Comprehensive Management of Pediatric Femoral Fractures
Key Takeaway
Pediatric femoral fractures require age-specific management strategies, ranging from Pavlik harnesses in infants to rigid intramedullary nailing in adolescents. Treatment decisions hinge on fracture location, biomechanical deforming forces, and patient weight. This guide provides a comprehensive, evidence-based approach to non-operative and operative techniques, including spica casting, elastic stable intramedullary nailing (ESIN), and external fixation, ensuring optimal alignment and minimizing complications like refracture or limb-length discrepancy.
EPIDEMIOLOGY AND ETIOLOGY OF FEMORAL FRACTURES
Fractures of the femur are major orthopaedic injuries that require meticulous assessment and age-specific management. They are anatomically classified by location: subtrochanteric, diaphyseal (proximal, middle, and distal thirds), supracondylar, and distal femoral physeal. The middle third of the diaphysis is the most frequent site of injury.
According to Hinton et al., the annual incidence of pediatric femoral shaft fractures is 19.15 per 100,000. The age distribution is distinctly bimodal, demonstrating peak incidences at 2 years and 17 years of age. Demographically, males sustain these fractures at higher rates than females across all age groups, and adverse socioeconomic conditions demonstrate a statistically significant correlation with increased fracture rates.
The primary mechanisms of injury are highly age-dependent:
* Children < 6 years: Low-energy falls.
* Children 6 to 9 years: Motor vehicle-pedestrian accidents.
* Teenagers: High-energy motor vehicle collisions and sports trauma.
Non-Accidental Trauma (Child Abuse)
In the infant and toddler populations, non-accidental trauma must be at the forefront of the differential diagnosis. Kasser noted that 30% of femoral fractures in children younger than 4 years old are attributable to child abuse. Alarmingly, in children younger than 1 year of age, 70% of femoral fractures are abuse-related.
Clinical Pearl: Red Flags for Non-Accidental Trauma
Abuse must be highly suspected if any of the following are present: (1) an unreasonable or inconsistent history, (2) an inappropriate delay in seeking medical care, (3) a previous history of abuse, (4) radiographic evidence of other fractures in various stages of healing, (5) multiple acute fractures, and (6) characteristic fracture patterns (e.g., corner fractures, posterior rib fractures) in non-ambulatory infants.
Associated Injuries
A femoral fracture represents a massive transfer of kinetic energy. If a child sustains sufficient trauma to fracture the largest bone in the body, occult abdominal, thoracic, or closed head injuries may be present. Furthermore, examination of the ipsilateral knee is mandatory; Robertson et al. reported that ligamentous instability or meniscal pathology occurs in up to 4% of children with femoral fractures.
BIOMECHANICS AND DEFORMING FORCES
Understanding the muscular anatomy of the thigh is critical for achieving and maintaining fracture reduction, whether via closed traction or operative fixation. The displacement of femoral fragments is dictated by the unopposed pull of regional musculature.
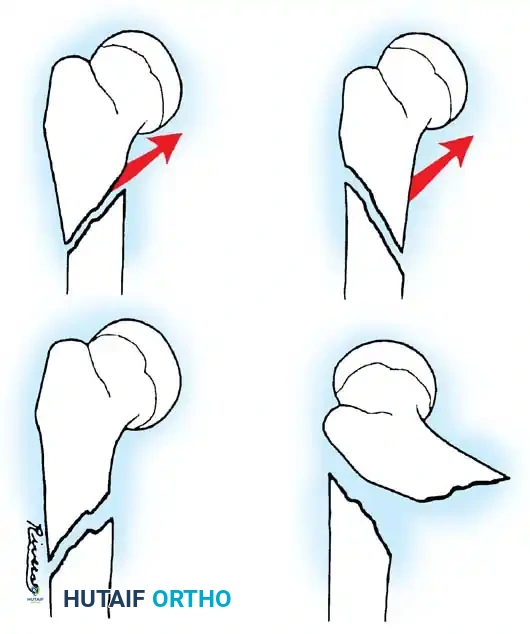
- Proximal Shaft and Subtrochanteric Fractures: The proximal fragment is typically driven into flexion, abduction, and external rotation. This is due to the unopposed pull of the iliopsoas (flexion), the gluteus medius and minimus (abduction), and the short external rotators.
- Midshaft Fractures: The adductors and extensors remain intact. The distal fragment is usually in satisfactory alignment, albeit with a tendency toward external rotation and proximal migration (shortening) due to the adductor magnus and quadriceps.
