Open Reduction and Internal Fixation of Radial Head and Neck Fractures

Introduction and Epidemiology
Radial head and neck fractures represent the most frequently encountered elbow fractures in the adult demographic, constituting approximately 33% of all elbow fractures and nearly 20% of all acute elbow injuries. Epidemiological data indicates a bimodal distribution, though they occur most frequently in adults between the ages of 20 and 60 years, with a slight predilection for females in the osteopenic population. The classic mechanism of injury involves an indirect axial load applied to a pronated forearm with the elbow in partial flexion. This position directs the kinetic energy from the carpus, through the interosseous membrane, directly into the radiocapitellar joint, frequently resulting from a fall on an outstretched hand (FOOSH).
While these fractures frequently present as isolated injuries, they are notoriously associated with complex osseous, osteochondral, and capsuloligamentous disruption. The surgeon must maintain a high index of suspicion for highly morbid associated patterns. These include the terrible triad of the elbow (radial head fracture, coronoid fracture, and acute elbow dislocation), Essex-Lopresti injuries (radial head fracture combined with longitudinal interosseous membrane disruption and distal radioulnar joint instability), and various Monteggia fracture-dislocation variants.
The management algorithm for radial head and neck fractures spans a broad spectrum, ranging from nonoperative functional rehabilitation for stable, nondisplaced patterns to open reduction and internal fixation (ORIF), fragment excision, or primary radial head arthroplasty (RHA) for complex configurations. The overarching objective of any intervention is the anatomic restoration of elbow and forearm kinematics, encompassing both dynamic motion and static stability. The decision-making matrix relies heavily on fracture morphology, the degree of metaphyseal comminution, and the competence of the surrounding primary and secondary ligamentous stabilizers.
Fracture Classification Systems
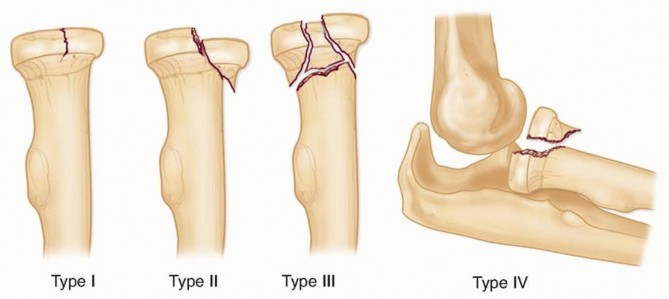
The Mason classification, originally described in 1954, remains the most universally utilized and clinically relevant system for categorizing radial head fractures, primarily because it directly guides therapeutic decision-making.
- Type I Nondisplaced or minimally displaced fractures (less than 2 mm of articular step-off) with no mechanical block to forearm rotation.
- Type II Displaced fractures (greater than 2 mm) involving more than 30% of the articular surface, potentially creating a mechanical block to pronosupination.
- Type III Severely comminuted and displaced fractures involving the entire radial head, often precluding reliable osteosynthesis.
- Type IV A modification added by Johnston, defining any radial head fracture (Types I-III) associated with a concomitant elbow dislocation.

The Broberg and Morrey modification further refines these definitions by strictly quantifying the displacement and articular involvement necessary to warrant surgical intervention, providing a more objective threshold for operative management. Hotchkiss further modified the Mason classification to base treatment algorithms on clinical findings, specifically the presence of a mechanical block and the amenability of the fracture to osteosynthesis versus arthroplasty.
Understanding the epidemiology requires an appreciation of the energy transfer mechanisms. High-energy trauma in younger demographics often yields severely comminuted Mason III fractures with associated ligamentous compromise, whereas low-energy falls in osteopenic individuals frequently result in Mason I or II cleavage-type fractures. The recognition of these distinct patterns is paramount for anticipating the requisite surgical inventory and preoperative planning.

