Operative Management of Acetabular and Pelvic Fractures: A Comprehensive Surgical Masterclass

Key Takeaway
Acetabular and pelvic fractures present complex reconstructive challenges requiring profound anatomical knowledge and meticulous surgical execution. This guide details the Letournel and Judet two-column classification, critical radiographic landmarks, and step-by-step surgical approaches. Emphasizing concentric reduction of the femoral head beneath the anatomical dome, it provides orthopedic surgeons with evidence-based protocols for managing neurovascular risks, optimizing patient positioning, and achieving stable internal fixation to ensure optimal long-term functional outcomes.
FRACTURES OF THE ACETABULUM AND PELVIS: PRINCIPLES AND OPERATIVE MANAGEMENT
The management of acetabular and pelvic ring fractures represents one of the most formidable challenges in orthopedic trauma surgery. These injuries typically result from high-energy mechanisms, such as motor vehicle collisions or falls from significant heights, and are frequently associated with life-threatening polytrauma. The primary objective in treating acetabular fractures is the anatomical restoration of the articular surface to prevent post-traumatic osteoarthritis, while pelvic ring injuries require the restoration of mechanical stability to allow early mobilization.
This comprehensive guide delineates the intricate osteology, neurovascular hazards, radiographic evaluation, classification, and step-by-step surgical management of these complex fractures, adhering to the foundational principles established by Emile Letournel and Robert Judet.
ANATOMY AND BIOMECHANICS: THE TWO-COLUMN CONCEPT
The acetabulum is a complex, hemispherical articular socket situated at the confluence of the ilium, ischium, and pubis. It is composed of a horseshoe-shaped articular surface surrounding the nonarticular cotyloid fossa. To conceptualize the biomechanics and fracture patterns of this region, Letournel and Judet described the acetabulum as being supported by two distinct columns of bone, forming an inverted "Y".


The Anterior Column:
The anterior column extends from the anterior iliac crest down to the pubic symphysis. It comprises the anterior half of the iliac wing, the anterior superior and inferior iliac spines, the anterior half of the acetabular articular surface, and the superior and inferior pubic rami.
The Posterior Column:
The posterior column is a massive, dense strut of bone designed to withstand the primary vectors of weight-bearing. It includes the ischial tuberosity, the ischial spine, the posterior half of the acetabulum, and the dense bone forming the greater and lesser sciatic notches. The shorter posterior column terminates at its intersection with the anterior column at the apex of the sciatic notch.



The Acetabular Dome and Quadrilateral Surface:
The dome, or roof, of the acetabulum is the critical weight-bearing portion of the articular surface that supports the femoral head. Anatomical restoration of the dome with concentric reduction of the femoral head beneath it is the paramount goal of both operative and nonoperative treatment.

Medial to the acetabulum lies the quadrilateral surface, a flat plate of bone forming the lateral border of the true pelvic cavity. Anteriorly, the iliopectineal eminence lies directly over the femoral head. Both the quadrilateral surface and the iliopectineal eminence are structurally thin, severely limiting the types of internal fixation (e.g., screw length and trajectory) that can be safely utilized in these regions without breaching the joint space.


Clinical Pearl: The column concept is not merely an anatomical descriptor; it is the foundation of fracture classification, the selection of surgical approaches, and the strategic placement of reconstruction plates and lag screws.
APPLIED NEUROVASCULAR ANATOMY AND SURGICAL HAZARDS
The pelvis houses critical neurovascular structures that are at high risk during both the initial traumatic event and subsequent surgical interventions. Surgical approaches must be meticulously designed and executed to navigate these hazards.
The Sciatic Nerve and Superior Gluteal Vessels:
The sciatic nerve exits the pelvis through the greater sciatic notch, typically passing inferior to the piriformis muscle. It is highly susceptible to injury in posterior fracture-dislocations of the hip and fractures with significant posterior displacement.
