Comprehensive Management of Tibia Vara (Blount Disease)
Key Takeaway
Tibia vara, or Blount disease, is an acquired disorder of the proximal tibial metaphysis characterized by progressive varus, internal tibial torsion, and genu recurvatum. Driven by asymmetrical compressive shear forces across the medial physis, it is classified into infantile and adolescent forms. Management ranges from bracing in early stages to complex proximal tibial osteotomies and medial plateau elevation for advanced Langenskiöld stages to restore the mechanical axis.
Introduction and Pathophysiology
Erlacher is credited with the first description of tibia vara and internal tibial torsion in 1922, but it was Walter Blount’s seminal article in 1937 that prompted widespread recognition of this complex disorder. Blount originally described tibia vara as an osteochondrosis similar to coxa plana or Madelung’s deformity, localized to the medial aspect of the proximal tibial epiphysis. However, contemporary orthopedic consensus defines tibia vara as an acquired disease of the proximal tibial metaphysis, characterized by disordered enchondral ossification rather than a true epiphyseal dysplasia or osteochondrosis.
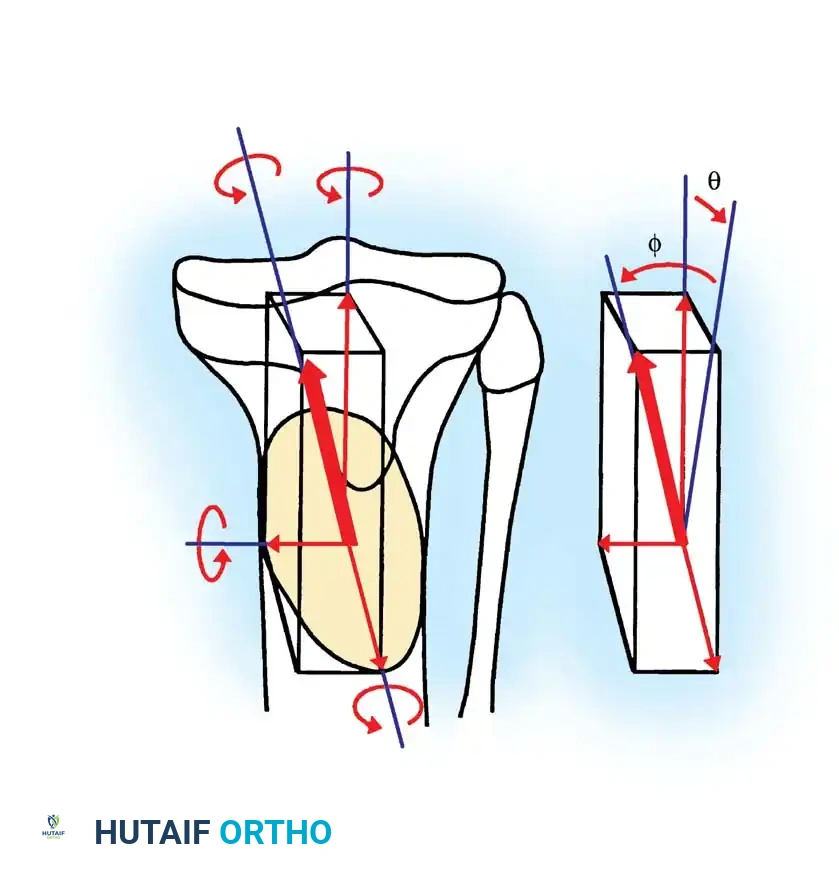
The exact etiology remains multifactorial, combining hereditary predisposition, developmental factors, and mechanical overload. The pathogenesis is heavily driven by the Hueter-Volkmann principle, which dictates that excessive compressive forces across a physis inhibit growth. Weight-bearing is an absolute prerequisite for the development of Blount disease; it does not occur in nonambulatory patients. The relationship between early walking, childhood obesity, and the onset of tibia vara has been clearly documented. Asymmetrical compressive shear forces across the proximal medial tibial physis promote disruption, causing compression and deviation of normal intercondylar ossification.
Clinical Pearl: The classic triad of Blount disease includes varus angulation, internal tibial torsion, and genu recurvatum. Recognition of the rotational and sagittal plane deformities is critical, as isolated coronal plane correction will lead to suboptimal functional outcomes.
Classification of Blount Disease
Blount distinguished two primary types of tibia vara based on the age of onset. Although the exact cause remains controversial, the clinical and radiographic findings within these cohorts are highly consistent.