The incidence of concomitant injuries cannot be overstated. Magnetic resonance imaging (MRI) studies have demonstrated that up to 80% of patients with ostensibly isolated radial head fractures possess some degree of lateral ulnar collateral ligament (LUCL) sprain, and approximately 30% have associated medial collateral ligament (MCL) signal changes. Furthermore, osteochondral lesions of the capitellum are frequently observed due to the impaction forces generated during the initial traumatic event.

Surgical Anatomy and Biomechanics
A profound understanding of proximal radius osteology, regional vascularity, and capsuloligamentous anatomy is an absolute prerequisite for successful ORIF. The radial head is not a perfect cylinder; rather, it is elliptical in axial cross-section. The concave articular dish (fovea) articulates with the capitellum, while the peripheral margin (articular circumference) articulates with the lesser sigmoid notch of the proximal ulna.
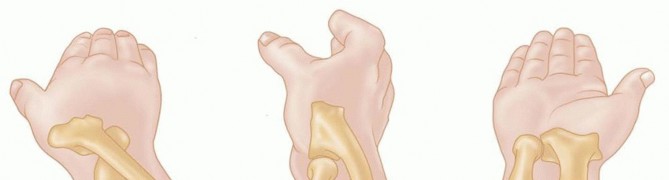
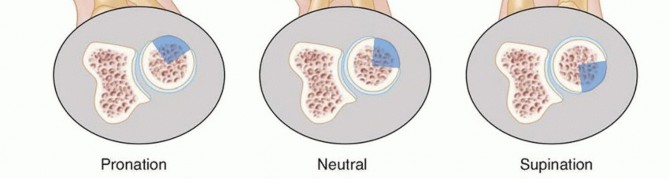
The Safe Zone
The radial head possesses a critical non-articulating arc, classically referred to as the safe zone. This region encompasses approximately 105 to 120 degrees of the lateral radial head circumference when the forearm is in neutral rotation. It is devoid of hyaline cartilage and does not articulate with the lesser sigmoid notch of the ulna during the normal arc of pronosupination.
Intraoperatively, the safe zone can be identified by referencing the radial styloid and Lister's tubercle. Bisecting the radial head with an imaginary line extending proximally from the radial styloid defines the anterior border of the safe zone, while a line extending from Lister's tubercle defines the posterior border. Implants placed outside this zone will inevitably impinge upon the proximal radioulnar joint (PRUJ), leading to severe restriction of forearm rotation, articular cartilage degradation, and early-onset osteoarthritis.
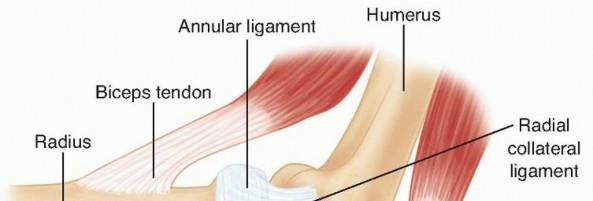
Capsuloligamentous Stabilizers
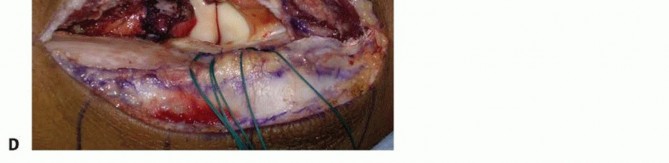
The radial head is intimately associated with the lateral collateral ligament (LCL) complex, which consists of the radial collateral ligament (RCL), the lateral ulnar collateral ligament (LUCL), and the annular ligament. The LUCL is the primary restraint to posterolateral rotatory instability (PLRI). It originates from the lateral epicondyle, blending with the annular ligament, and inserts onto the supinator crest of the ulna.