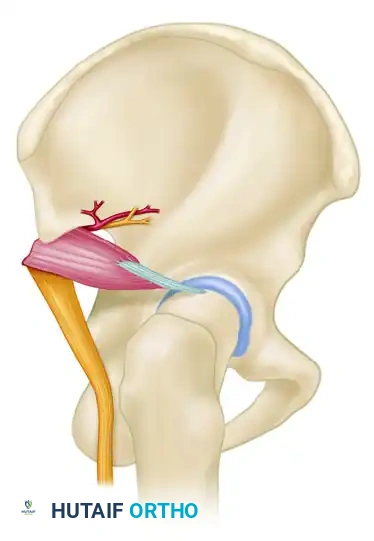
The superior gluteal artery and nerve exit the greater sciatic notch at its most superior aspect, tethered to the bone by variable fascial attachments. Fractures extending into the superior portion of the greater sciatic notch can cause massive hemorrhage from the superior gluteal artery, occasionally necessitating preoperative angiography and embolization.
Surgical Warning: The function of both the tibial and common peroneal divisions of the sciatic nerve must be rigorously documented in the emergency department, immediately following closed reduction of a hip dislocation, and postoperatively. Iatrogenic injury during the Kocher-Langenbeck approach is a devastating complication, often resulting from excessive retractor tension.
The Corona Mortis:
During anterior approaches (e.g., Ilioinguinal or modified Stoppa), the surgeon must be acutely aware of the corona mortis (crown of death). This is a variable, often large, arterial and/or venous anastomosis between the external iliac (or inferior epigastric) system and the obturator system, passing over the superior pubic ramus.
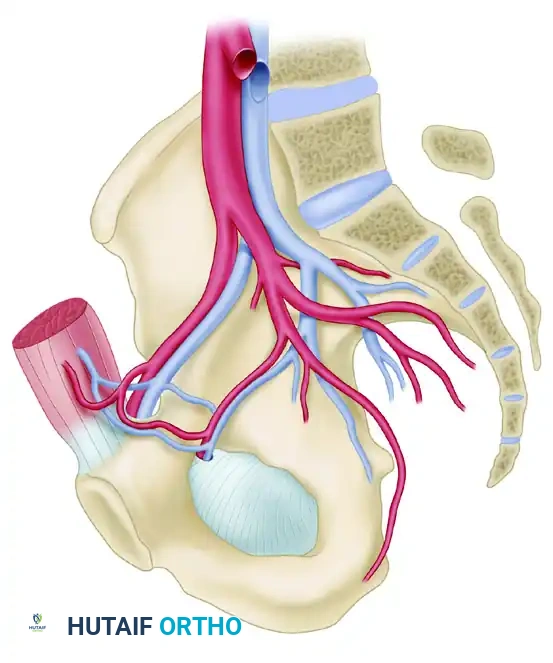
Failure to identify and ligate this vascular connection can lead to catastrophic hemorrhage that retracts into the true pelvis, making hemostasis exceedingly difficult.
RADIOGRAPHIC EVALUATION
Accurate classification and preoperative planning rely on a standardized radiographic series, supplemented universally in modern practice by fine-cut Computed Tomography (CT) with 3D reconstructions.
The Standard Radiographic Series:
The evaluation begins with an Anteroposterior (AP) view of the pelvis, followed by the two Judet oblique views (Obturator Oblique and Iliac Oblique), taken at 45-degree angles.
Six fundamental radiographic landmarks must be identified on the AP radiograph to understand the fracture pattern:
1. Iliopectineal Line: Represents the anterior column.
2. Ilioischial Line: Represents the posterior column.
3. Radiographic Teardrop: Represents the medial wall of the acetabulum (anterior-inferior portion of the quadrilateral surface).
