Masterclass in Triple Arthrodesis: Advanced Surgical Techniques and Protocols

Key Takeaway
Triple arthrodesis remains a cornerstone procedure for correcting severe, rigid hindfoot and midfoot deformities. This comprehensive guide details the biomechanical principles, preoperative templating, and step-by-step surgical execution of the Siffert-Forster-Nachamie and Lambrinudi techniques. Emphasizing precise bone resection, rigid internal fixation, and meticulous soft tissue handling, these procedures provide durable stability, alleviate pain, and restore a plantigrade foot in patients with complex neuromuscular or post-traumatic pathologies.
INTRODUCTION TO TRIPLE ARTHRODESIS
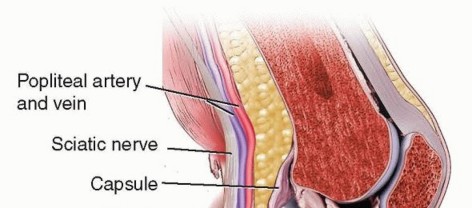
Triple arthrodesis is a powerful, time-honored orthopedic procedure designed to fuse the three primary joints of the hindfoot and midfoot: the subtalar (talocalcaneal), talonavicular, and calcaneocuboid joints. Historically conceptualized to manage the devastating sequelae of poliomyelitis, the procedure has evolved significantly. Today, it remains the gold standard for addressing severe, rigid, and painful deformities of the hindfoot that are refractory to conservative management and joint-sparing osteotomies.
The primary goals of a triple arthrodesis are to relieve pain, correct complex multiplanar deformities, restore a stable and plantigrade foot, and eliminate pathological motion that contributes to gait instability. By fusing the peritalar complex, the surgeon effectively locks the transverse tarsal joint, which subsequently limits the motion of the entire midfoot and forefoot.
Clinical Pearl: The talonavicular joint is the keystone of the triple complex. Fusion of the talonavicular joint alone eliminates approximately 90% of subtalar motion. Therefore, meticulous preparation and rigid fixation of this specific articulation are paramount to the success of the overall triple arthrodesis.
This masterclass details two highly specialized variations of the triple arthrodesis: the Siffert, Forster, and Nachamie Technique (a modification of the classic Dunn procedure) and the Lambrinudi Arthrodesis, which is specifically tailored for paralytic drop foot.
BIOMECHANICS AND PREOPERATIVE PLANNING
Biomechanical Considerations
The hindfoot functions as a complex, interdependent unit. The subtalar joint primarily accommodates inversion and eversion, allowing the foot to adapt to uneven terrain. The talonavicular and calcaneocuboid joints (Chopart's joint) dictate the flexibility of the midfoot. When the subtalar joint is everted, the axes of the talonavicular and calcaneocuboid joints are parallel, unlocking the midfoot for shock absorption. Conversely, during inversion, these axes diverge, locking the midfoot to provide a rigid lever arm for toe-off.
A triple arthrodesis permanently locks this mechanism. Consequently, adjacent joints—specifically the ankle (tibiotalar) joint and the tarsometatarsal joints—will experience increased biomechanical stress over time, predisposing the patient to adjacent segment osteoarthritis.
Indications
- Neuromuscular Deformities: Charcot-Marie-Tooth disease, residual poliomyelitis, cerebral palsy.
- Post-Traumatic Arthritis: Sequelae of calcaneus or talus fractures.
- End-Stage Inflammatory Arthritis: Rheumatoid arthritis affecting the hindfoot.
- Severe Rigid Pes Planovalgus: Stage III or IV posterior tibial tendon dysfunction (PTTD).
- Severe Rigid Pes Cavovarus: Fixed cavus deformities requiring extensive bony resection.
Contraindications
- Active local or systemic infection.
- Severe peripheral arterial disease (inadequate vascular supply for bone healing).
- Inadequate soft tissue envelope.
- Significant, unaddressed ankle joint arthritis (unless a pantalar arthrodesis is planned).
SURGICAL TECHNIQUE: SIFFERT, FORSTER, AND NACHAMIE
The Siffert, Forster, and Nachamie technique is a sophisticated modification of the classic Dunn arthrodesis. The Dunn technique historically involved the complete excision of the navicular to shorten the medial column in cases of severe deformity. The Siffert modification preserves the superior soft tissue attachments of the talus and utilizes a "beak" resection to lock the midfoot securely under the talus, providing superior intrinsic stability.
1. Exposure and Joint Preparation
- Incision: Expose the calcaneocuboid, talonavicular, and subtalar joints through a standard extended lateral approach (Ollier incision), originating from the tip of the lateral malleolus and extending distally toward the base of the fourth metatarsal. A supplementary medial incision over the talonavicular joint may be utilized if medial column access is restricted.