The annular ligament encircles the radial head, stabilizing it within the lesser sigmoid notch. During surgical exposure, particularly via the Kocher approach, the surgeon must be cognizant of the LUCL's origin and trajectory to avoid iatrogenic destabilization. If the LUCL is avulsed or iatrogenically transected, it must be meticulously repaired to the lateral epicondyle using suture anchors or transosseous tunnels to prevent chronic PLRI.
Elbow Biomechanics and Load Transmission
Biomechanically, the radial head is a crucial secondary stabilizer to valgus stress. The anterior bundle of the medial collateral ligament (AMCL) is the primary restraint. However, in the setting of AMCL deficiency, the radial head becomes the primary osseous block against valgus displacement. Consequently, excision of the radial head in the presence of an incompetent AMCL will lead to catastrophic valgus instability.

Furthermore, the radiocapitellar joint is responsible for transmitting approximately 60% of the axial load across the elbow joint during maximal extension, with the remaining 40% transmitted through the ulnohumeral articulation. This load transmission dynamic shifts depending on the degree of elbow flexion and forearm rotation. Preservation of the radial head, either through anatomic osteosynthesis or appropriately sized arthroplasty, is imperative to maintain this force distribution and prevent proximal migration of the radius, which would otherwise culminate in ulnocarpal impaction syndrome.
Indications and Contraindications
The decision to proceed with operative intervention for radial head and neck fractures requires a nuanced synthesis of fracture morphology, patient demands, and the integrity of the surrounding soft tissue envelope. The primary goal is the restoration of a stable, congruent radiocapitellar and proximal radioulnar articulation to permit early, active mobilization.
Operative vs Non Operative Management
| Indication Category | Non-Operative Management | Operative Management (ORIF) |
|---|---|---|
| Fracture Displacement | < 2 mm articular step-off | ≥ 2 mm articular step-off |
| Articular Involvement | < 30% of articular surface | ≥ 30% of articular surface |
| Mechanical Block | Full passive pronosupination | Mechanical block to rotation |
| Associated Injuries | Isolated injury, stable ligaments | Terrible triad, Essex-Lopresti, Monteggia variants |
| Elbow Stability | Concentric reduction, stable to stress | Instability, subluxation, or frank dislocation |
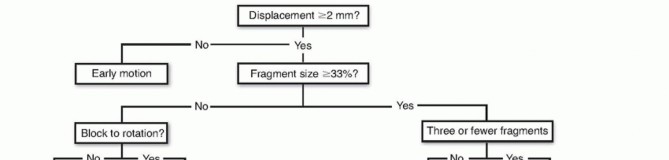
Nondisplaced or minimally displaced fractures (Mason Type I) are universally managed nonoperatively with a brief period of immobilization (sling for comfort) followed by early active range of motion within 48 to 72 hours. Prolonged immobilization is strictly contraindicated as it invariably leads to debilitating elbow stiffness.
Operative intervention is indicated for displaced fractures (Mason Type II) that create a mechanical block to rotation. The presence of a mechanical block is best assessed by aspirating the radiocapitellar joint hematoma and injecting local anesthetic to eliminate pain-induced muscle guarding. If passive pronosupination remains restricted or a distinct "catch" is palpable, surgical intervention is warranted.

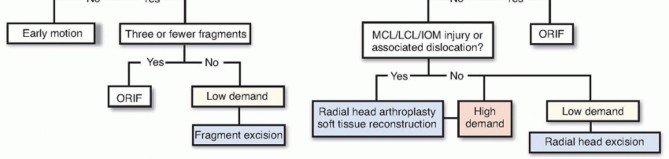
For complex, comminuted fractures (Mason Type III), the decision lies between ORIF and radial head arthroplasty. ORIF is indicated when the fracture pattern consists of three or fewer major articular fragments that can be anatomically reduced and rigidly fixed without compromising the vascularity of the segments. If the fracture is highly comminuted, osteopenic, or involves significant metaphyseal bone loss precluding stable fixation, radial head arthroplasty is the procedure of choice.