Infantile Tibia Vara
The infantile form begins before 8 years of age and is notoriously difficult to differentiate from physiological bowing, especially in children younger than 2 years. Infantile tibia vara is bilateral and symmetrical in approximately 60% of affected children, whereas physiological bowing is almost universally bilateral. The critical distinction lies in the natural history: in Blount disease, the varus deformity increases progressively, whereas physiological bowing tends to resolve spontaneously with growth.
Adolescent (Late-Onset) Tibia Vara
Adolescent Blount disease begins after 8 years of age but before skeletal maturity. It is less common than the infantile form and is subdivided into two distinct etiologic categories:
1. Post-Traumatic/Infectious: Occurring between ages 8 and 13 years, caused by partial closure of the medial physis secondary to trauma or infection.
2. Idiopathic Late-Onset: Occurring predominantly in obese children, particularly of African descent, between ages 8 and 13 without a distinct inciting event.
Histological changes in late-onset tibia vara are markedly similar to those seen in infantile tibia vara and slipped capital femoral epiphysis (SCFE), suggesting a common mechanical etiology. Loder et al. reported that less than half of late-onset cases are bilateral. Patients typically present with knee pain, a gradually progressive genu varum deformity, and an average preoperative tibiofemoral angle of 14 degrees.
Clinical and Radiographic Evaluation
Radiographic Parameters and Staging
Standard radiographic evaluation requires standing, full-length anteroposterior (AP) and lateral radiographs of the lower extremities to accurately assess the mechanical axis.
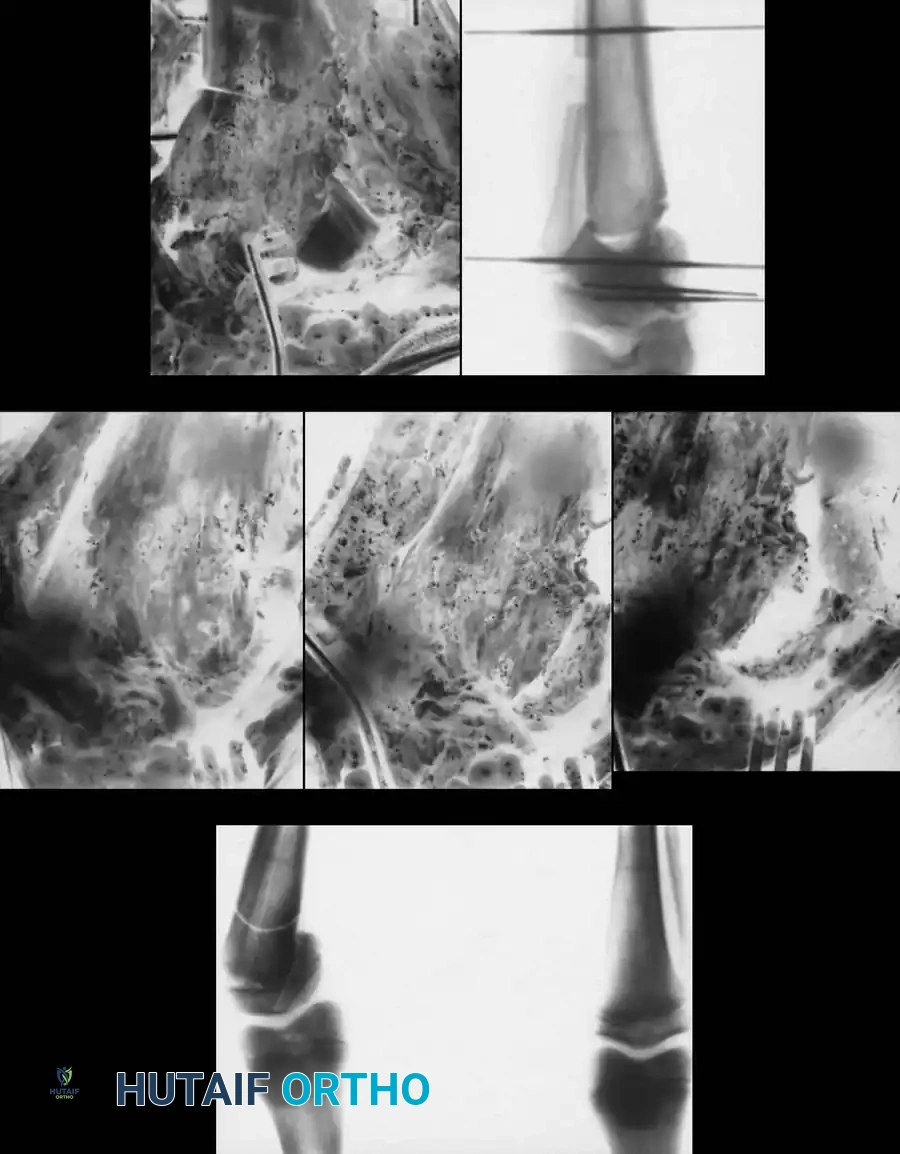
In tibia vara, the medial half of the epiphysis is characteristically short, thin, and wedged. The physis is irregular in contour and slopes medially. The proximal metaphysis forms a distinct medial projection (metaphyseal beak). While this projection is palpable clinically, it is not exclusively diagnostic of tibia vara. However, medial metaphyseal fragmentation is considered pathognomonic for progressive disease.