- Cartilage Removal: Systematically denude the calcaneocuboid and subtalar joints of all articular cartilage down to bleeding subchondral bone. Use sharp osteotomes, curettes, and a high-speed burr to ensure complete decortication while preserving the underlying joint contours.
- Navicular Preparation: Excise the dorsal cortex of the navicular to prepare the recipient bed for the talar beak.
2. Osteotomy and Beak Creation
- Wedge Planning: Plan the wedge of bone to be removed by performing an osteotomy of the anterior aspect of the calcaneus, the posterior aspect of the navicular, and the inferior aspect of the talar head and neck.
- Execution: Start the osteotomy inferiorly and carry it superiorly to the inferior surface of the talus.
- The Talar Beak: Resect the inferior portion of the talar head and neck to form a distinct "beak."
Surgical Warning: It is critical to leave the soft tissue structures on the superior aspect of the talus (anterior to the ankle joint) completely undisturbed. This preserves the tenuous blood supply to the talar body and prevents avascular necrosis.
3. Reduction and Fixation
- Displacement: Displace the forefoot plantarward. Lock the remaining proximal navicular firmly beneath the newly created beak of the talar head and neck.
- Assessment: Ensure the bones fit together snugly. The foot must be plantigrade, with the heel in neutral to maximum 5 degrees of valgus. Never fuse the hindfoot in varus.
- Internal Fixation: Obtain a firm purchase with large-fragment (6.5 mm or 7.3 mm) cannulated screws.
- Drive a screw from the posterior calcaneal tuberosity up into the body of the talus.
- Drive a second screw from the navicular into the talar head/neck.
- Drive a third screw across the calcaneocuboid joint.
- Troubleshooting Fixation: If fixation is even slightly tenuous, redrill the calcaneus in a different trajectory. If the deformity is so severe that adequate reduction cannot be achieved, the surgeon must revert to the classic Dunn technique, ensuring that the entire navicular is removed to allow for adequate shortening and realignment.
SURGICAL TECHNIQUE: THE LAMBRINUDI ARTHRODESIS
The Lambrinudi arthrodesis is a highly specialized, historically significant procedure designed specifically to address paralytic drop foot (equinus deformity), most commonly seen in poliomyelitis. Unlike a standard triple arthrodesis, the Lambrinudi technique utilizes the bony architecture of the hindfoot to create a mechanical block against plantar flexion, effectively utilizing the anterior capsule of the ankle joint to suspend the foot.
1. Preoperative Radiographic Templating
The success of the Lambrinudi procedure relies entirely on meticulous preoperative templating.
* Obtain a true lateral radiograph of the foot and ankle with the foot forced into extreme plantar flexion.
* Trace the radiographic film. Cut the tracing into three distinct pieces along the outlines of the subtalar and midtarsal joints.
* From these pieces, calculate the exact amount of bone to be removed from the talus.
* The Critical Angle: In the tracing, the line representing the articulation of the talus with the tibia must be left undisturbed. However, the line corresponding to its plantar and distal parts is cut so that, when the navicular and calcaneocuboid joints are later fitted to it, the foot rests in slight equinus relative to the leg.
* Target Alignment: Five to ten degrees of equinus is optimal. If the extremity has significant shortening (common in polio), slightly more equinus may be desirable to compensate for limb length discrepancy.
2. Surgical Approach and Soft Tissue Release
- Incision: Expose the tarsus through a long, curved lateral incision.
- Tendon Management: Section the peroneal tendons using a Z-shaped cut to allow for later repair and lengthening.
- Capsulotomy: Open the talonavicular and calcaneocuboid joints. Divide the interosseous talocalcaneal ligament and the fibular collateral ligaments of the ankle. This extensive release permits complete medial dislocation of the tarsus at the subtalar joint, providing unhindered access to the inferior talus.
3. Bone Resection and Trough Creation
- Talar Resection: Using a small power saw (which provides superior accuracy compared to a chisel or osteotome), remove the predetermined wedge of bone from the plantar and distal parts of the neck and body of the talus.
Figure A: The shaded area represents the precise wedge of the talus to be resected based on preoperative templating.
- Calcaneal Preparation: Remove the cartilage and subchondral bone from the superior surface of the calcaneus to form a flat, bleeding plane that is perfectly parallel with the longitudinal axis of the foot.
- Navicular Trough: Make a V-shaped trough transversely in the inferior part of the proximal navicular. Denude the calcaneocuboid joint of enough bone to correct any pre-existing lateral or medial column deformity.
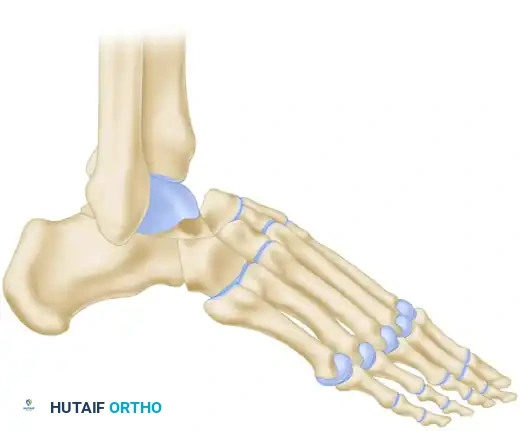
Figure B: The sharp distal margin of the remaining talus is wedged into the prepared V-shaped trough in the navicular.