Contraindications to ORIF
Absolute contraindications to ORIF include active local or systemic infection and critical medical comorbidities precluding anesthesia. Relative contraindications include severe osteopenia, which limits screw purchase and increases the risk of catastrophic hardware failure. Additionally, fractures with more than three articular fragments (excluding the neck) are generally considered a relative contraindication to ORIF due to the high incidence of nonunion, malunion, and avascular necrosis. In these scenarios, primary radial head excision (only if ligaments are intact) or arthroplasty is favored.
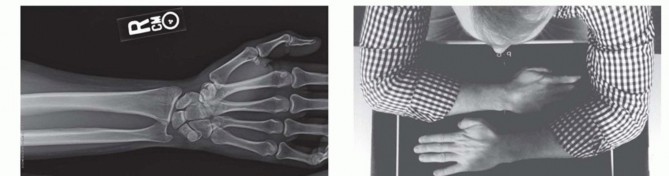
Pre Operative Planning and Patient Positioning
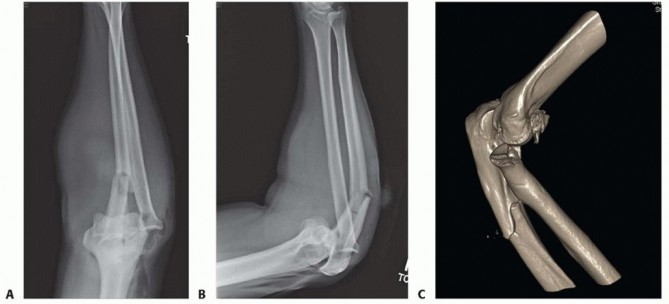
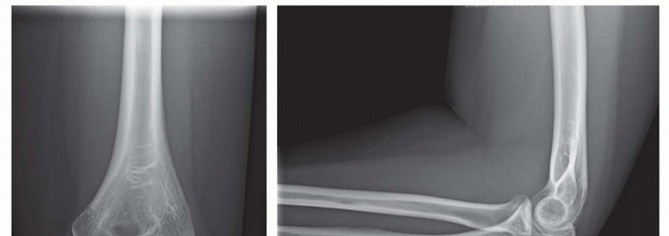
Thorough preoperative planning is critical for optimizing surgical outcomes and minimizing intraoperative delays. Standard orthogonal radiographs (anteroposterior and lateral views) of the elbow are mandatory. A supplemental radiocapitellar view (Greenspan view), obtained with the beam angled 45 degrees cephalad, can better delineate the articular surface of the radial head and the capitellum.
Advanced Imaging Considerations
In the setting of complex comminution, displaced head-neck junction fractures, or suspected associated injuries, a non-contrast computed tomography (CT) scan with 3D reconstructions is highly recommended. CT imaging provides invaluable spatial information regarding fragment morphology, the degree of articular impaction, and the presence of occult coronoid or capitellar fractures. This facilitates precise preoperative templating and aids in determining whether osteosynthesis is feasible or if arthroplasty should be anticipated.
Patient Positioning and Setup
The patient is typically positioned supine on the operating table. The operative extremity is placed on a radiolucent hand table. A non-sterile tourniquet is applied high on the brachium to provide a bloodless surgical field. The arm is prepped and draped in a standard sterile fashion, ensuring that the drape allows for full, unrestricted flexion, extension, pronation, and supination of the elbow and forearm.