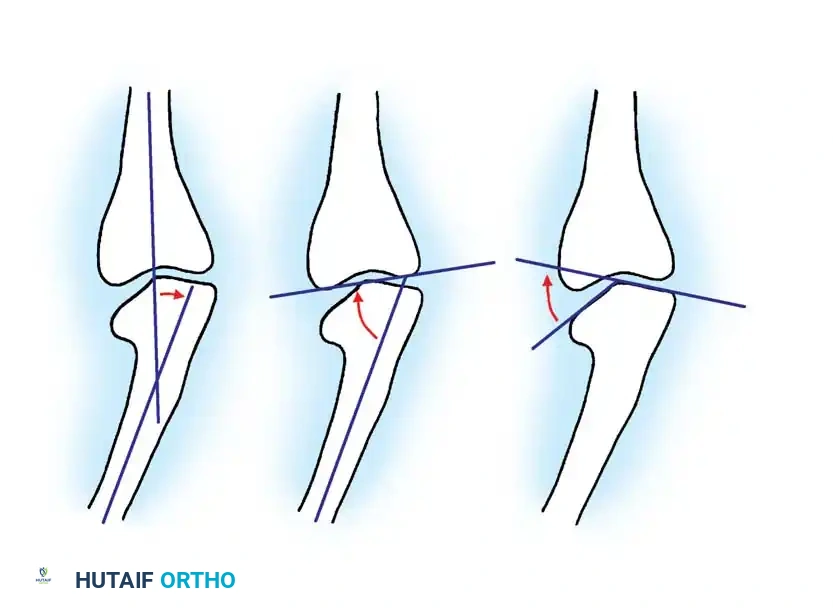
Langenskiöld described the progressive epiphyseal changes and deformity through six distinct stages (Stages I–VI) correlating with growth and development. By Stage VI, the medial portion of the epiphysis fuses at a 90-degree downward angle, representing a severe, irreversible physeal arrest.
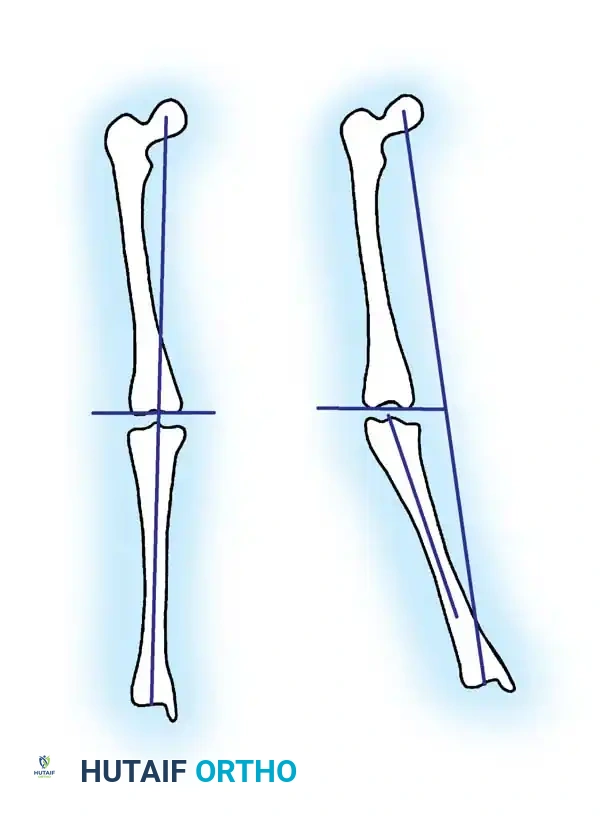
To differentiate infantile Blount disease from physiological bowing, the metaphyseal-diaphyseal angle (Drennan’s angle) is a critical early indicator. Formed by a line drawn perpendicular to the longitudinal axis of the tibia and a line drawn through the two beaks of the metaphysis, an angle of 11 degrees or more is highly predictive of Blount disease. Children with angles less than 11 degrees typically have physiological bowing that resolves with growth.

