Elbow Arthrodesis

Introduction and Epidemiology
Elbow arthrodesis (EA) is a rare, technically demanding, and functionally consequential intervention in modern orthopedic surgery. Historically recognized as a primary treatment modality for tuberculous septic elbow arthritis—where early techniques yielded a modest 50% primary fusion rate—the procedure has evolved into a definitive salvage operation. The advent of modern rigid internal fixation, governed by AO principles and particularly the utilization of dual orthogonal or parallel compression plating, has dramatically improved outcomes. Contemporary literature reports primary fusion success rates approximating 86%. When factoring in subsequent revision surgeries, final fusion rates demonstrate robust efficacy, ranging from 83% to 100%.
Despite these advancements in achieving osseous union, elbow arthrodesis carries a substantial morbidity profile. The procedure is fraught with perioperative and postoperative challenges, characterized by a high reoperation burden averaging 1.4 to 1.6 procedures per patient. Revisions are most frequently necessitated by nonunion, persistent deep space infection, catastrophic wound healing failures, and symptomatic hardware prominence in a historically poor soft-tissue envelope.

From a kinematic and functional standpoint, arthrodesis of the elbow imposes a significantly greater degree of disability than fusions of larger, weight-bearing joints such as the hip, knee, or ankle. The elbow serves as the critical mechanical linkage positioning the hand in space; its rigid immobilization profoundly diminishes upper extremity utility. This deficit can only be partially compensated by hypermobility and adaptive kinematics at the ipsilateral shoulder girdle, radiocarpal joint, and axial trunk. Consequently, with the maturation of total elbow arthroplasty (TEA) and advanced protocols for managing chronic osteomyelitis, the indications for EA have become highly restrictive. It is currently reserved for extreme scenarios where reconstructive arthroplasty is contraindicated or exhausted, prioritizing the creation of a stable, painless, and infection-free limb over the restoration of articular mobility.
Surgical Anatomy and Biomechanics
A rigorous comprehension of the elbow's osseous architecture, soft-tissue envelope, and local neurovascular topography is imperative for executing a successful arthrodesis, particularly given the distorted anatomy typically encountered in salvage scenarios.
Osteology of the Elbow Joint
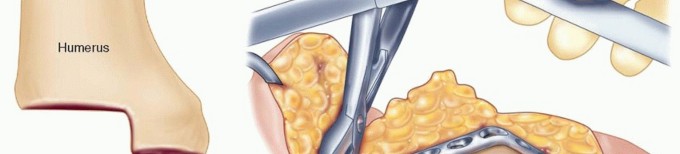
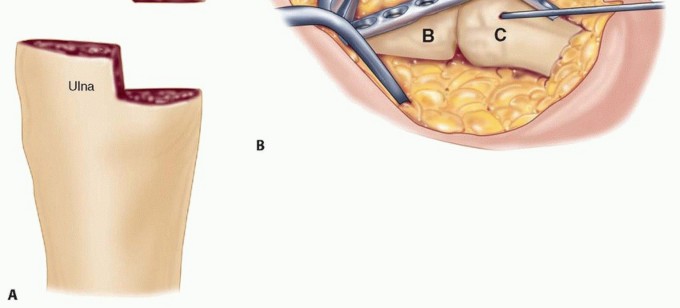
The articular complex comprises the distal humerus, proximal ulna, and proximal radius. The distal humerus presents the spool-shaped trochlea medially and the hemispherical capitellum laterally. The trochlea articulates with the greater sigmoid notch of the proximal ulna, bounded by the olecranon posteriorly and the coronoid process anteriorly. The capitellum articulates with the concave fovea of the radial head.

In the context of arthrodesis, these articular congruities are systematically dismantled. The surgical objective requires radical decortication of the trochlea, capitellum, greater sigmoid notch, and frequently the radial head, to expose bleeding subchondral bone. In salvage cases—such as failed TEA or chronic osteomyelitis—the native bone stock is often critically compromised, presenting massive cavitary or segmental defects that dictate the necessity for structural allografting or massive autogenous bone grafting to achieve mechanical stability and biologic union.
Ligamentous Stability and Joint Capsule
The native stability of the elbow is conferred by its highly congruent osseous anatomy augmented by the collateral ligamentous complexes. The medial collateral ligament (MCL), specifically its anterior bundle, is the primary restraint to valgus stress. The lateral ulnar collateral ligament (LUCL) serves as the primary restraint to posterolateral rotatory instability. During arthrodesis, these ligamentous structures, along with the joint capsule, are routinely excised to mobilize the joint and facilitate optimal positioning for fusion. The radical resection of these stabilizing structures transfers the entirety of the mechanical load to the internal fixation construct until solid osseous union is achieved.

