hughston et al. described a reliable reconstructive technique utilizing a strip of the patellar tendon to tether the patella laterally, restoring central tracking.
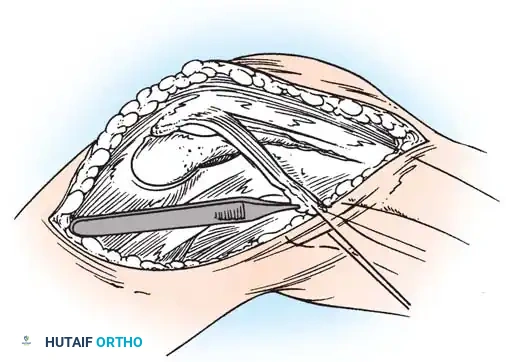
Fig. 45-17A: Hughston Reconstruction. A lateral one-fourth strip of the patellar tendon is meticulously developed, remaining attached at its proximal origin on the inferior pole of the patella.
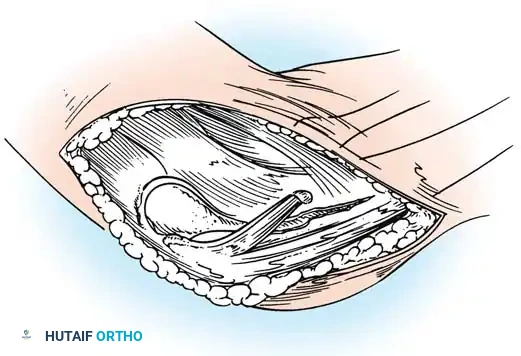
Fig. 45-17B: The harvested strip is routed laterally and attached to the lateral tibial tubercle. Fixation is achieved either by direct suturing to the robust local periosteum or by passing the tendon strip through a dedicated bony tunnel for rigid osseous integration.
Key Surgical Steps:
1. Tendon Harvest: Identify the lateral border of the patellar tendon. Longitudinally split the tendon to create a strip comprising the lateral one-fourth of its width. Detach this strip distally from the tibial tubercle, leaving its
You Might Also Like