4. Reduction and Locking Mechanism
- Wedging the Talus: Firmly wedge the sharp, newly created distal margin of the remaining part of the talus into the prepared V-shaped trough in the navicular.
- Apposition: Appose the prepared superior surface of the calcaneus to the inferior surface of the talus.
Figure C: Final apposition of the raw osseous surfaces of the talus, calcaneus, and cuboid, demonstrating the mechanical block.
Surgical Pitfall: Place the distal margin of the talus well medially in the navicular trough. If placed too laterally, the position of the foot will fall into an unacceptable varus alignment. Furthermore, no attempt should be made to compensate for any tibial torsion within the foot itself; doing so will compromise the plantigrade nature of the arthrodesis.
- Mechanical Check: Once reduced, the talus is locked in the ankle joint in complete equinus, and the foot cannot be plantar flexed any farther. The anterior ankle capsule is now under tension, preventing drop foot.
- Closure: Suture the peroneal tendons (repairing the Z-lengthening) and close the wound in layers over a closed suction drain.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is critical to ensure solid bony union and prevent displacement of the meticulously crafted bone cuts.
Immediate Postoperative Phase (0 to 14 Days)
- Immobilization: A bulky, well-padded short-leg cast or posterior splint is applied in the operating room.
- For Siffert/Dunn: The foot is held in a neutral, plantigrade position with 0-5 degrees of hindfoot valgus.
- For Lambrinudi: The cast is applied with the foot in moderate equinus (as templated) and the knee in slight flexion. Firm pressure is exerted on the sole of the foot while the plaster is setting to stretch the plantar structures as much as possible and lock the talus into the navicular trough.
- Elevation: The cast is suspended by slings to an overhead frame for 48 to 72 hours to aggressively manage edema. Strict elevation above the level of the heart is mandatory.
- Weight-Bearing: Strictly non-weight-bearing (NWB).
Intermediate Phase (2 to 6 Weeks)
- Wound Check: At 10 to 14 days, the initial cast is removed. The surgical incisions are inspected, and sutures or staples are removed.
- Casting: A new, snug-fitting short-leg fiberglass cast is applied.
- Mobility: Non-weight-bearing ambulation on crutches or a knee scooter is allowed. This NWB cast is worn for an additional 4 weeks.
Late Phase (6 to 12+ Weeks)
- Radiographic Assessment: At 6 weeks postoperatively, the cast is removed, and out-of-cast weight-bearing radiographs (AP, Lateral, and Mortise views) are obtained to assess early trabecular bridging across the arthrodesis sites.
- Weight-Bearing Progression: If clinical and radiographic signs of early union are present, the patient is transitioned to a short-leg walking cast or a rigid controlled ankle motion (CAM) boot. Weight-bearing to tolerance (WBAT) is initiated.
- Final Union: The walking cast or boot is worn until solid bony union is demonstrated both clinically (absence of pain on palpation/stress) and radiographically. This typically occurs at 10 to 12 weeks after surgery, though patients with significant comorbidities (e.g., diabetes, smoking history) may require up to 16 weeks.
COMPLICATIONS AND MANAGEMENT
Even in the hands of master surgeons, triple arthrodesis carries inherent risks due to the complexity of the deformity correction and the vascular anatomy of the hindfoot.
- Nonunion / Delayed Union: The talonavicular joint is the most frequent site of nonunion in a triple arthrodesis (up to 10% in some series). This is due to its spherical anatomy, which makes rigid compression difficult, and its watershed blood supply. Management requires prolonged immobilization, bone stimulators, or revision surgery with structural bone grafting.
- Malunion: Fusing the hindfoot in varus is the most devastating technical error. A varus heel locks the transverse tarsal joint rigidly, leading to lateral column overload, fifth metatarsal stress fractures, and severe pain. Revision osteotomy is mandatory for symptomatic varus malunion.
- Avascular Necrosis (AVN) of the Talus: Aggressive soft tissue stripping of the dorsal talar neck can disrupt the artery of the tarsal canal and the dorsal pedis branches. The Siffert beak technique specifically aims to minimize this by preserving dorsal soft tissues.
- Adjacent Segment Disease: Over a period of 10 to 20 years, the rigid hindfoot transfers stress to the ankle joint and the tarsometatarsal joints, frequently leading to secondary osteoarthritis. Patients must be counseled preoperatively regarding this long-term biomechanical consequence.
📚 Medical References
You Might Also Like