4. Roof of the Acetabulum: The superior weight-bearing dome.
5. Anterior Lip (Wall) of the Acetabulum.
6. Posterior Lip (Wall) of the Acetabulum.
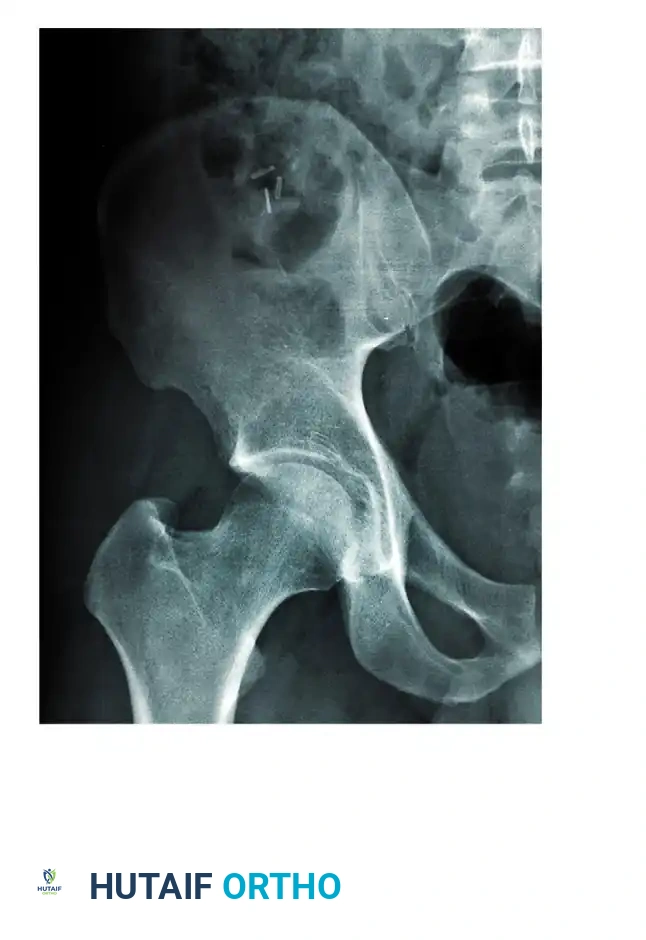
Fractures traversing the anterior column disrupt the iliopectineal line, whereas posterior column fractures disrupt the ilioischial line.
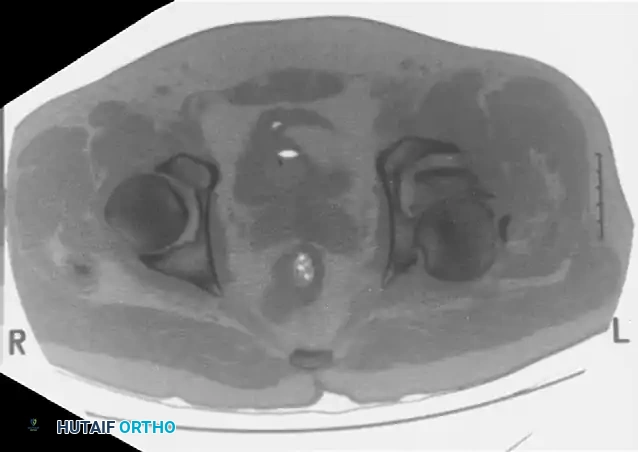
Computed Tomography (CT):
CT scanning is mandatory. It defines the size of wall fragments, the presence of intra-articular loose bodies, marginal impaction, and the exact orientation of fracture lines. CT is particularly critical in identifying incarcerated fragments that block closed reduction of a dislocated hip.


CLASSIFICATION OF ACETABULAR FRACTURES
The Letournel and Judet classification remains the gold standard, dividing fractures into five elementary and five associated patterns based on the two-column concept.