Neurovascular Topography
The neurovascular anatomy surrounding the elbow dictates the surgical approach and represents a significant source of potential perioperative morbidity. The ulnar nerve courses posterior to the medial epicondyle within the cubital tunnel before entering the forearm between the two heads of the flexor carpi ulnaris. In the setting of elbow arthrodesis, particularly when utilizing posterior or medial plating techniques, the ulnar nerve is at extreme risk. Routine identification, neurolysis, and anterior transposition are generally mandated to prevent iatrogenic injury or late compressive neuropathy from postoperative scarring or hardware prominence.
The radial nerve transitions from the posterior compartment of the arm to the anterior compartment by piercing the lateral intermuscular septum approximately 10 centimeters proximal to the lateral epicondyle. It then courses anterior to the radiocapitellar joint. Extensive lateral dissection or the placement of long posterior plates extending proximally on the humerus necessitates meticulous identification and protection of the radial nerve.
The median nerve and brachial artery traverse the anterior compartment, crossing the joint line medial to the biceps tendon. While less frequently exposed during a standard posterior approach for arthrodesis, these structures are vulnerable during radical anterior capsulectomy, removal of extruded cement from prior arthroplasty, or when addressing severe flexion contractures.

Kinematics and Biomechanical Considerations
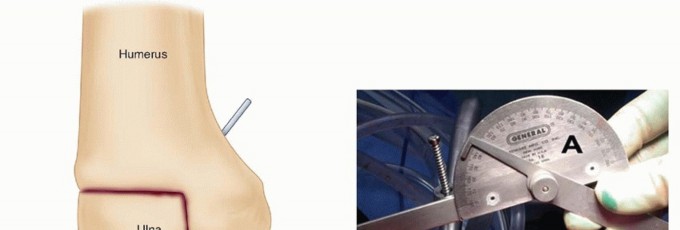
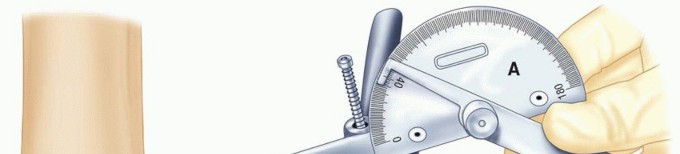
The determination of the optimal position for elbow arthrodesis is a complex biomechanical and functional calculation. The normal arc of elbow motion ranges from 0 degrees of extension to 140 degrees of flexion, with functional tasks typically requiring an arc between 30 and 130 degrees.
When arthrodesis is performed, the surgeon must select a static angle that maximizes the patient's ability to perform activities of daily living (ADLs). Historically, a position of 90 degrees of flexion with neutral forearm rotation was advocated as the universal standard. However, contemporary biomechanical analyses and patient-reported outcome studies suggest that the optimal position is highly individualized.
For unilateral arthrodesis, a position of 90 to 110 degrees of flexion is generally preferred to allow the hand to reach the mouth for feeding and the head for hygiene. If the patient relies heavily on the extremity for pushing up from a chair or utilizing walking aids, a more extended position (approximately 60 to 70 degrees) may be biomechanically advantageous. In the exceedingly rare scenario of bilateral elbow arthrodesis, one limb is typically fused at 110 degrees to facilitate feeding, while the contralateral limb is fused at 65 degrees to assist with perineal care and spatial reach.

