Comprehensive Management of Congenital Hand Anomalies: Metacarpal Lengthening and Radial Dysplasia

Key Takeaway
Metacarpal lengthening and radial clubhand reconstruction require meticulous surgical planning. This guide details the biomechanics, indications, and operative techniques for distraction osteogenesis in metacarpal deficiencies, alongside the comprehensive management of radial longitudinal dysplasia. Emphasizing Heikel’s classification and centralization procedures, it provides orthopedic surgeons with evidence-based protocols to optimize functional and cosmetic outcomes in complex congenital hand anomalies.
Introduction to Congenital Hand Anomalies
The management of congenital hand anomalies demands a profound understanding of embryology, pathoanatomy, and the biomechanical principles of the upper extremity. Conditions such as transverse metacarpal deficiencies, phocomelia, and radial longitudinal deficiency (radial clubhand) present unique reconstructive challenges. The primary goal of surgical intervention is to maximize functional independence, achieve stable articulation, and, when possible, improve cosmesis. This masterclass delineates the evidence-based protocols, surgical techniques, and postoperative management strategies for these complex deformities.
Metacarpal Lengthening via Distraction Osteogenesis
Metacarpal lengthening is a highly specialized procedure primarily reserved for transverse deficiencies at the level of the metacarpophalangeal (MCP) joints. It is most frequently indicated in children who possess at least one remaining functional digit, allowing for the restoration of a functional pinch or grasp.
First described by Matev in 1967, the technique utilizes the principles of distraction osteogenesis—gradual mechanical distraction of a healing osteotomy to generate new bone (regenerate), followed by structural bone grafting if necessary. While initially developed for the deficient thumb, its application has expanded to include the congenital absence of fingers.
Indications and Patient Selection
Patient selection is the most critical determinant of success. The procedure requires immense clinical judgment and should only be performed by surgeons intimately familiar with the psychological needs of the pediatric patient and the rigorous demands of the postoperative protocol.
- Optimal Age: The procedure is best performed in patients between the ages of 5 and 11 years. At this stage, the bone possesses robust osteogenic potential, and the child is mature enough to cooperate with the distraction apparatus.
- Expected Outcomes: An average length gain of 4 to 5 cm can be achieved. However, surgeons must counsel parents that while length is gained, normal function and perfect cosmesis are rarely fully realized. The primary objective is functional opposition and grasp.
Surgical Warning: Metacarpal lengthening is contraindicated in patients with severe non-compliance, active local infection, or inadequate soft-tissue envelopes that cannot accommodate the expanding skeletal framework.
Biomechanics and Preoperative Planning
The biomechanics of distraction osteogenesis rely on the tension-stress effect described by Ilizarov. Gradual traction stimulates metabolic activation and cellular proliferation within the osteotomy gap. Ilizarov and colleagues demonstrated that utilizing a specialized distraction/fixation apparatus yields superior gains in length and function by providing rigid stability while allowing precise, controlled distraction.
Surgical Technique (Kessler et al.)
The surgical approach must meticulously preserve the periosteal blood supply to ensure robust regenerate formation.
- Preparation and Positioning: The procedure is performed under general anesthesia with strict tourniquet control to ensure a bloodless field. The arm is prepped and draped in a standard sterile fashion.
- Incision: Make longitudinal dorsal incisions directly over or between the metacarpals targeted for lengthening. Care must be taken to protect the dorsal sensory branches of the radial and ulnar nerves, as well as the extensor venous network.
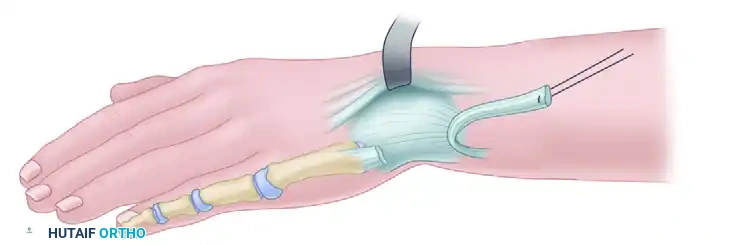
- Hardware Placement: Insert two smooth or threaded Kirschner wires (or specialized half-pins) transversely through the skin and the metacarpal diaphysis. One set of wires is placed proximal to the planned osteotomy site, and the second set is placed distally.
- Osteotomy: Perform a precise, low-energy transverse or slightly oblique osteotomy of the appropriate metacarpal between the pin clusters. A Gigli saw, multiple drill holes connected with an osteotome, or a cooled oscillating saw may be used to prevent thermal necrosis.