Elementary Fractures:
1. Posterior Wall (Most common)
2. Posterior Column
3. Anterior Wall
4. Anterior Column
5. Transverse (Divides the innominate bone into superior and inferior halves)
Associated Fractures:
1. Posterior Column + Posterior Wall
2. Transverse + Posterior Wall
3. T-Shaped (Transverse fracture with a vertical split through the obturator ring)
4. Anterior Column/Wall + Posterior Hemitransverse
5. Both-Column (The defining feature is that no portion of the articular surface remains attached to the intact axial skeleton; the "spur sign" is pathognomonic).
INDICATIONS FOR TREATMENT
Indications for Nonoperative Treatment
Nonoperative management is reserved for a highly select group of patients. Strict criteria must be met to ensure the femoral head remains concentrically reduced beneath an intact weight-bearing dome.
* Minimal Displacement: Fracture displacement less than 2 mm.
* Intact Roof Arc Angles: Matta described roof arc angles (measured on AP, obturator oblique, and iliac oblique views). Angles >45 degrees indicate the fracture exits outside the critical weight-bearing zone.
* Secondary Congruence: Seen in certain both-column fractures where the fragments settle concentrically around the femoral head.
* Medical Comorbidities: Patients whose physiological status precludes major reconstructive surgery.
Indications for Operative Treatment
Operative intervention is the standard of care for the majority of displaced acetabular fractures to prevent rapid-onset post-traumatic arthritis.
* Displacement: >2 mm of displacement within the articular weight-bearing dome.
* Instability: Posterior wall fractures involving >20% of the articular surface, or those demonstrating dynamic instability on fluoroscopic stress examination.
* Incongruency: Any non-concentric reduction of the femoral head.
* Intra-articular Pathology: Incarcerated osteochondral fragments or soft tissue blocking reduction.
* Irreducible Dislocations: Requiring emergent open reduction and internal fixation (ORIF).
SURGICAL APPROACHES AND STEP-BY-STEP TECHNIQUES
The choice of surgical approach is dictated entirely by the fracture pattern. The goal is to visualize the primary displacement and apply direct reduction techniques.
1. The Kocher-Langenbeck Approach
Indications: Posterior wall, posterior column, and certain transverse or T-shaped fractures with predominant posterior displacement.
Positioning: Prone or lateral decubitus on a radiolucent table. The knee must be flexed to 90 degrees to relax the sciatic nerve.
Step-by-Step Execution:
1. Incision: Centered over the greater trochanter, extending proximally toward the PSIS and distally along the femoral shaft.
2. Superficial Dissection: Split the gluteus maximus bluntly in line with its fibers. Incise the fascia lata distally.
3. Deep Dissection: Identify the sciatic nerve. Isolate and tag the piriformis and the short external rotators (obturator internus and gemelli).
4. Exposure: Transect the short external rotators near their femoral insertion and reflect them posteriorly over the sciatic nerve. This acts as a protective cushion for the nerve.
5. Capsulotomy: If a posterior wall fracture is present, the capsule is often already torn. Preserve the labrum.
6. Reduction & Fixation: Clean the fracture site of hematoma and debris. Reduce the posterior column using Schanz pins in the ischium as joysticks, or use pelvic reduction forceps. Fix with a 3.5mm pelvic reconstruction plate spanning from the ischium to the intact ilium. Posterior wall fragments are reduced and fixed with lag screws and a buttress plate.
Pitfall: Avoid placing retractors directly into the greater sciatic notch without direct visualization, as this can compress the sciatic nerve or avulse the superior gluteal vessels.
2. The Ilioinguinal Approach
Indications: Anterior column, anterior wall, and anterior column + posterior hemitransverse fractures.
Positioning: Supine on a radiolucent table.
Step-by-Step Execution:
1. Incision: Extends from the pubic symphysis, along the inguinal ligament, to the anterior superior iliac spine (ASIS), and posteriorly along the iliac crest.
2. Windows: The approach utilizes three distinct surgical windows to access the internal pelvis without detaching the inguinal ligament.