Diagnostic Warning: Because of internal tibial torsion, Drennan’s angle can be artificially altered by limb rotation during radiography. Ensure the patella is facing strictly forward (true AP of the knee) when obtaining these measurements.

Associated Deformities
Kline et al. identified femoral varus as a significant compensatory deformity in late-onset Blount disease, contributing 34% to 76% of the overall genu varum. This excessive femoral varus must be calculated on standing long-film radiographs and may require simultaneous femoral osteotomy to avoid residual mechanical axis deviation.
Intra-articular pathology is also common. Arthrography and arthrotomy often reveal a hypertrophied medial meniscus and a posteromedial depression of the unossified cartilage of the medial tibial plateau. As the knee flexes, the medial femoral condyle sinks into this posteromedial depression, leading to apparent relaxation of the medial collateral ligament and dynamic instability.

Differential Diagnosis: Focal Fibrocartilaginous Dysplasia
Focal fibrocartilaginous dysplasia is a rare cause of tibia vara that mimics Blount disease. It presents as a unilateral lesion of the proximal medial metaphysis with a characteristic radiographic appearance. Unlike Blount disease, this condition is generally self-limiting and often corrects spontaneously. Severe progression must be definitively documented before any valgus osteotomy is considered.

Non-Operative Management
The treatment of Blount disease is dictated by the patient's age and the severity (Langenskiöld stage) of the deformity.
For children between ages 2 and 5 years with Langenskiöld Stage I or II disease, observation or a trial of bracing (e.g., knee-ankle-foot orthosis [KAFO] locked in extension during weight-bearing) may be indicated. Literature is divided on the efficacy of bracing. Some authors report favorable influences on the natural history of unilateral early-stage disease, while others (Shinohara et al.) found no difference in resolution rates between braced and unbraced patients. If bracing is utilized, close follow-up at 6-month intervals is mandatory. If the deformity persists or progresses beyond age 4, surgical intervention is required.
Surgical Management: Indications and Techniques
Surgical intervention is indicated for progressive deformity, failure of conservative management, or presentation in an older child where spontaneous correction is impossible. The proximal tibial physis has the potential to correct adjacent metaphyseal deformity, but this potential diminishes rapidly with age and advancing Langenskiöld stage.
Timing of Surgery
The age at the time of osteotomy is the single most critical prognostic factor.
* Early Osteotomy (< 4 years): Yields the best results. Up to 88% of children are treated successfully with a single osteotomy. Recurrence rates are low (e.g., 10% or less).
* Late Osteotomy (> 5 years): Associated with unacceptably high recurrence rates. Ferriter and Shapiro reported a 76% recurrence rate in children undergoing osteotomy at 5 years of age or older. Beaty et al. reported an 83% recurrence rate necessitating repeated osteotomies in this older cohort.
Proximal Tibial Valgus Osteotomy
The workhorse procedure for Blount disease is a valgus-producing proximal tibial osteotomy combined with a fibular osteotomy. Mild overcorrection into 5 to 10 degrees of valgus is recommended in young children to accommodate potential recurrence.
Surgical Approaches and Variations:
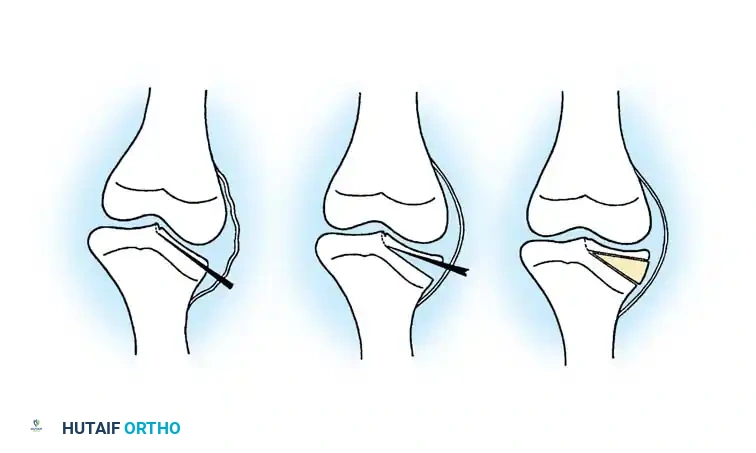
1. Rab's Oblique Osteotomy: A single-plane oblique cut that allows simultaneous correction of varus and internal rotation. It permits postoperative cast wedging if necessary to fine-tune the alignment.
2. Laurencin's Incomplete Closing Wedge: Designed to avoid neurovascular and physeal complications, this oblique incomplete closing wedge osteotomy is fixed with a lateral tension band plate.