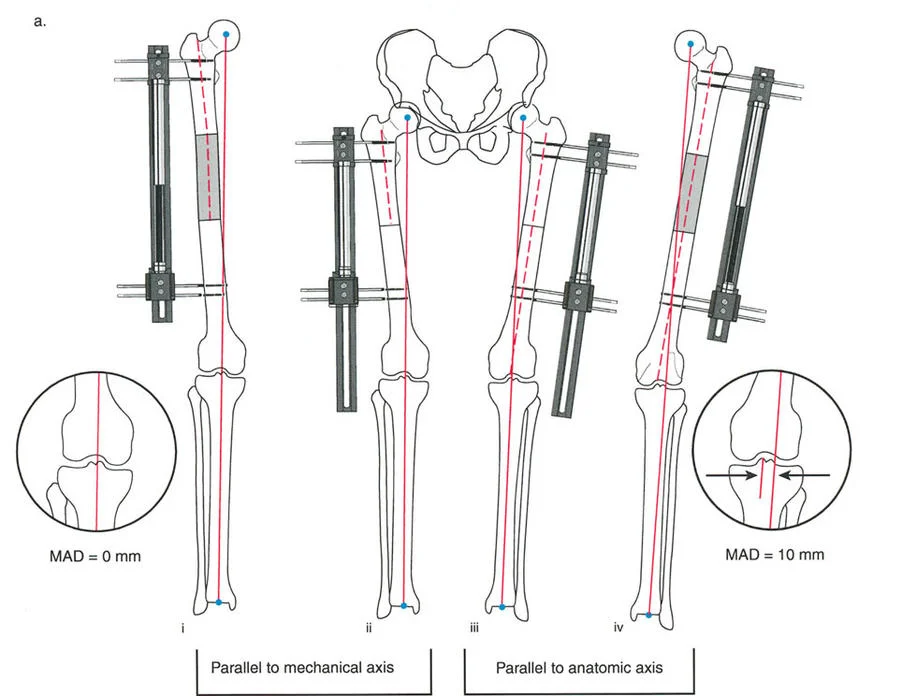
- Apparatus Application: Close the incisions in a routine, tension-free manner. Apply the external distraction apparatus to the pins, ensuring it is parallel to the longitudinal axis of the metacarpal to prevent angular deformity during lengthening.
Postoperative Protocol and Distraction Phase
- Latency Period: The hand is elevated continuously for 48 to 72 hours postoperatively to minimize edema. Distraction does not begin immediately; a latency period of 5 to 7 days is observed to allow the initial fracture hematoma to organize into a fibrovascular callus.
- Distraction Rate: Distraction is initiated at a strict rate of 1.0 mm per day, typically divided into four 0.25 mm increments. This rate optimizes osteogenesis while preventing premature consolidation (if too slow) or nonunion/ischemia (if too fast).
- Monitoring: The distraction process should be painless. Distraction must be terminated immediately at any sign of vascular compromise, severe pain, or neurological impairment.
- Consolidation and Grafting: Once the maximal safe lengthening is achieved, the apparatus is locked. If the regenerate bone is insufficient or if the gap is excessively large, secondary autologous bone grafting (typically from the iliac crest) is performed to bridge the defect and ensure structural integrity.
Complications and Pitfalls
Complications are frequent and require vigilant management:
* Pin Track Infection: The most common complication. Managed with aggressive local pin care and oral antibiotics.
* Neurovascular Compromise: Caused by excessive tension on the neurovascular bundles. Requires immediate cessation or slight reversal of distraction.
* Distal Ulcerations: Result from tight soft tissues failing to expand at the rate of the bone.
* Joint Contractures: Prophylactic splinting and aggressive hand therapy are mandatory to maintain adjacent joint mobility.
Phocomelia: Classification and Management
Phocomelia is a rare congenital anomaly characterized by the severe underdevelopment or absence of the proximal limb segments, with the hand or digits attaching directly to the trunk.
Frantz and O’Rahilly Classification
The anatomical variations of phocomelia are classified into three distinct types by Frantz and O’Rahilly:
* Type A (Complete): The hand is attached directly to the shoulder with no intermediate humeral or forearm segment.
* Type B (Proximal): The hand is attached to the shoulder with an abnormal, fused, or severely hypoplastic humeral, radial, and ulnar segment intervening.
* Type C (Distal): The hand is attached to the shoulder with an intervening humeral segment, but a complete absence of the forearm segment.
Clinical Presentation and Treatment Strategies
Patients with phocomelia exhibit profound functional limitations. The scapula is often laterally deficient, making active abduction difficult—usually achieved only by a sudden, jerking motion. The hand typically possesses only three or four digits, and the thumb is almost universally absent. As the child grows and the chest widens, the ability to reach the midline, mouth, and genitalia becomes increasingly compromised, leading to significant psychological and functional impairment.