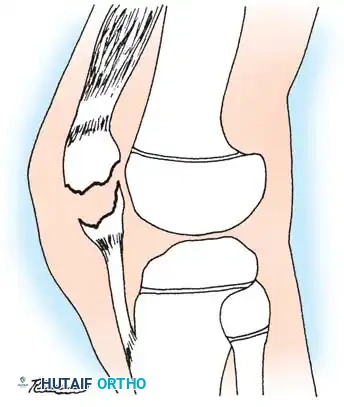
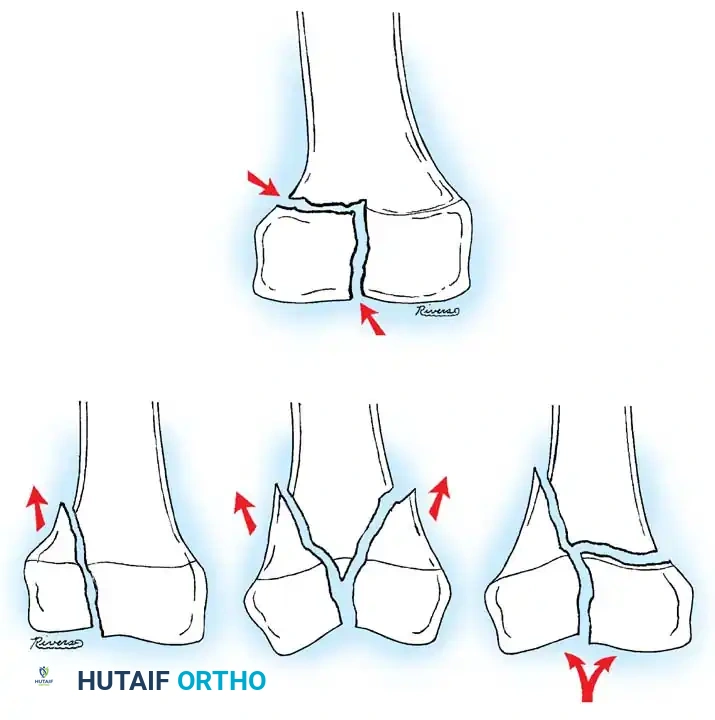
- Supracondylar Fractures: The distal fragment is pulled into hyperextension due to the strong origin of the gastrocnemius muscle on the posterior femoral condyles.
Fig. 33-146: Subtrochanteric fracture stability. (A) If the proximal spike of bone is posterior, the fracture is often stable against the distal fragment. (B) Conversely, if the proximal spike is anterior, the fracture is highly unstable, and 90-90 traction or operative fixation is necessary to counteract the flexion force of the iliopsoas.
AGE-BASED TREATMENT ALGORITHMS
The management of pediatric femoral fractures has evolved significantly over the past decade. As noted by Carey and Galpin, there has been a paradigm shift toward operative approaches. This shift is driven by the desire for rapid mobilization, reintegration into school, and the recognition that prolonged immobilization yields negative psychological and physiological effects. Economic pressures and hospital length-of-stay metrics also favor operative intervention in appropriate candidates.
Staheli defined the ideal treatment as one that controls alignment and length, is comfortable for the child, convenient for the family, and minimizes psychological impact. The consensus among pediatric orthopaedists, supported by Sanders et al., is that treatment must be strictly age-dependent.
General Treatment Guidelines
- Age < 1 Year:
- Preferred: Pavlik harness.
- Alternate: Early spica casting.
- Age 1 to 6 Years:
- Preferred: Early spica casting.
- Alternate: Traction followed by spica casting (for length-unstable fractures).
- Age 6 to 13 Years:
- Preferred: Elastic Stable Intramedullary Nailing (ESIN).
- Alternate: Submuscular locking plate, external fixation (for open/comminuted fractures).
- Age 15 to Adult:
- Preferred: Rigid Intramedullary (IM) nail (>8 mm).
- Alternate: Locking compression plate.
Surgical Warning: Open Fractures
Regardless of age, open fractures of the femoral diaphysis require emergent irrigation and debridement. External fixation remains a highly reliable primary or provisional stabilization method across all age groups for severe open injuries.
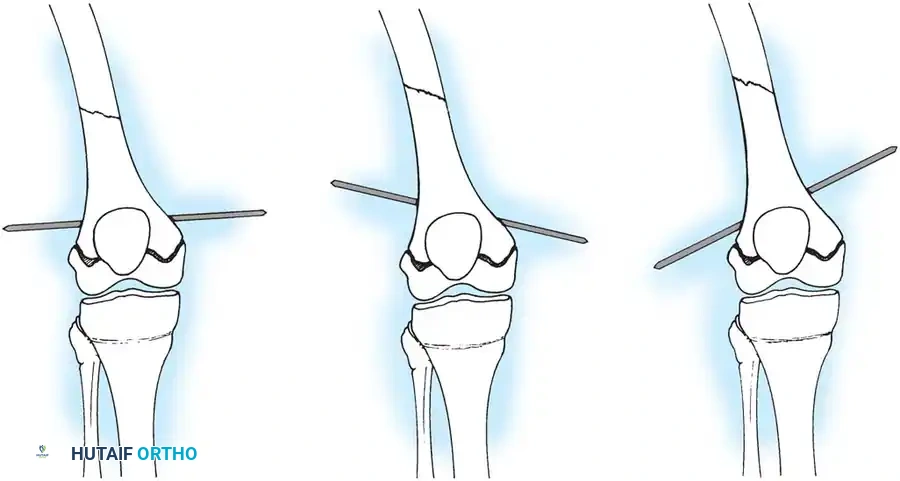
Fig. 33-147: Position of the skeletal traction pin. The optimal position is horizontal. Oblique pins induce varus or valgus malalignment reflecting the resultant pull of the traction bow.
NON-OPERATIVE MANAGEMENT: TRACTION AND SPICA CASTING
While operative fixation is increasing, closed management remains the gold standard for toddlers and preschool-aged children (1 to 6 years).
Traction Techniques
At our institution, skin or skeletal traction is utilized in children younger than 6 years old depending on the child's size and fracture morphology.
* Skin Traction: Limited to children weighing less than 15 kg. Overhead skin traction should be avoided due to the high risk of neurovascular compromise.
* Skeletal Traction: For children 6 to 10 years old (or larger toddlers), a 5/64-inch Steinmann pin is inserted into the proximal tibia or distal femur.
* Tibial Pin: Must be placed distal to the tibial tubercle and proximal tibial physis to prevent iatrogenic genu recurvatum.
* Femoral Pin: Reserved for distal supracondylar fractures (to counteract posterior angulation) or 90-90 traction in proximal fractures. Never use a distal femoral pin if subsequent intramedullary nailing is planned, as the pin tract can serve as a nidus for deep intramedullary infection.
Peroneal nerve palsy is a rare but documented complication of traction. Weiss et al. reported a 3.6% incidence in patients treated with 90-90 traction. Frequent neurovascular checks are mandatory.