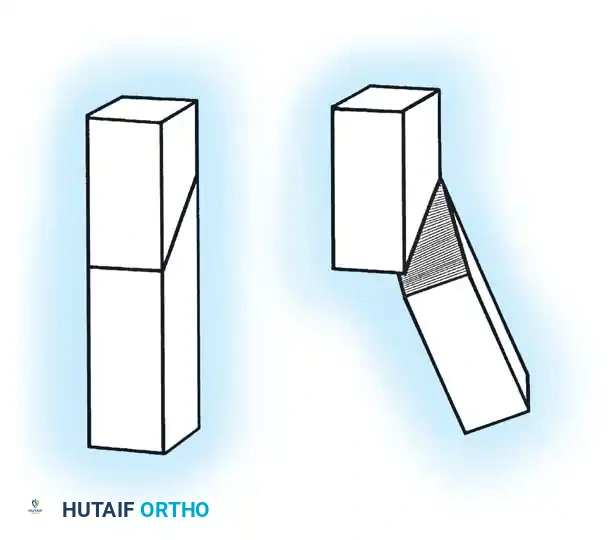
3. Greene's Chevron Osteotomy: Utilizes a crescent-shaped or chevron cut where a lateral closing wedge is harvested and inserted medially as an opening wedge. This maintains limb length, which is critical in moderate to severe tibia vara.
Step-by-Step Surgical Technique (Proximal Tibial Osteotomy)
- Positioning and Preparation: The patient is positioned supine on a radiolucent table. A tourniquet is applied to the proximal thigh. Fluoroscopy must be available to visualize the mechanical axis from the center of the femoral head to the center of the ankle mortise.
- Fibular Osteotomy: A fibular osteotomy is mandatory to allow tibial correction. This is typically performed in the middle third of the fibula to avoid the common peroneal nerve proximally and the distal tibiofibular syndesmosis distally. An oblique cut is made to allow sliding.
- Tibial Exposure: A transverse or longitudinal incision is made over the proximal tibia, distal to the tibial tubercle to avoid the apophysis. The anterior compartment musculature is elevated laterally.
- Osteotomy Execution: Guide pins are placed under fluoroscopic guidance to define the osteotomy plane. The cut is made distal to the tibial tubercle to ensure the extensor mechanism remains attached to the proximal fragment.
- Deformity Correction: The distal fragment is translated laterally, angulated into valgus, and externally rotated to correct the multiplanar deformity.
- Fixation: Fixation depends on surgeon preference and patient age. Options include crossed Kirschner wires incorporated into a long-leg cast, rigid internal fixation (plates and screws), or external fixation (Ilizarov or Taylor Spatial Frame), which allows for gradual postoperative correction.

Management of Physeal Bars
A primary cause of recurrence after osteotomy is the presence of an undiagnosed medial physeal bar. Greene established criteria for preoperative tomographic (or MRI) evaluation to rule out a bony bar:
1. Age older than 5 years.
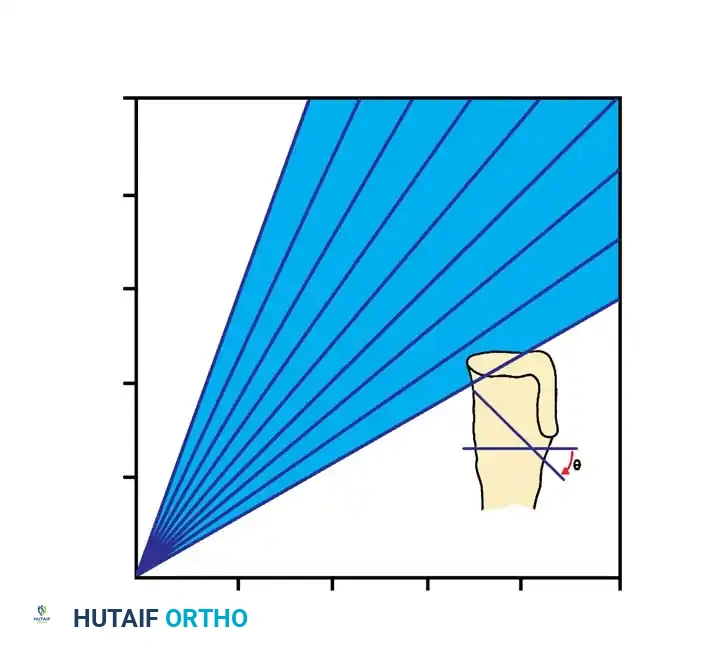
2. Medial physeal slope of 50 to 70 degrees.
3. Langenskiöld grade IV radiographic changes.
4. Body weight greater than the 95th percentile.
5. Black girls meeting the previous criteria.
If a bony bridge is present and the child has remaining growth potential, bony bridge resection (epiphyseolysis) with interposition of fat or cranioplast should be performed in conjunction with the tibial osteotomy. Medial physeal bar resection alone is insufficient if significant angular deformity already exists.