Treatment is overwhelmingly conservative.
* Assistive Devices: Ingenious adaptive devices for hygiene, feeding, and dressing play a paramount role in achieving independence.
* Prosthetics: Conventional prostheses designed to increase limb length are frequently rejected by patients due to the loss of tactile sensation and the heavy, cumbersome nature of the devices.
* Surgical Role: Surgery plays a very minor role and is generally reserved for severe shoulder instability, extreme limb shortening, or inadequate thumb opposition. Rotational osteotomy of a digit combined with web space deepening may occasionally improve opposition, though outcomes remain unpredictable.
Radial Clubhand (Radial Longitudinal Deficiency)
Radial ray deficiencies encompass a spectrum of malformations characterized by the longitudinal failure of formation along the preaxial (radial) border of the upper extremity. This includes deficient thenar muscles, a hypoplastic or absent thumb, and a shortened or absent radius.
Epidemiology and Syndromic Associations
Radial clubhand occurs in approximately 1 per 100,000 live births. It is bilateral in 50% of cases; when unilateral, the right side is more frequently affected. Both sexes are equally predisposed. Complete absence of the radius is far more common than partial absence.
While many cases are sporadic, radial dysplasia is notoriously associated with severe systemic syndromes. A multidisciplinary approach is mandatory to rule out life-threatening anomalies before any orthopedic intervention.
Clinical Pearl: Approximately 25% of patients with radial clubhand have associated cardiac, hematopoietic, gastrointestinal, or renal abnormalities. These pose significant morbidity and mortality risks.
- Holt-Oram Syndrome: Autosomal dominant. Associated with cardiac septal defects (most commonly ASD). Cardiac correction must precede limb reconstruction.
- Fanconi Anemia: Autosomal recessive. A fatal pancytopenia of early childhood. A chromosomal breakage challenge test is mandatory for early detection. Prognosis is extremely poor without bone marrow transplantation.
- TAR Syndrome (Thrombocytopenia-Absent Radius): Autosomal recessive. Characterized by absent radii but thumbs are always present (though lacking extension). Thrombocytopenia usually resolves by age 4 to 5 years and is not an absolute contraindication to delayed surgery.
- VACTERL Association: Vertebral defects, Anal atresia, Cardiac malformations, Tracheoesophageal fistula, Renal abnormalities, and Limb anomalies.
Pathoanatomy and Biomechanics
The anatomical derangement in radial clubhand is extensive:
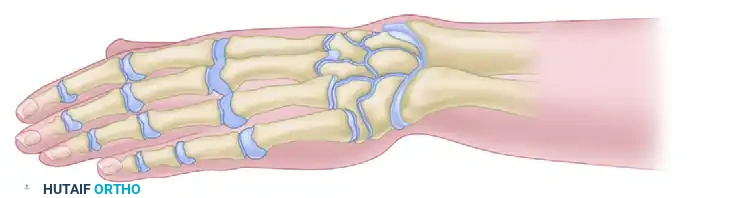
* Osteology: The ulna is characteristically short (50-75% of normal length), thick, and bowed toward the radius. The scaphoid and trapezium are absent in >50% of patients. The thumb is absent in >80% of cases.
* Musculature: The long head of the biceps, brachialis, brachioradialis, and pronator teres are frequently absent or severely hypoplastic. The flexor digitorum superficialis is usually present but abnormal.
* Neurology: The median nerve is anomalous, thicker than normal, and runs superficially along the preaxial border of the forearm. Flatt famously described it as a "strong and unyielding bowstring" of the radially bowed hand. It is at extreme risk during surgical dissection. The radial nerve frequently terminates at the lateral epicondyle.
* Vascularity: The radial artery is almost universally absent. The hand is perfused by a normal ulnar artery and a well-developed common interosseous artery.



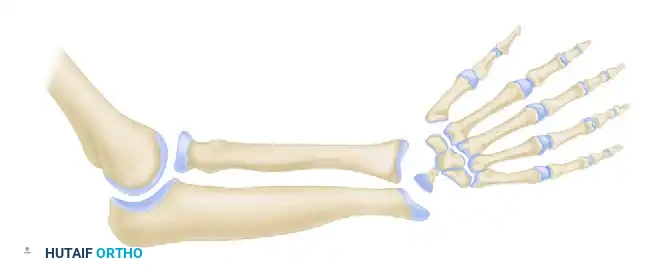
Heikel’s Classification of Radial Dysplasia
The currently accepted classification system is Heikel’s modification, which categorizes the deformity into four types based on radiographic appearance:
-
Type I (Short Distal Radius): The distal radial physis is present but delayed. The radius is only slightly shortened, and the ulna is not bowed. Radial support to the carpus is maintained.