Radiographic evaluation of a pediatric femur fracture managed in a spica cast, demonstrating acceptable alignment and early callus formation.
Technique 33-37: Spica Cast Application
- Preparation: Under general anesthesia, remove the skeletal traction pin and sterilely dress the wound sites.
- Positioning: Place the child on a pediatric spica table (image box). Ensure the sacrum is well-supported.
- Padding: Apply Gore-Tex or standard cast padding. Protect the bony prominences (ASIS, sacrum, heels).
- Leg Positioning: Flex the knee 50 to 90 degrees (depending on age and fracture stability) to relax the gastrocnemius and control rotation. Flex the hip to match the proximal fragment (often 45-60 degrees of flexion, 30 degrees of abduction, and 15 degrees of external rotation).
- Casting: Apply a short leg cast first to control the foot and ankle, then extend to a long leg cast, and finally incorporate the pelvis and contralateral thigh (1.5 spica).
- Molding: Mold the proximal thigh anteriorly and laterally to prevent the common apex-anterior and apex-lateral bowing.
OPERATIVE MANAGEMENT
Elastic Stable Intramedullary Nailing (ESIN)
For children aged 6 to 13 years, ESIN (using titanium or stainless steel Nancy/Ender nails) is the treatment of choice for length-stable transverse or short oblique diaphyseal fractures.
Biomechanics of ESIN:
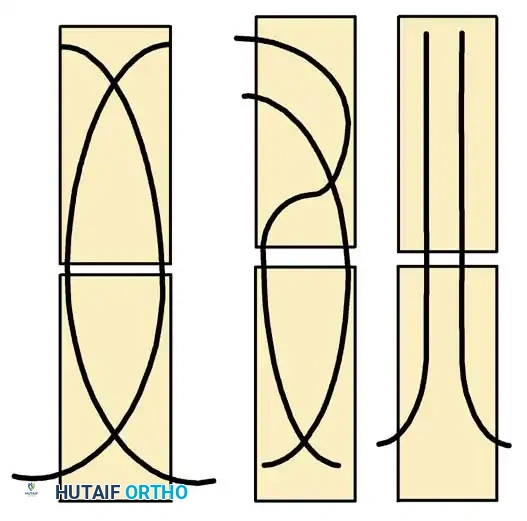
ESIN relies on the principle of symmetric, three-point fixation. Two pre-bent elastic nails are inserted (usually retrograde from the distal femur) and advanced across the fracture site. The restorative forces of the bent elastic nails pushing against the inner cortical walls provide rotational and angular stability while allowing micromotion that stimulates robust secondary bone healing (callus formation).