Guided Growth (Hemiepiphysiodesis)
In children older than 9 years with less severe involvement, lateral tibial epiphysiodesis (with or without fibular epiphysiodesis) can be utilized. Westberry et al. demonstrated that hemiepiphysiodesis in adolescent tibia vara successfully improves or maintains the deformity in 87.8% of patients, potentially preventing the need for morbid osteotomies. Tension-band plating (e.g., eight-Plates) across the lateral physis gradually corrects the varus angulation through asymmetric growth.
Advanced Disease: Intraepiphyseal Osteotomy and Medial Plateau Elevation
For older patients with severe, neglected deformities (Langenskiöld grades V and VI) where bracing and standard osteotomies have failed, the joint line is severely distorted. The medial femoral condyle sinks into a profound epiphyseal defect, causing severe joint instability.
In these advanced cases, a standard metaphyseal osteotomy will correct the mechanical axis but will leave the joint line unacceptably oblique, leading to early osteoarthritis.
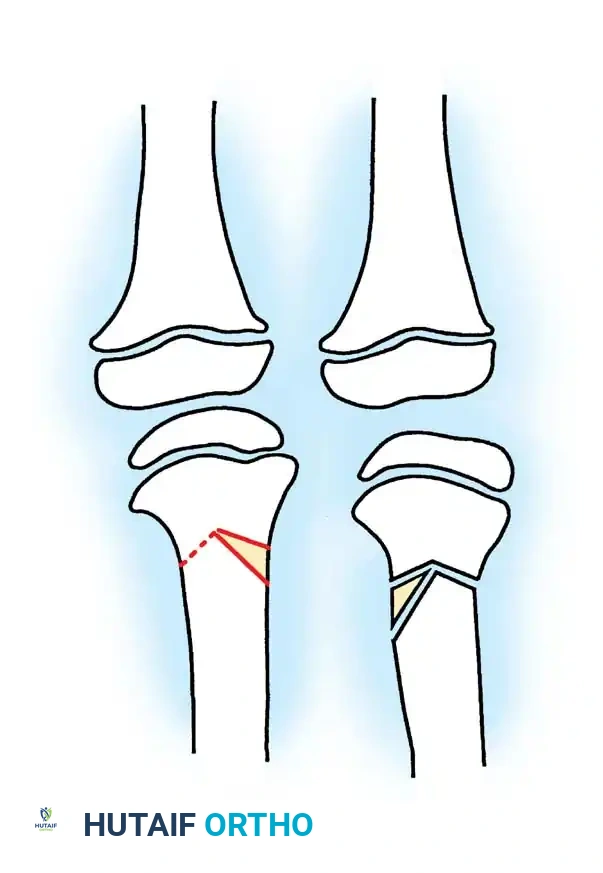
Therefore, a double-elevating osteotomy is required:
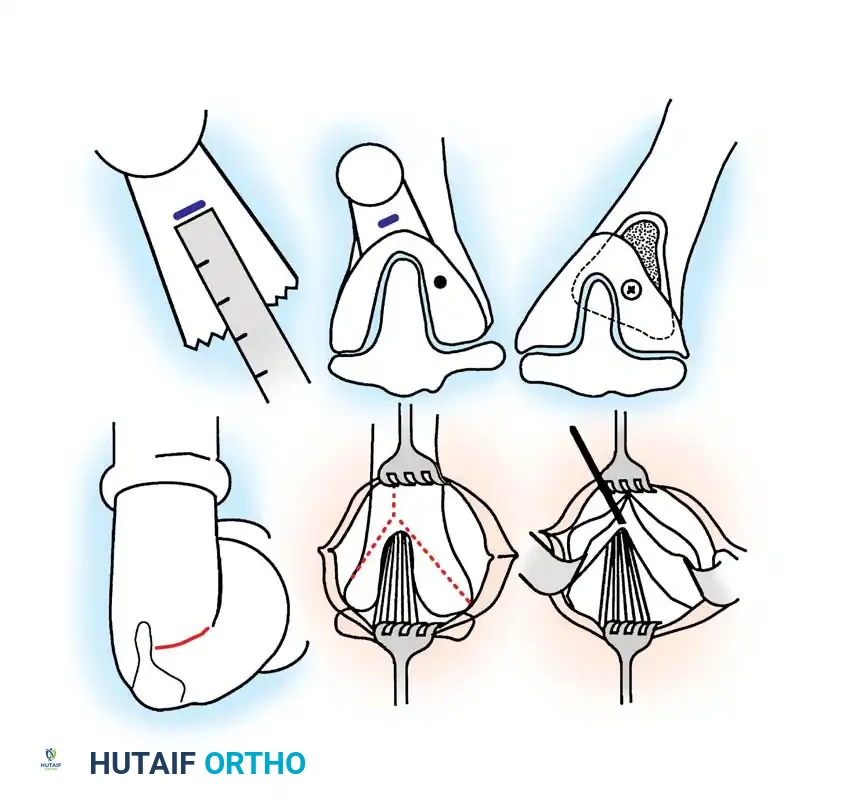
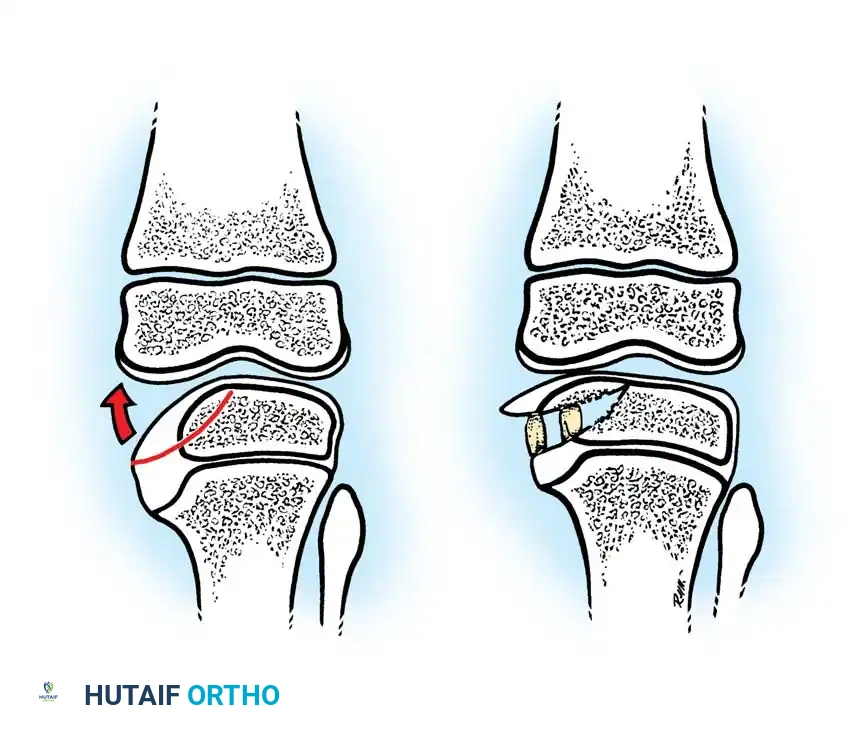
1. Intraepiphyseal Osteotomy: To elevate the depressed medial tibial plateau and reconstruct the horizontal joint line.
2. Metaphyseal Valgus Osteotomy: To correct the diaphyseal varus angulation.

Schoenecker et al. reported successful elevation of the medial tibial plateau in patients aged 10 to 13 years with average preoperative varus deformities of 25 degrees. The procedure involves an osteotomy through the epiphysis, elevating the medial plateau to match the lateral plateau, and supporting the elevation with structural bone graft.