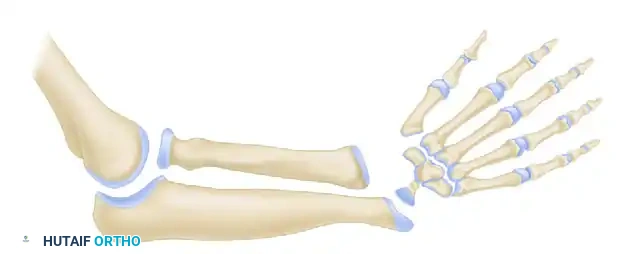
-
Type II (Hypoplastic Radius): Both distal and proximal radial physes are present but delayed. This results in moderate shortening of the radius and secondary thickening and bowing of the ulna.
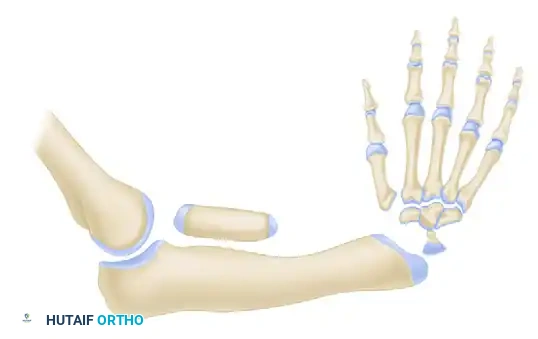
-
Type III (Partial Absence of the Radius): Absence may be proximal, middle, or distal (distal third absence is most common). The carpus is radially deviated and unsupported. The ulna is thickened and bowed.
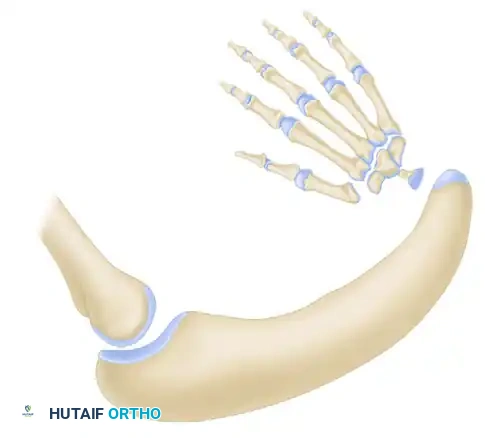
-
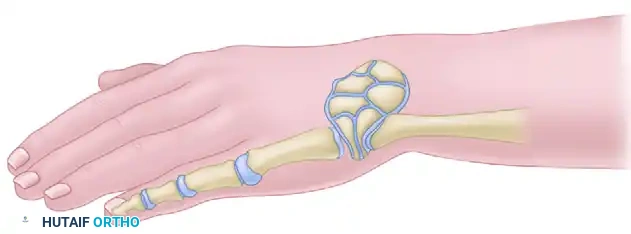
Type IV (Total Absence of the Radius): The most common pattern. Features total absence of the radius, severe radial deviation of the carpus, palmar and proximal subluxation, frequent pseudoarticulation with the radial border of the distal ulna, and a severely shortened, bowed ulna.

Non-Operative Management
Treatment begins immediately after birth. The goal of conservative therapy is to stretch the contracted radial soft tissues and passively correct the carpal subluxation over the distal ulna.
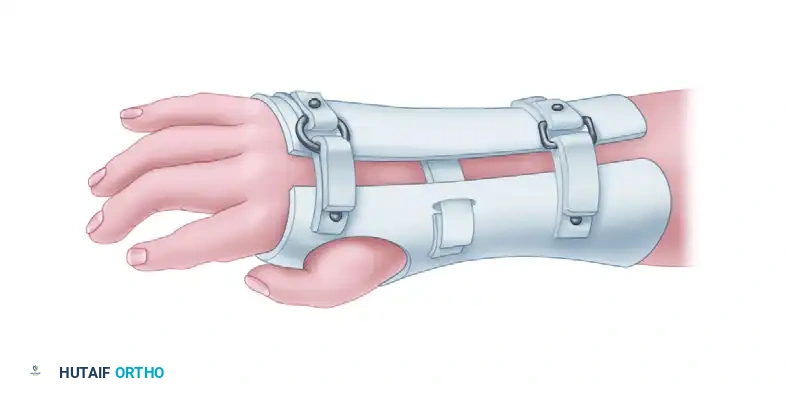
- Serial Casting: Initiated as soon as possible. The cast is applied in three stages (similar to clubfoot casting): correcting the hand and wrist first, followed by the elbow.