Biomechanical principles of Elastic Stable Intramedullary Nailing (ESIN), demonstrating the three-point cortical contact required for stability.

Intraoperative fluoroscopy demonstrating the retrograde insertion of elastic nails through the distal femoral metaphysis.
Surgical Technique:
1. Nail Selection: The diameter of each nail should be 40% of the narrowest diaphyseal medullary canal diameter. The combined diameter of both nails should fill 80% of the canal.
2. Entry Points: Medial and lateral incisions are made 2.5 cm proximal to the distal femoral physis.
3. Insertion: The nails are pre-bent to an apex that will sit exactly at the fracture site. They are advanced sequentially to the fracture.
4. Reduction and Crossing: The fracture is reduced closed. The nails are advanced across the fracture into the proximal metaphysis. Crucially, the nails must cross above or below the fracture site, never exactly at the fracture level, to maintain stability.
5. Final Seating: The nails are driven into the proximal femoral metaphysis, with the lateral nail terminating near the greater trochanter and the medial nail near the lesser trochanter.

Fluoroscopic view showing the elastic nails crossing in the diaphysis, ensuring symmetric construct rigidity.

Final seating of the elastic nails in the proximal femur. Note the divergent tips anchoring in the cancellous bone of the metaphysis.

Postoperative AP radiograph demonstrating excellent alignment and appropriate nail sizing.

Postoperative lateral radiograph confirming restoration of the anatomic anterior bow of the femur.

Follow-up radiograph at 6 weeks demonstrating robust, symmetric bridging callus typical of the relative stability provided by ESIN.
Rigid Intramedullary Nailing
In adolescents (typically >13 years or >50 kg), the medullary canal is large enough, and the physis is mature enough, to accept a rigid, locked intramedullary nail.
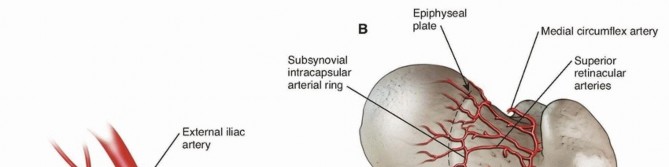
Pitfall: Avascular Necrosis (AVN) of the Femoral Head
In skeletally immature patients, a piriformis fossa entry point is strictly contraindicated due to the high risk of iatrogenic damage to the medial femoral circumflex artery, leading to AVN. A lateral trochanteric entry point must be utilized.

Intraoperative fluoroscopy demonstrating a lateral trochanteric entry point for rigid intramedullary nailing, avoiding the piriformis fossa.
Distal interlocking screws placed to control rotation and maintain length in a comminuted adolescent femur fracture.
Proximal interlocking of the rigid intramedullary nail.
Postoperative AP radiograph of a rigidly nailed adolescent femur fracture.
Postoperative lateral radiograph demonstrating anatomic alignment and secure fixation.
Submuscular Plating (Locked Plating)
For length-unstable fractures (spiral, highly comminuted) in the 6 to 13-year age group where ESIN would fail to maintain length, submuscular locked plating is highly effective. A locking compression plate is slid submuscularly via a minimally invasive distal or proximal incision, bridging the fracture zone without disturbing the fracture hematoma.
Submuscular bridge plating of a comminuted pediatric femur fracture. This technique preserves the fracture biology while providing absolute length and rotational control.
External Fixation
External fixation is indicated for polytrauma patients (damage control orthopaedics), severe open fractures, or highly comminuted fractures where internal fixation is contraindicated.
While effective, external fixation carries a high complication profile. Gregory et al. reported a 30% major complication rate, including pin track infections and refractures.
The Refracture Risk:
Skaggs et al. identified a 12% secondary fracture rate after fixator removal. The critical variable is the amount of bridging callus. Fractures showing fewer than three cortices of bridging callus on orthogonal radiographs at the time of frame removal had a 33% refracture rate, whereas those with three or four cortices had only a 4% rate.
DISTAL FEMORAL PHYSEAL AND SUPRACONDYLAR FRACTURES
Fractures involving the distal femoral physis (Salter-Harris types) or the supracondylar region require distinct management. The distal femoral physis contributes 70% of the growth of the femur and 40% of the overall growth of the lower extremity. Consequently, anatomic reduction is paramount to minimize the risk of premature physeal closure and subsequent limb-length discrepancy or angular deformity.