Surgical Warning: Intraepiphyseal osteotomies carry a high risk of intra-articular fracture, avascular necrosis of the elevated fragment, and permanent physeal arrest. Meticulous fluoroscopic guidance and rigid fixation are absolute requirements.
Postoperative Protocol and Complications
Postoperative management is dictated by the stability of the fixation.
* Cast Fixation: If pins-in-plaster are used, the patient is placed in a non-weight-bearing long-leg cast for 6 to 8 weeks. Cast wedging may be performed at 2 weeks to optimize alignment.
* Internal Fixation: Patients with rigid plate fixation may begin early range of motion but remain non-weight-bearing until radiographic union is evident (typically 6-8 weeks).
* External Fixation: Pin site care is paramount. Gradual correction protocols begin 7-10 days postoperatively. Weight-bearing is often permitted as tolerated to stimulate bone healing.
Complications:
* Recurrence: The most common complication, particularly in children operated on after age 5 or those with unrecognized physeal bars.
* Neurovascular Injury: The common peroneal nerve is at risk during fibular osteotomy and during acute valgus correction. Prophylactic anterior compartment fasciotomy should be considered to prevent compartment syndrome.
* Overcorrection/Undercorrection: Precise preoperative planning and intraoperative mechanical axis assessment are required to prevent residual deformity.