- Splinting: As the child grows, custom thermoplastic splints are utilized to maintain alignment. However, as ulnar growth continues, splinting alone becomes inadequate to maintain correction in severe types (III and IV).
Operative Treatment: Centralization of the Carpus
Surgery is indicated for children with inadequate radial support of the carpus (Types III and IV) who have adequate elbow flexion.
Surgical Warning: Centralization is strictly contraindicated in patients with stiff elbows in extension. If the elbow cannot flex, a centralized, straight wrist will prevent the patient from reaching their mouth, devastating their ability to feed themselves.
- Timing: Centralization is optimally performed between 3 to 6 months of age. This allows the child to grow large enough to tolerate anesthesia and for the anatomical structures to be easily identifiable, but early enough to prevent irreversible soft-tissue contractures. Pollicization (thumb reconstruction) follows at 9 to 12 months.
Surgical Approaches and Techniques
The modern centralization technique evolved from Sayre (1893) and Lidge, focusing on placing the carpus squarely over the distal ulna without destroying the ulnar physis.
- Incision: Various incisions are utilized. Manske and McCarroll advocate for transverse ulnar incisions with the removal of an ellipse of redundant skin. Alternatively, a bilobed or Z-plasty approach over the radial aspect can be used to release the tight radial band.
- Soft Tissue Release: The tight radial structures (fibro-osseous anlage, contracted fascia) must be radically excised. The anomalous, superficial median nerve must be meticulously identified and protected.
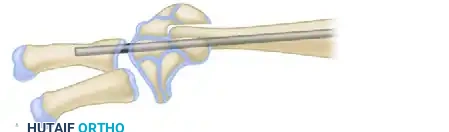
- Carpal Preparation: A notch is surgically created in the central carpus (typically excising the lunate or capitate) to accept the distal ulna. The ulnar articular cartilage is preserved to maintain growth potential.
- Skeletal Fixation: The hand is centralized over the ulna. A stout Kirschner wire or Steinmann pin is driven retrogradely through the carpus and third metacarpal, and then antegrade down the medullary canal of the ulna to hold the reduction.
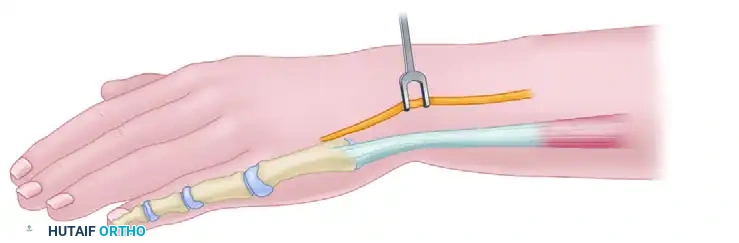
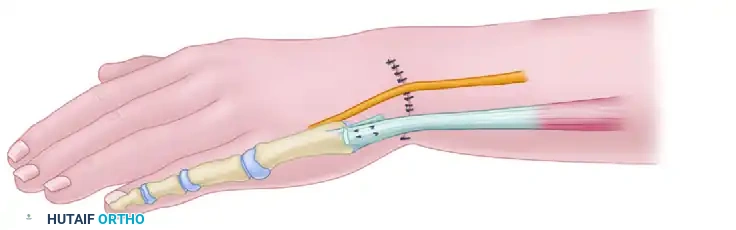
- Tendon Transfers: To maintain the centralized position dynamically, the extensor carpi ulnaris (ECU) or flexor carpi ulnaris (FCU) may be advanced or transferred to the dorsal-ulnar aspect of the carpus.
- Ulnar Osteotomy: If the ulnar bowing exceeds 30 degrees, a concurrent closing wedge osteotomy of the ulna may be required to allow straight intramedullary pin placement and correct the mechanical axis.
Postoperative Care and Long-Term Outcomes
Postoperatively, the limb is immobilized in a long-arm cast for 6 to 8 weeks. The intramedullary pin is often left in place for several months to a year to act as an internal splint, preventing early recurrence of the radial deviation.
Despite meticulous surgical technique, recurrence of radial deviation is the most common long-term complication, often necessitating revision surgery or radialization procedures. Furthermore, parents must be educated that the centralized limb will never achieve normal length, as the ulnar growth plate remains inherently abnormal. However, successful centralization dramatically improves the mechanical advantage of the extrinsic flexors and extensors, providing the child with a functional, cosmetically acceptable limb capable of independent activities of daily living.
📚 Medical References
You Might Also Like