Alternatively, for complex fracture-dislocations requiring posterior or medial access (e.g., terrible triad injuries requiring coronoid fixation or MCL repair), a lateral decubitus position with the arm draped over a well-padded post may be utilized. This position allows gravity to assist with elbow flexion and provides excellent access to the posterior and lateral compartments.
Regardless of the position, the fluoroscopy unit (C-arm) must be positioned to allow easy access for intraoperative imaging without compromising the sterile field. The surgeon must verify that perfect AP and lateral fluoroscopic views can be obtained prior to making the incision. The surgical inventory must include a comprehensive mini-fragment set (1.5 mm, 2.0 mm, and 2.4 mm screws), headless compression screws, low-profile radial head and neck plates, and a modular radial head arthroplasty system available as a contingency.
Detailed Surgical Approach and Technique
The surgical approach to the radial head must provide adequate exposure for reduction and fixation while meticulously protecting the posterior interosseous nerve (PIN) and the lateral ligamentous stabilizers. The two primary approaches utilized are the Kocher approach and the Kaplan approach.
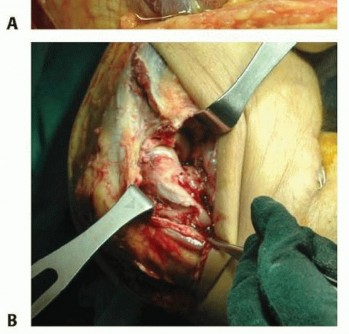
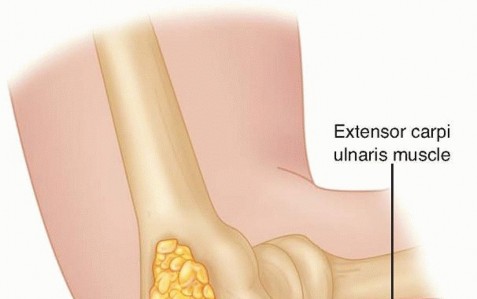
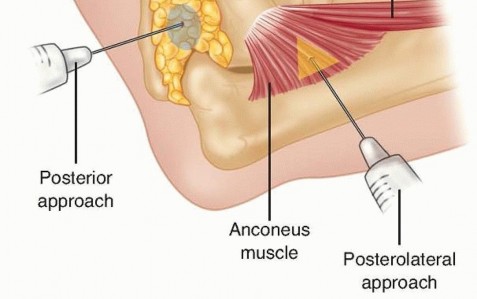
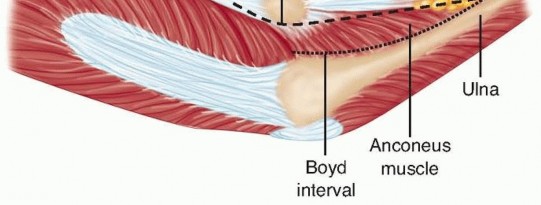
The Kocher Approach
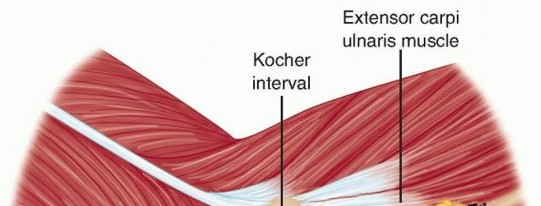
The Kocher approach exploits the internervous plane between the anconeus (innervated by the radial nerve) and the extensor carpi ulnaris (ECU, innervated by the PIN).
- An oblique incision is made extending distally from the lateral epicondyle toward the ulnar crest.
- The deep fascia is incised, and the interval between the anconeus and ECU is developed.
- The joint capsule and annular ligament are exposed. The capsule is incised anterior to the equator of the radial head to avoid iatrogenic injury to the LUCL, which lies posteriorly.
- To protect the PIN, the forearm is fully pronated. Pronation translates the PIN anteriorly and medially, safely away from the surgical field. Dissection should not extend distal to the annular ligament unless absolutely necessary, and retractors must be placed with extreme care.