From a structural biomechanics perspective, the elbow joint experiences significant torque. The long lever arms of the humerus and forearm generate massive bending moments at the fusion site. Consequently, the fixation construct must possess a high area moment of inertia. Dual plating configurations (either orthogonal or parallel) are mechanically superior to single plating or external fixation, as they provide robust resistance to both torsional and cantilever bending forces during the extended period required for osseous consolidation.
Indications and Contraindications
The decision to proceed with elbow arthrodesis is rarely made in the acute setting. It is predominantly a tertiary referral procedure, utilized when all other reconstructive options have been exhausted.
Primary Surgical Indications
The most common contemporary indication for elbow arthrodesis is the catastrophic failure of a total elbow arthroplasty (TEA). Failed TEA is often accompanied by massive osteolysis, periprosthetic joint infection (PJI), and critical loss of the condylar bone stock, rendering revision arthroplasty impossible.
Chronic, recalcitrant septic arthritis or osteomyelitis of the distal humerus or proximal ulna represents another major indication. In these scenarios, arthrodesis is typically performed as a staged procedure following radical debridement, placement of antibiotic-impregnated spacers, and targeted systemic antimicrobial therapy.
Severe post-traumatic conditions, including unreconstructable intra-articular distal humerus fractures in young, heavy laborers, may occasionally warrant primary arthrodesis. While TEA is an option for older, low-demand patients with such fractures, the lifetime lifting restrictions associated with TEA make it an inappropriate choice for manual laborers.
Neurologic deficits, such as severe flaccid paralysis secondary to brachial plexus avulsion injuries, can also serve as an indication. In these cases, arthrodesis stabilizes the elbow in a functional position, allowing the patient to utilize residual shoulder or hand function more effectively.

Absolute and Relative Contraindications
Absolute contraindications to elbow arthrodesis are few but critical. Active, untreated deep space infection precludes definitive internal fixation and bone grafting. In the presence of active sepsis, a staged approach is mandatory. Severe soft-tissue compromise that cannot be addressed via local or free tissue transfer is also an absolute contraindication, as robust coverage is essential to prevent hardware exposure and subsequent failure.
Relative contraindications include severe dysfunction of the contralateral upper extremity. Rigid immobilization of one elbow places extraordinary functional demands on the contralateral limb; if the opposite limb is compromised, the patient's independence will be devastatingly curtailed. Advanced age and low physical demand are also relative contraindications, as these patients are generally better served by resection arthroplasty (flail elbow) or complex revision TEA, which preserve some degree of motion and require less rigorous bone healing.

Table of Indications and Salvage Alternatives
| Clinical Scenario | Arthrodesis Indication | Alternative Salvage Option | Rationale for Alternative |
|---|---|---|---|
| Failed TEA with massive bone loss | High (if young/high demand) | Resection Arthroplasty | Elderly/low demand; avoids nonunion risk. |
| Recalcitrant Periprosthetic Infection | High (staged approach) | Amputation | Life-threatening sepsis; intractable pain. |
| Unreconstructable Distal Humerus Fracture | High (manual laborers) | Total Elbow Arthroplasty | Elderly patients; preserves joint kinematics. |
| Brachial Plexus Palsy (Flaccid Elbow) | High (to position hand) | Functional Bracing | Patient refuses surgery; high surgical risk. |
| Severe Rheumatoid Arthritis | Low | Total Elbow Arthroplasty | Polyarticular disease requires motion preservation. |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful elbow arthrodesis. The compromised nature of the soft tissues and bone stock in these salvage cases leaves little margin for intraoperative error.
Clinical and Radiographic Evaluation
The clinical examination must rigorously assess the soft-tissue envelope. Previous surgical incisions should be mapped to optimize the surgical approach and minimize the risk of skin necrosis. The vascular status of the limb is evaluated via palpation of radial and ulnar pulses, supplemented by Doppler ultrasound or angiography if vascular compromise is suspected. A detailed neurologic examination is mandatory, with specific attention to ulnar nerve function, as preoperative neuropathy must be documented and addressed during surgery.
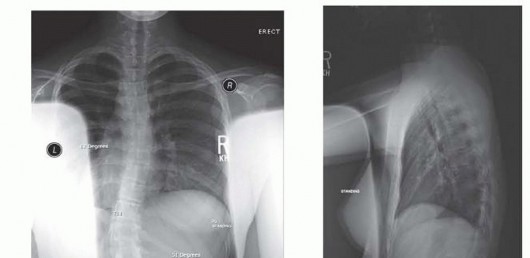
Radiographic evaluation begins with orthogonal plain radiographs of the humerus, elbow, and forearm. These images provide a baseline assessment of bone loss, hardware presence, and deformity.