* Leg Length Discrepancy: Unilateral disease and subsequent physeal arrest can lead to significant limb length inequalities, necessitating contralateral epiphysiodesis or ipsilateral lengthening procedures near skeletal maturity.
📚 Medical References
- Accadbled F, Laville J-M, Harper L: One-step treatment for evolved Blount’s disease, J Pediatr Orthop 23:747, 2003.
- Alekberov C, Shevtsov VI, Karatosun V, et al: Treatment of tibia vara by the Ilizarov method, Clin Orthop Relat Res 409:199, 2003.
- Arai K, Haga N, Taniguchi K, et al: Magnetic resonance imaging fi ndings and treatment outcome in late-onset tibia vara, J Pediatr Orthop 21:808, 2001.
- Auerbach JD, Radomisli TE, Simoncini J, et al: Variability of the metaphyseal-diaphyseal angle in tibia vara: a comparison of two methods, J Pediatr Orthop 24:75, 2004.
- Beaty JH, Coscia MF, Holt M: Blount’s disease. Paper presented at the Fifth Annual Meeting of the Southern Orthopedic Association, Edinburgh, Aug 4, 1988.
- Beck CL, Burke SW, Roberts JM, et al: Physeal bridge resection in infantile Blount disease, J Pediatr Orthop 7:161, 1987.
- Bell DF: Treatment of adolescent Blount’s disease using the Ilizarov technique, Op Tech Orthop 3:149, 1993.
- Blount WP: Tibia vara: osteochondrosis deformans tibiae, J Bone Joint Surg 19:1, 1937.
- Bradway JK, Klassen RA, Peterson HA: Blount disease: a review of the English literature, J Pediatr Orthop 7:471, 1987.
- Bright RW: Operative correction of partial epiphyseal plate closure by osseous-bridge resection and silicone-rubber implant, J Bone Joint Surg 56A:655, 1974.
- Canale ST, Harper MC: Biotrigonometric analysis and practical applications of osteotomies of tibia in children, Instr Course Lect 30:85, 1981.
- Carter JR, Leeson MC, Thompson GH, et al: Late-onset tibia vara: a histopathologic analysis: a comparative evaluation with infantile tibia vara and slipped capital femoral epiphysis, J Pediatr Orthop 8:187, 1988.
- Coogan PG, Fox JA, Fitch RD: Treatment of adolescent Blount disease with the circular external fi xation device and distraction osteogenesis, J Pediatr Orthop 16:450, 1996.
- Dalinka MK, Coren G, Hensinger R, et al: Arthrography in Blount’s disease, Radiology 113:161, 1974.
- De Palblos J, Azcarate J, Barrios C: Progressive opening-wedge osteotomy for angular long-bone deformities in adolescents, J Bone Joint Surg 77B:387, 1995.
- Eggert P, Viemann M: Physiological bowlegs or infantile Blount’s disease: some new aspects on an old problem, Pediatr Radiol 26:349, 1996.
- Erlacher P: Deformierended prozesse der Epiphysengegend bei Kindern, Arch Orthop Unfallchir 20:81, 1922.
- Feldman DS, Madan SS, Koval KK, et al: Correction of tibia vara with six-axis deformity analysis and the Taylor spatial frame, J Pediatr Orthop 23:387, 2003.
- Ferriter P, Shapiro F: Infantile tibia vara: factors affecting outcome following proximal tibial osteotomy, J Pediatr Orthop 7:1, 1987.
- Foreman KA, Robertson WW Jr: Radiographic measurement of infantile tibia vara, J Pediatr Orthop 5:452, 1985.
- Gaudinez R, Adar U: Use of the Orthofi x T-Garche fi xator in the late-onset tibia vara, J Pediatr Orthop 16:455, 1996.
- Greene WB: Infantile tibia vara, J Bone Joint Surg 75A:130, 1993.
- Gregosiewicz A, Wosko I, Kandzierski G, et al: Double-elevating osteotomy of tibiae in the treatment of severe cases of Blount’s disease, J Pediatr Orthop 9:178, 1989.
- Hayek S, Segev E, Ezra E, et al: Results using a new technique for the correction of infantile tibia vara, J Bone Joint Surg 82B:1026, 2000.
- Henderson RC, Kemp GJ Jr, Greene WB: Adolescent tibia vara: alternatives for operative treatment, J Bone Joint Surg 74A:342, 1992.
- Herring JA, Ehrlich MG: Instructional case: valgus knee deformity—etiology and treatment, J Pediatr Orthop 3:527, 1983.
- Herring JA, Wenger DR: Blount disease, J Pediatr Orthop 7:601, 1987.
You Might Also Like