The Kaplan Approach
The Kaplan approach utilizes the internervous plane between the extensor digitorum communis (EDC, innervated by the PIN) and the extensor carpi radialis brevis (ECRB, innervated by the radial nerve) or extensor carpi radialis longus (ECRL).
- A longitudinal incision is made originating at the lateral epicondyle and extending distally over the radial head.
- The interval between the EDC and ECRB is identified and developed.
- This approach provides a more direct, anterior exposure of the radial head and coronoid compared to the Kocher approach.
- However, the PIN crosses the operative field more proximally in the Kaplan approach, necessitating meticulous identification and protection. The capsule is incised longitudinally, splitting the annular ligament.

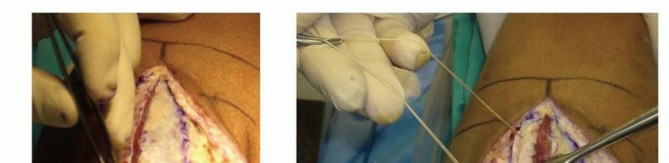
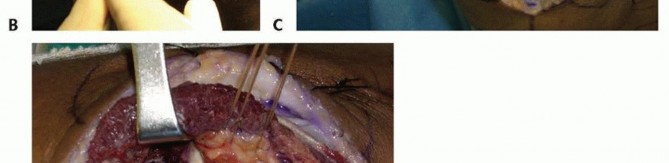
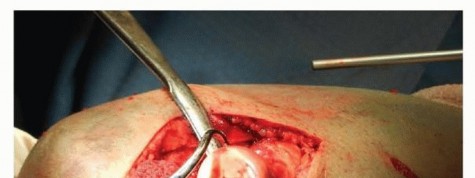
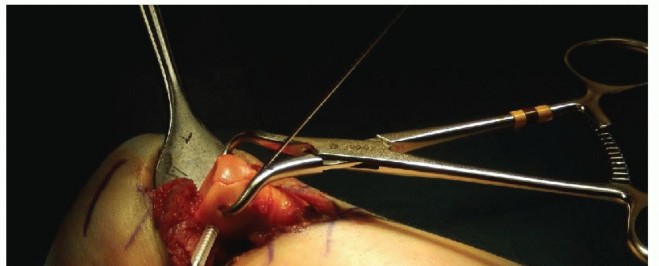
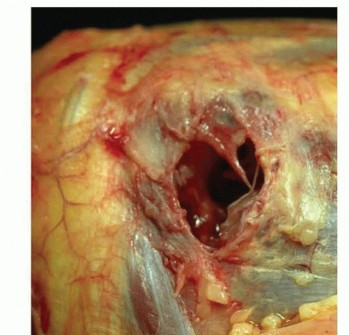
Fracture Preparation and Reduction
Upon entering the radiocapitellar joint, the fracture hematoma is evacuated, and the joint is copiously irrigated. Small, devitalized osteochondral fragments that do not contribute to structural stability are excised. The fracture surfaces are meticulously debrided of interposed soft tissue and organized clot using a dental pick or small curette.

Provisional reduction is achieved using fine Kirschner wires (K-wires) utilized as joysticks. The fragments are manipulated into anatomic alignment, focusing on restoring the articular congruity and the normal valgus tilt of the radial neck. Once reduced, the fragments are provisionally stabilized with smooth K-wires or a pointed reduction forceps.
Implant Selection and Fixation Strategies
The choice of fixation depends entirely on the fracture morphology.
Isolated Partial Articular Fractures (Mason II):
These are optimally stabilized using headless compression screws or countersunk mini-fragment cortical screws. The screws are placed perpendicular to the fracture plane to maximize interfragmentary compression. It is imperative that the screw heads are buried beneath the subchondral bone to prevent catastrophic abrasive wear on the capitellar articular cartilage.

Neck Fractures and Complex Comminution:
Fractures involving the radial neck or exhibiting significant comminution require plate osteosynthesis. Low-profile, pre-contoured radial head plates are utilized. The plate must be positioned strictly within the safe zone to prevent impingement on the lesser sigmoid notch during pronosupination.

During plate application, the proximal screws must capture the radial head fragments without penetrating the far articular cortex. Locking screws provide angular stability, which is particularly beneficial in osteopenic bone or when addressing severe metaphyseal comminution. Non-locking screws may be used to draw the bone
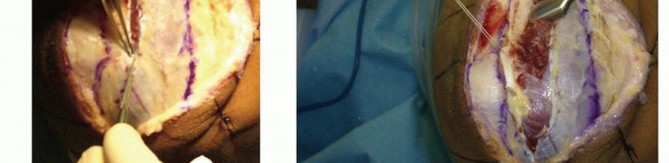
Clinical & Radiographic Imaging





You Might Also Like