Advanced imaging is routinely required. Computed Tomography (CT) with metal artifact reduction sequence (MARS) is invaluable for quantifying volumetric bone defects and planning structural graft dimensions. If an indolent infection is suspected in the setting of prior hardware or arthroplasty, inflammatory markers (ESR, CRP) are drawn, and a tagged white blood cell scan or MRI may be utilized to localize the infectious burden.
Preoperative templating involves selecting the appropriate hardware. Standard 3.5mm or 4.5mm dynamic compression plates, locking compression plates (LCP), or specialized pre-contoured arthrodesis plates are evaluated against the patient's anatomy. The surgeon must also plan the source and volume of bone graft. Autogenous iliac crest bone graft (ICBG) remains the gold standard for biologic activity, but massive defects may necessitate structural fibular allografts or custom-milled femoral head allografts.

Patient Positioning and Operating Room Setup
Patient positioning must facilitate extensile exposure of the posterior elbow while allowing access to bone graft harvest sites. The lateral decubitus position is frequently preferred. The patient is secured with a beanbag, and the operative arm is draped free over a padded sterile post. This position allows unimpeded access to the posterior elbow and facilitates gravity-assisted retraction. Furthermore, the lateral decubitus position provides excellent access to the posterior superior iliac spine (PSIS) for autogenous bone graft harvest.
Alternatively, the patient may be positioned prone, with the arm resting on a radiolucent arm board. This also provides excellent posterior exposure but can complicate airway management and access to the anterior iliac crest if required.
A sterile tourniquet is applied high on the brachium. The use of a tourniquet is generally recommended to minimize blood loss and improve visualization during the arduous dissection, though it must be deflated prior to final closure to ensure meticulous hemostasis. Fluoroscopy is positioned to enter from the anterior aspect of the patient, allowing for orthogonal intraoperative imaging without compromising the sterile field.
Detailed Surgical Approach and Technique
The surgical execution of an elbow arthrodesis is a complex, multi-stage endeavor requiring meticulous soft-tissue handling, radical bone preparation, and rigid biomechanical stabilization.
Incision and Extensile Exposure
A universal posterior longitudinal incision is the standard approach. The incision is centered over the olecranon, curving slightly laterally to avoid the tip of the olecranon, which is prone to wound breakdown. In revision scenarios, previous incisions should be incorporated if possible, maintaining broad skin bridges to preserve vascularity.
Full-thickness fasciocutaneous flaps are elevated medially and laterally. The triceps mechanism is mobilized. Depending on the extent of exposure required, a triceps-reflecting (Bryan-Morrey) approach, a triceps-splitting approach, or an olecranon osteotomy may be utilized. In cases of failed TEA, the triceps is often already compromised, and a broad V-Y turndown or complete reflection from the olecranon is necessary to gain access to the distal humerus and proximal ulna.

Ulnar Nerve Transposition
Early in the dissection, the ulnar nerve must be identified proximally in the posterior compartment of the arm and traced distally into the cubital tunnel. The nerve is circumferentially neurolysed and mobilized. The medial intermuscular septum is excised to prevent kinking. The nerve is then transposed anteriorly into a subcutaneous or submuscular bed. This step is non-negotiable, as the placement of heavy posterior and medial plates will otherwise impinge upon or obliterate the native cubital tunnel.
Joint Preparation and Debridement
The core principle of joint preparation is the creation of broad, bleeding, congruent cancellous bony surfaces. All remaining articular cartilage, fibrous tissue, and sclerotic bone must be aggressively resected using osteotomes, rongeurs, and high-speed burrs.
In the setting of a failed TEA, all prosthetic components and polymethylmethacrylate (PMMA) bone cement must be meticulously extracted. The intramedullary canals of the humerus and ulna are reamed to healthy, bleeding bone. A prophylactic cerclage wire may be placed around the distal humerus and proximal ulna prior to component extraction to prevent iatrogenic longitudinal fractures.
The radial head is frequently excised to provide autogenous local bone graft and to eliminate a potential source of impingement or radiocapitellar pain. However, if the radioulnar joint is pristine and forearm rotation is to be preserved, the radial head may be retained, though achieving fusion of the humeroulnar joint while preserving proximal radioulnar motion is technically challenging and risks synostosis.