* Lateral Window: Between the iliac crest and the iliopsoas muscle/femoral nerve. Provides access to the internal iliac fossa and SI joint.
* Middle Window: Between the iliopsoas/femoral nerve laterally and the external iliac vessels medially. Provides access to the pelvic brim and quadrilateral surface.
* Medial Window: Medial to the external iliac vessels and lateral to the rectus abdominis. Provides access to the superior pubic ramus and symphysis.
3. Vascular Control: The external iliac vessels must be carefully mobilized with vessel loops. The corona mortis must be identified and ligated in the medial window.
4. Reduction & Fixation: Reduction is achieved using specialized asymmetric pelvic reduction forceps (e.g., Jungbluth forceps). Fixation is typically achieved with long 3.5mm lag screws down the anterior column and a reconstruction plate along the pelvic brim.
3. The Modified Stoppa Approach
Indications: Increasingly used as an alternative or adjunct to the ilioinguinal approach for anterior fractures, particularly those with significant medial displacement of the quadrilateral surface.
Technique: A transverse Pfannenstiel incision is made. The rectus abdominis is split linearly, and the dissection proceeds extraperitoneally along the pelvic brim. This provides excellent direct visualization of the quadrilateral surface and allows for the placement of infra-pectineal buttress plates to prevent medial subluxation of the femoral head.
POSTOPERATIVE CARE AND REHABILITATION
The success of acetabular fracture surgery relies heavily on strict postoperative protocols.
- Weight-Bearing Status: Patients are restricted to toe-touch weight-bearing (TTWB) or flat-foot weight-bearing (approx. 20 lbs) on the operative extremity for 8 to 12 weeks, depending on radiographic evidence of healing.
- Deep Vein Thrombosis (DVT) Prophylaxis: Pelvic trauma carries an exceptionally high risk of venous thromboembolism. Chemical prophylaxis (e.g., Low Molecular Weight Heparin) is mandatory for a minimum of 4 weeks postoperatively, barring contraindications. Mechanical prophylaxis (SCDs) should be used continuously while in the hospital.
- Heterotopic Ossification (HO) Prophylaxis: The Kocher-Langenbeck and extensile approaches carry a high risk of HO. Prophylaxis with Indomethacin (75mg SR daily for 3-6 weeks) or single-dose localized radiation therapy (700-800 cGy within 72 hours of surgery) is highly recommended.
- Physical Therapy: Early passive and active-assisted range of motion (ROM) of the hip, knee, and ankle is initiated on postoperative day one to nourish the articular cartilage and prevent stiffness.
OUTCOMES AND COMPLICATIONS
The most critical determinant of long-term outcome is the accuracy of the surgical reduction. Anatomical reduction (0-1 mm step-off) yields good to excellent clinical results in 80-90% of cases.
Complications include:
* Post-Traumatic Osteoarthritis: The most common late complication, occurring in up to 20% of anatomically reduced fractures and >80% of poorly reduced fractures. May eventually necessitate Total Hip Arthroplasty (THA).
* Avascular Necrosis (AVN) of the Femoral Head: Occurs in 2-10% of cases, most frequently associated with posterior fracture-dislocations.
* Sciatic Nerve Palsy: Iatrogenic injury occurs in 2-8% of posterior approaches. The peroneal division is most susceptible. Recovery is variable and often incomplete.
* Infection: Deep surgical site infections occur in 1-5% of cases, requiring aggressive surgical debridement and targeted intravenous antibiotic therapy.
CONCLUSION
The operative management of acetabular and pelvic fractures demands a profound understanding of complex three-dimensional anatomy, meticulous preoperative planning, and precise surgical execution. By adhering to the biomechanical principles of the two-column concept, respecting neurovascular boundaries, and striving for absolute articular congruity, the orthopedic surgeon can optimize functional recovery and mitigate the devastating sequelae of post-traumatic arthritis in this challenging patient population.
You Might Also Like