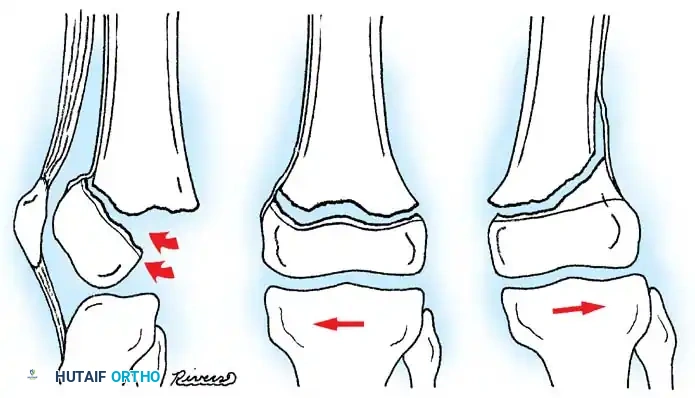
AP radiograph demonstrating a displaced Salter-Harris II fracture of the distal femur.

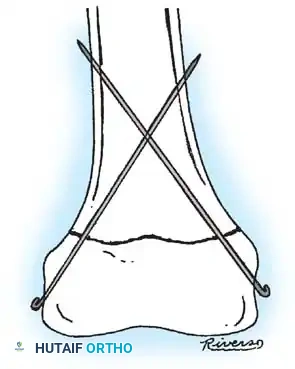
Intraoperative fluoroscopy showing smooth Kirschner wire fixation crossing the physis to stabilize a Salter-Harris fracture.

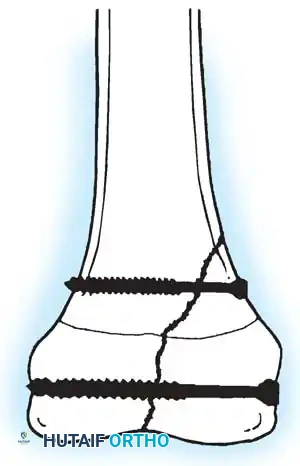
Cannulated screw fixation of a distal femoral epiphyseal/metaphyseal injury, ensuring the threads do not cross the open physis.
REMODELING AND LONG-TERM OUTCOMES
The pediatric femur possesses a remarkable capacity for remodeling, which dictates acceptable reduction parameters.
Overgrowth
Femoral overgrowth is a well-documented phenomenon following diaphyseal fractures in children aged 2 to 10 years, driven by fracture hyperemia stimulating the physes. Historically, surgeons intentionally allowed 1 to 2 cm of overriding (shortening) in spica casts to compensate for this. However, Hedin et al. noted that in externally fixed fractures, mean overgrowth was only 0.5 cm and did not correlate with the healed position. Modern consensus suggests reducing the fracture to anatomic length, as clinically significant overgrowth (>2 cm) is rare.
Rotational and Angular Remodeling
If alignment and length are maintained, mild malrotation usually corrects with growth. Strong et al. demonstrated in animal models that an average of 55% of rotational remodeling occurs spontaneously.
Angular deformities remodel robustly in the sagittal plane (flexion/extension) and moderately in the coronal plane (varus/valgus). Wallace and Hoffman reported an average 85% correction in children who had angular deformities of 10 to 26 degrees. They concluded that in children younger than 13 years of age, malunion of up to 25 degrees in any plane will remodel sufficiently to yield normal joint surface alignment.
CONCLUSION
The management of pediatric femoral fractures demands a nuanced, age-specific approach. While non-operative management with spica casting remains a cornerstone for toddlers, the modern orthopaedic surgeon must
📚 Medical References
You Might Also Like