Bone Grafting Strategies
The management of bone defects is critical to the success of the arthrodesis. Simple decortication is rarely sufficient in salvage cases.
For segmental defects, structural grafting is required. A dual onlay fibular strut graft technique is highly effective. The fibular struts are placed bridging the humeroulnar defect and secured with independent lag screws. Alternatively, an intramedullary structural graft (such as a fibula or a custom-shaped femoral head allograft) can be impacted into the humeral and ulnar canals, acting as an internal dowel to provide immediate mechanical stability.
Cancellous autograft, harvested from the iliac crest or utilizing Reamer-Irrigator-Aspirator (RIA) techniques from the femur, is densely packed into all remaining interstices. The osteoinductive and osteogenic properties of autograft are essential to stimulate union in the hostile, avascular environment typical of revision elbow surgery. Demineralized bone matrix (DBM) and bone morphogenetic proteins (BMP-2 or BMP-7) are frequently utilized as adjuncts, particularly in patients with a history of nonunion or compromised biology.

Reduction and Internal Fixation Techniques
Once the bone ends are prepared and grafted, the elbow is positioned at the pre-determined angle of fusion (typically 90 degrees). Temporary stabilization is achieved with heavy Steinmann pins or provisional external fixation.
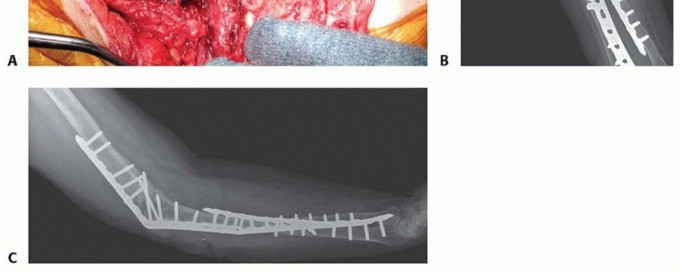
The gold standard for internal fixation is the application of dual, heavy-duty plates. A 90-90 orthogonal configuration is biomechanically optimal.
The primary plate is typically a 4.5mm dynamic compression plate (DCP) or locking compression plate (LCP) contoured to the posterior aspect of the humerus and the dorsal aspect of the ulna. Contouring a thick 4.5mm plate to accommodate the 90-degree bend requires specialized plate benders and careful templating to avoid stress risers at the bend. The plate is secured with bicortical screws, utilizing compression techniques across the fusion interface if the bone stock permits.

A secondary plate, usually a 3.5mm reconstruction plate or LCP, is applied orthogonally. This plate is typically positioned on the medial or lateral aspect of the humerus and extended down the corresponding aspect of the ulna. The addition of this second plate significantly increases the torsional rigidity of the construct and neutralizes cantilever bending forces that would otherwise lead to fatigue failure of a single posterior plate.
In scenarios where bone quality is profoundly osteoporotic, locking screws are utilized extensively. Long intramedullary screws passing from the olecranon into the humeral canal can also be employed as an adjunct to augment the plate fixation.
Soft Tissue Reconstruction and Closure
Following rigid fixation, the tourniquet is deflated, and meticulous hemostasis is achieved. The soft-tissue envelope over the posterior elbow is naturally thin and is often further compromised by multiple prior surgeries.
If the posterior soft tissues cannot be closed without tension, or if the hardware is excessively prominent, local muscle flaps are indicated. The anconeus flap or the flexor carpi ulnaris (FCU) flap can be rotated to provide vascularized coverage over the olecranon and proximal ulna. In cases of massive soft-tissue defects, consultation with a microsurgical reconstructive team for a free tissue transfer (e.g., latissimus dorsi
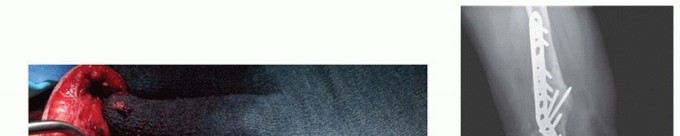
Clinical & Radiographic Imaging






You Might Also Like